
Hip disarticulation is a viable procedure for preventing further morbidity in patients with refractory prosthetic joint infection and peripheral arterial disease.
Dr. Anderson Lee, Department of Orthopaedic Surgery, University of Toledo, 3000 Arlington Ave, Toledo 43614, Ohio. E-mail: anderson.lee@rockets.utoledo.edu
Abstract
Introduction: The aim of this study was to report a patient with refractory prosthetic joint infection (PJI) and severe peripheral arterial disease that necessitated hip disarticulation (HD), a rare and aggressive procedure. While this is not the first HD performed due to PJI, this is the first reported incidence that deals with profound infection burden along with immense vascular disease that has failed all other treatment options.
Case Report: We report a case of an elderly patient with a prior history of the left total hip arthroplasty, PJI, and severe peripheral arterial disease who underwent a rare HD procedure and was discharged with minimal complications. Before this major surgery, several surgical revisions and antibiotic regimens were attempted. The patient had also failed a revascularization procedure to treat an occlusion stemming from the peripheral arterial disease and had developed a necrotic wound at the surgical site. Irrigation and debridement of associated necrotic tissue was unsuccessful and due to concerns such as cellulitis, HD was performed with patient consent.
Conclusion: HD is a rare procedure that comprises only 1–3% of all lower limb amputations and is reserved for extremely deleterious indications such as infection, ischemia, and trauma. Complication and 5 year mortality rates have been reported to be as high as 60% and 55%, respectively. Despite these rates, the patient case illustrates a situation, in which early detection of indications for HD prevented further negative outcomes. Based on this case, we believe that HD is a reasonable treatment of choice in patients with severe peripheral arterial disease who fail revascularization and prior moderate treatment options. However, the limited availability of data involving HD and variety of comorbid conditions necessitate further analysis in terms of outcomes.
Keywords: Total hip arthroplasty, joint infection, disarticulation, peripheral arterial disease, arterial occlusive diseases.
An important complication that must be contemplated before and total hip arthroplasty (THA) is prosthetic joint infection (PJI). Before surgery, considering PJI as one of the major complications can inform clinical decision on what type of surgical approach (anterior vs. lateral/posterior) to use as there are slight differences in complication risks [1]. Following THA, diagnostic factors including positive cultures, purulence, and immune cell levels are some of the many factors that can lead to a highly sensitive diagnosis of PJI and help guide therapeutic plan [2]. Any delay in identifying the microorganisms responsible and beginning treatment can lead to persistence of infection, pain, decreased mobility or disability, and serious extra-articular complications. Although there are many variations in treatment protocol depending on the acute or chronic nature of the PJI, revision surgeries with antibiotic spacers, suppressive antibiotic therapy, and prosthetic debridement are common steps [3]. The presence of accompanying peripheral arterial disease in the same limb can further exacerbate the condition by increasing the risk for ischemia and necrosis. Here, we have presented a case of hip disarticulation (HD) in an elderly patient with prior THA who exhibited multiple recurrences of joint infections and symptoms stemming from peripheral arterial disease.
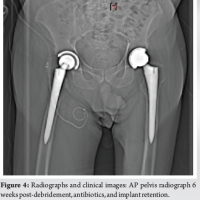
The patient is a 74-year-old male who presented to our institution for evaluation of his left leg with a history of the left hip THA 14 years prior. He subsequently underwent seven surgeries on his left hip and knee due to three episodes of PJI, a fall resulting in a periprosthetic femur fracture, and complications with the implants (loosening and limb-length discrepancy). The PJIs were treated with chronic antibiotic use as well as two-step revisions with antibiotic spacer placement, with the most recent surgery being a stage I revision with antibiotic spacer placement. The patient also had a history of liposarcoma removal and hypertension, with chronic left lower extremity edema. Five years before the current episode, he was diagnosed with peripheral arterial disease of the left lower extremity. A few months ago, he presented with resting left lower extremity pain and CT angiography showed occlusion of the common left iliac artery. A right femoral to the left popliteal bypass surgery was performed, but the bypass surgical site had become necrotic, indicating failed revascularization. X-ray imaging of the left lower extremity revealed displacement of his hip hardware components with cortical irregularities of the proximal femur and acetabulum which suggested healing fractures or chronic infection (Fig. 1). Physical examination of the patient revealed a 10 cm × 5 cm black, necrotic wound on the medial side of his left lower extremity, mixed with vital pink tissue, and purulent material. His left lower extremity was more edematous compared to the right side. Capillary refill in his left leg was slow and his dorsalis pedis pulse was unable to be palpated. He had diminished sensation in his superficial peroneal, deep peroneal, sural, saphenous, and tibial nerve distributions of the left lower extremity though he indicated that this was his baseline. Active range of motion was limited significantly due to displacement of his antibiotic spacer. The patient and his family inquired about a HD of his left lower extremity and after an extensive discussion with the orthopedic team about the risks and benefits of this major operation; it was decided that he would undergo an irrigation and debridement of the non-healing wound 2 days later. This procedure was uneventful, and the patient was discharged but returned to the emergency department (ED) 8 days later with concerns of cellulitis with increasing redness and blackness of his wound. After discussion of his treatment options and explanation of the risks and benefits, the patient consented to HD of his left lower extremity. Vascular surgery was consulted and agreed with the treatment as well as being present for the operation should any complications arise. Pre-operative testing and assessment of his nutritional status were performed. The patient was taken to the operating room 4 days later after admission to the ED where he received general anesthesia and was placed in the floppy lateral position. Prophylactic antibiotics were given before incision. The left lower extremity was prepped and draped in standard sterile fashion, and a classic tennis racquet style incision was made through the skin down the medial and lateral aspects of the proposed flaps. Electrocautery was used to extend the incision down to the level of the fascia. Once it was determined that there was adequate soft-tissue elevation across the entirety of the anterior aspect of the thigh, the posterior flaps were made. Electrocautery was once again used to dissect down to the level of the muscular fascia circumferentially around the thigh, and the sciatic nerve was transected. The electrocautery was then used to elevate the soft-tissues off the bone with care to leave a thick medial cuff of tissue which likely contained all of the vessels. Once dissection had reached the level of the prosthesis, it was split using an osteotome and completely removed. The entirety of the THA including cement fragments was removed. At this point, a large seroma was encountered and cultures were obtained. Following this, a combination of electrocautery and silk ties were used to dissect the medial bundle and the collateral vessels. After all of the soft-tissue of the medial bundle was released, the leg was able to be removed at the level of the hip. The wound was copiously irrigated and appropriately closed with placement of a wound VAC. He was monitored over the next few days and did well postoperatively without any fever, chills, numbness, or tingling of his stump end. The patient was eventually discharged 8 days postoperatively. Subsequent X-rays at 2 months follow-up demonstrated complete removal of the left femoral prosthesis (Fig. 2).
Peripheral arterial disease is narrowing or occlusion of antegrade blood flow in major arteries outside of those involved in coronary and cerebral blood flow. Treatment involves modifying lifestyle habits, avoiding risk factors such as smoking, and pharmacologic therapies to reduce risk of cardiovascular events [4]. Peripheral arterial disease may progress to limb ischemia, in which patients develop pain at rest, ulceration, and possibly tissue necrosis. The Rutherford classification of peripheral arterial disease includes seven stages that describe specific criteria for progression and severity of this condition (0 – asymptomatic, 6 – ulceration or gangrene present) [5]. Limb ischemia may threaten limb viability, thereby requiring patients to undergo revascularization techniques or oftentimes amputations in nearly 25% of cases of chronic limb ischemia within 12 months of diagnosis [4]. PJI is a serious complication of arthroplasty procedures, occurring in 1–2% of primary arthroplasties and 4% of revision arthroplasties [3]. Major challenges in the management of this are the persistence of microorganism infection on the implant, often requiring debridement or exchange of prosthesis parts. Aside from death, amputation is the most significant and worst outcome for a total joint arthroplasty procedure. Peripheral vascular disease has historically been the leading cause of lower extremity amputations, while amputations due to peri-PJI s have seen an uptick in incidence since 1998 [6]. HD, or amputation of the lower limb through the hip joint, is a radical and rare procedure that is considered a last-resort operation for life-threatening complications or circumstances with high rates of morbidity and mortality. It accounts for around only 0.5% of lower extremity amputations within the United States and its most common indications include severe trauma, necrotizing fasciitis, infection, ischemia, and malignant musculoskeletal tumors [7,8]. Between three different studies discussing the rates and indications of HD, five out of 35 patients underwent HD as a result of severe peripheral vascular disease. Twenty-four of these procedures were performed electively [7,8,9]. The mortality rate was 4% in patients who underwent the procedure electively compared to 33% when performed emergently [9]. In this case, the patient had long-standing peripheral arterial disease as well as prior chronic peri-PJI and had failed revascularization, resulting in a sizable necrotic wound and further complications even after irrigation and debridement. The absence of successful revascularization in patients with critical limb ischemia results in amputation up to 40% of the time with mortality rates exceeding 20.3% [10]. HD is a procedure for PJIs that are found to be more likely in patients with concomitant peripheral vascular disease or diabetes. One study evaluated seven of these procedures that were performed due to emergent indications and concluded that the procedure was associated with a low mortality rate [6]. HD became the elective treatment of choice due to the patient’s risk for further infection and necrosis. With such high reported mortality rates in patients with refractory peripheral arterial disease, it was decided that the best option for his subsequent quality of life and survival was HD. The procedure itself was met with minimal complications as it was discovered intraoperatively that the majority of the vessels within his amputated extremity had become occluded. In this patient’s case, he recovered well postoperatively and was in minimal pain by the time he was discharged from the hospital.
This patient case demonstrates that while any form of amputation or disarticulation remains as a last resort for treatment, HD in the setting of refractory PJI with immense amount of osteomyelitis present in the setting of profound vascular disease who has failed revascularization is a viable option not only for treatment but also for overall patient satisfaction. Due to the level of the patient’s soft-tissue infection and persistent hip infection, HD was the only option as above knee amputation would have provided inadequate stump creation, tolerance for prothesis, and eradication of joint infection, making HD a reasonable option to address both the orthopedic and vascular issues that were refractory to other interventions. The authors of this study believe HD can offer patients a salvage intervention for patients that present with complex medical and orthopedic issues to provide better patient satisfaction and decreased morbidity.
HD is a rare and drastic procedure that does not come without risks of complications and mortality. Indications for this procedure must be carefully considered and in cases like this can have a beneficial outcome for the patient.
References
- 1.Pincus D, Jenkinson R, Paterson M, Leroux T, Ravi B. Association between surgical approach and major surgical complications in patients undergoing total hip arthroplasty. JAMA 2020;323:1070-6. [Google Scholar | PubMed]
- 2.Parvizi J, Tan TL, Goswami K, Higuera C, Valle DC, Chen AF, et al. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J Arthroplasty 2018;33:1309-14.e2. [Google Scholar | PubMed]
- 3.Izakovicova P, Borens O, Trampuz A. Periprosthetic joint infection: Current concepts and outlook. EFORT Open Rev 2019;4:482-94. [Google Scholar | PubMed]
- 4.Conte SM, Vale PR. Peripheral arterial disease. Heart Lung Circ 2018;27:427-32. [Google Scholar | PubMed]
- 5.Aronow WS. Peripheral arterial disease of the lower extremities. Arch Med Sci 2012;8:375-88. [Google Scholar | PubMed]
- 6.Schwartz AJ, Trask DJ, Bews KA, Hanson KT, Etzioni DA, Habermann EB. Hip disarticulation for periprosthetic joint infection: Frequency, outcome, and risk factors. J Arthroplasty 2020;35:3269-73.e3. [Google Scholar | PubMed]
- 7.Simman R, Klomparens K, Abbas FT, Lamaj S, Rehman N. Hip disarticulation in wound care: A case series. Eplasty 2022;22:e28. [Google Scholar | PubMed]
- 8.Zalavras CG, Rigopoulos N, Ahlmann E, Patzakis MJ. Hip disarticulation for severe lower extremity infections. Clin Orthop Relat Res 2009;467:1721-6. [Google Scholar | PubMed]
- 9.Moura DL, Garruço A. Hip disarticulation-case series analysis and literature review. Rev Bras Ortop 2017;52:154-8. [Google Scholar | PubMed]
- 10.Dua A, Lee CJ. Epidemiology of peripheral arterial disease and critical limb ischemia. Tech Vasc Interv Radiol 2016;19:91-5. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 April 10, 2024 Short-term Success in Treatment of an Acute Hematogenous Periprosthetic Hip Joint Infection with Debridement, Antibiotics, and Implant Retention
April 10, 2024 Short-term Success in Treatment of an Acute Hematogenous Periprosthetic Hip Joint Infection with Debridement, Antibiotics, and Implant Retention August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips