
Recalcitrant lateral epicondylitis, especially in the background of repeated steroid injections should alert practitioners to the possibility of full thickness tear of common extensor origin.
Dr. Udit Kumar Biswal, Department of Orthopaedics, Sparsh Hospital, Bengaluru, Karnataka, India. E-mail: uditkumarbiswal@gmail.com
Abstract
Introduction: Complete avulsion of the common extensor origin of the elbow is a very rare injury which significantly weakens upper limb function. The restoration of the extensor origin is indispensable to the function of the elbow. There are very few reports of such injuries and their reconstruction.
Case Report: We present a case report of a 57-year-old male who presented with pain and swelling of elbow with inability to lift objects for 3 weeks. We diagnosed a complete common extensor origin rupture due to prior degeneration after corticosteroid injection for tennis elbow. The patient underwent reconstruction of the extensor origin with suture anchor. His wound healed well and he was mobilized from 2 weeks onward. At 3 months, he had full recovery of range of movement.
Conclusion: It is crucial to diagnose these injuries, reconstruct them anatomically, and ensure good rehabilitation for optimum results.
Keywords: Common extensor origin, tennis elbow, steroid injection, suture anchor.
Sporting injuries of the elbow though quite uncommon in the past have been substantially increasing in incidence in the past decade due to the growing emphasis on an active lifestyle and cardiovascular benefits of active sports, even at an amateur level. The most common painful non-traumatic condition around the elbow is lateral epicondylitis or tennis elbow, affecting 1–3% of adults each year [1]. The most common soft-tissue injury around the elbow appears to be the avulsion or rupture of the common extensor origin from the lateral epicondyle of the humerus [2]. There has been a great deal of controversy regarding the anatomical location of the extensor carpi radialis brevis (ECRB) and extensor digitorum communis (EDC) tendons in the so called “common extensor origin.” The general consensus is that the two origins are deeply adherent albeit separable. The ECRB tendon constitutes the deepest 25–35% of the common origin while the EDC constitutes bulk of the superficial origin [3]. This, along with the fact that the ECRB is attached in contrasting pattern to the lateral epicondyle to allow it to remain attached at all times to the bone while allowing for movement without any restriction. This is also the reason why ECRB is most commonly implicated in the pathogenesis of tennis elbow pain [4,5,6]. The brachioradialis remains closely associated with the ECRL and ECRB, but it originates further proximally from the lateral supracondylar ridge and the lateral intermuscular septum. There are very few case reports of rupture of the common extensor origin and even fewer to no reports of rupture of the common extensor origin, lateral ulnar collateral ligament (LUCL), lateral collateral ligament, as well as the brachioradialis origin together in the same elbow. We present such a rare case with clinical photographs and a complete follow-up and evaluation of the results of reconstruction.
A 57-year-old gentleman who is a casual tennis player, presented to our outpatient clinic with complaints of pain and swelling over outer aspect of the right elbow for the past 3 weeks. As per his recollection, 3 weeks back while playing tennis, he had felt a sharp pain in his right elbow, which has gradually progressed to the present condition. He gives history of past treatment for tennis elbow in the same limb with at least two instances of injection of corticosteroid into the lateral epicondyle region. The pain was brought about by activity and almost completely relieved by rest. When he found it difficult to lift objects with the right hand, he consulted us. On examination, we found a soft ill-defined swelling over the posterolateral aspect of the right elbow which was diffusely tender with maximum tenderness over the lateral epicondylar tip. Stress testing revealed a Grade II varus laxity. The range of movements at the elbow was full range but terminally painful and painful against resistance. Cozen’s test was negative. A plain X-ray was normal and we did an magnetic resonance imaging (MRI) with limited computed tomography cuts for the elbow. The MRI revealed subtotal disruption of the common extensor origin from the lateral epicondyle (Fig. 1). The residual fibers were elevated by fluid loculation extending from the joint, likely indicating disruption of joint capsule into lateral subcutaneous aspect of the elbow measuring about 2.5 × 2.2 × 3.0 cm. Mild elbow joint effusion was reported which communicated with the lateral subcutaneous collection.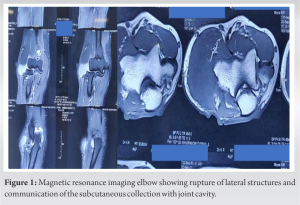 The bones revealed normal marrow intensities. The biceps and triceps insertion, the lateral and medial collateral ligaments, the LUCL, and the annular ligament were reported as normal. There were small chips of bony avulsion of the lateral epicondyle. He was prepared for an open repair of the torn lateral structures under general anesthesia. A standard Kochers lateral approach was taken to the elbow. There was a gross soft-tissue defect below the lateral epicondyle (Fig. 2).
The bones revealed normal marrow intensities. The biceps and triceps insertion, the lateral and medial collateral ligaments, the LUCL, and the annular ligament were reported as normal. There were small chips of bony avulsion of the lateral epicondyle. He was prepared for an open repair of the torn lateral structures under general anesthesia. A standard Kochers lateral approach was taken to the elbow. There was a gross soft-tissue defect below the lateral epicondyle (Fig. 2). 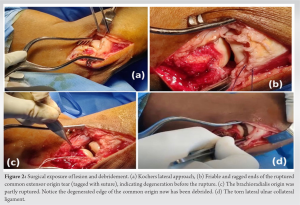 The common extensor origin was ruptured in its entirety and retracted distally for about 2 cm. The edges of the rupture were ragged and friable, suggesting prior degeneration, probably due to repeated episodes of corticosteroid injection into the elbow. There was partial detachment of the origin of the brachioradialis from the lateral epicondylar ridge which was tagged with a fiberwire stitch. Annular ligament appeared partly intact. The LUCL appeared torn from the humerus. There was a small circumscribed bony defect in the most lateral part of the lateral epicondyle. The ragged edge of the tendinous rupture was debrided and devitalized bits were trimmed. A fiberwire stitch was taken in the ruptured tendon. Using image intensifier, the center of the humeral condyle on true lateral view was marked as the point of insertion of suture anchor (Fig. 3).
The common extensor origin was ruptured in its entirety and retracted distally for about 2 cm. The edges of the rupture were ragged and friable, suggesting prior degeneration, probably due to repeated episodes of corticosteroid injection into the elbow. There was partial detachment of the origin of the brachioradialis from the lateral epicondylar ridge which was tagged with a fiberwire stitch. Annular ligament appeared partly intact. The LUCL appeared torn from the humerus. There was a small circumscribed bony defect in the most lateral part of the lateral epicondyle. The ragged edge of the tendinous rupture was debrided and devitalized bits were trimmed. A fiberwire stitch was taken in the ruptured tendon. Using image intensifier, the center of the humeral condyle on true lateral view was marked as the point of insertion of suture anchor (Fig. 3).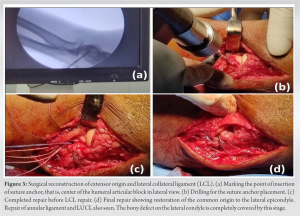 A 5.4 mm Arthrex Corkscrew FT II suture anchor (Arthrex Inc, Naples, FL, USA) was placed in the predetermined point in the lateral condyle. The fiberwire stitch through the ruptured extensor tendon was tied in a knot to the fiberwire of the anchor. The anchor was tightened, thus pulling the retracted edge of the tendon proximally to a more anatomic location. The sutures through the brachioradialis were also tightened to the rest of the repair. After this step of the procedure, the majority of the repair was complete. The LCL was then repaired with the other loop of fiberwire. All the redundant wire loops were cut. The elbow range of movement and stability of the repair was checked by gentle motion. Then, the wound was washed and closed in layers. No suction drain was used. A posterior plaster splint was applied in 90° elbow flexion. Post-operative day wound check was satisfactory. He was discharged on post-operative day 2. The skin stitches were removed on post-operative day 15. The wound had healed satisfactorily. A crepe bandage and a thermoplastic posterior elbow splint were applied in 90° of elbow flexion and gradual active elbow mobilization was initiated. At 6 weeks from the date of surgery, he had regained nearly normal range of movement with the exception of terminal 10° of extension. At 3 months, he had regained full pain free range of movement and was comfortable in all household activities (Fig. 4).
A 5.4 mm Arthrex Corkscrew FT II suture anchor (Arthrex Inc, Naples, FL, USA) was placed in the predetermined point in the lateral condyle. The fiberwire stitch through the ruptured extensor tendon was tied in a knot to the fiberwire of the anchor. The anchor was tightened, thus pulling the retracted edge of the tendon proximally to a more anatomic location. The sutures through the brachioradialis were also tightened to the rest of the repair. After this step of the procedure, the majority of the repair was complete. The LCL was then repaired with the other loop of fiberwire. All the redundant wire loops were cut. The elbow range of movement and stability of the repair was checked by gentle motion. Then, the wound was washed and closed in layers. No suction drain was used. A posterior plaster splint was applied in 90° elbow flexion. Post-operative day wound check was satisfactory. He was discharged on post-operative day 2. The skin stitches were removed on post-operative day 15. The wound had healed satisfactorily. A crepe bandage and a thermoplastic posterior elbow splint were applied in 90° of elbow flexion and gradual active elbow mobilization was initiated. At 6 weeks from the date of surgery, he had regained nearly normal range of movement with the exception of terminal 10° of extension. At 3 months, he had regained full pain free range of movement and was comfortable in all household activities (Fig. 4).
This injury was a highly debilitating injury of the elbow which hampered the daily life as well as physical activity of the patient. The reconstruction done by us healed without any complications and the patient regained most of his range of movements without pain, by the time, this paper was being written. Very few published reports of such injuries are available across all databases. Kachrimanis and Papadopoulou [7], in their paper, described the ultrasonographic features of an acute partial rupture of the common extensor origin tendon. Their patient also had taken three steroid injections into the lesion before it ruptured. However, they did not comment on the method of treatment. Smith et al., [8] reported a case of rupture after corticosteroid injection for lateral epicondylitis of the elbow. They found rupture of the central 75% of the tendon intraoperative. They debrided and performed a side to side repair of the tendons. Histopathological evaluation showed fibrillary degeneration of the collagen bundles in the affected tendon. The aforementioned reports along with our case report is a testament to the fact that indiscriminate injections of corticosteroids into the lateral epicondylar area, like steroid injections into tendons elsewhere, carry with it a low but dangerous chance of massive rupture of the entire lateral ligamentous complex of elbow, thus rendering the elbow nearly useless for any physical activity. Such injections should be judiciously used where actually indicated, with informed consent of the patient about its possible complications. Steroid injections lead to fibrillary degeneration in the tendinous structures [9,10]; hence, the avulsed edges of the tendon are often devitalized and friable. Adequate debridement of such tissues before repair is of paramount importance to avoid cut through of sutures, leading to repair failure and need for re-surgery. Prolonged immobilization of such massive repairs with a view to protect the repair is not advisable as they increase the already existing elbow stiffness. Early judicious mobilization ensures satisfactory function of the elbow to gradually resume high demand physical activity.
Suture anchors are a reliable way of repairing such massive tears along with nearby structures that need repair. Such injuries though rare are quite debilitating to the functioning of the patients elbow. A sound repair and judicious physiotherapy are of utmost importance in regaining function.
We hope this illustrated case report of massive common extensor origin rupture and its treatment will help surgeons encountering this rare condition in their practice and most of all warn practitioners about the hazards of indiscriminate steroid injections into any tendinous area in the body.
References
- 1.Allander E. Prevalence, incidence, and remission rates of some common rheumatic diseases or syndromes. Scand J Rheumatol 1974;3:145-53. [Google Scholar | PubMed]
- 2.Martinoli C, Bianchi S, Giovagnorio F, Pugliese F. Ultrasound of the elbow. Skeletal Radiol 2001;30:605-14. [Google Scholar | PubMed]
- 3.Dones VC IIIrd, Milanese S, Worth D, Grimmer-Somers K. The anatomy of the forearm extensor muscles and the fascia in the lateral aspect of the elbow joint complex. Anatom Physiol 2013;3:1000117. [Google Scholar | PubMed]
- 4.Bunata RE, Brown DS, Capelo R. Anatomic factors related to the cause of tennis elbow. J Bone Joint Surg Am 2007;89:1955-63. [Google Scholar | PubMed]
- 5.Albrecht S, Cordis R, Kleihues H, Noack W. Pathoanatomic findings in radiohumeral epicondylopathy. A combined anatomic and electromyographic study. Arch Orthop Trauma Surg 1997;116:157-63. [Google Scholar | PubMed]
- 6.Faro F, Wolf JM. Lateral epicondylitis: Review and current concepts. J Hand Surg Am 2007;32:1271-9. [Google Scholar | PubMed]
- 7.Kachrimanis G, Papadopoulou O. Acute partial rupture of the common extensor tendon. J Ultrasound 2010;13:74-75. [Google Scholar | PubMed]
- 8.Smith A, Kosygan K, Williams H, Newman R. Common extensor tendon rupture following corticosteroid injection for lateral tendinosis of the elbow. Br J Sports Med 1999;33:423-4. [Google Scholar | PubMed]
- 9.Fredberg U. Local corticosteroid injection in sport: review of literature and guidelines for treatment. Scand J Med Sci Sport 1997;7:131-9. [Google Scholar | PubMed]
- 10.Maman E, Yehuda C, Pritsch T, Morag G, Brosh T, Sharfman Z, et al. Detrimental effect of repeated and single sub-acromial corticosteroid injections on the intact and injured rotator cuff: A biomechanical and imaging study in rats. Am J Sports Med 2016;44:177-82. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 A Prospective Randomized Controlled Study Comparing the Efficacy of Platelet Rich Plasma Injection versus Steroid Injection in Lateral Epicondylitis
July 1, 2026 A Prospective Randomized Controlled Study Comparing the Efficacy of Platelet Rich Plasma Injection versus Steroid Injection in Lateral Epicondylitis January 1, 2026 Correlation of Serum Vitamin D Levels and Incidence of Lateral Epicondylitis of the Elbow: An Observational Study in Eastern India
January 1, 2026 Correlation of Serum Vitamin D Levels and Incidence of Lateral Epicondylitis of the Elbow: An Observational Study in Eastern India December 1, 2025 Platelet-Rich Plasma Injections are Associated with Higher Resource Utilization and Surgical Escalation Compared with Corticosteroids in Lateral Elbow Tendinopathy
December 1, 2025 Platelet-Rich Plasma Injections are Associated with Higher Resource Utilization and Surgical Escalation Compared with Corticosteroids in Lateral Elbow Tendinopathy October 1, 2025 Comparison of Efficacy of Autologous Blood Injection versus Steroid Injection in Treatment of Lateral Epicondylitis: A Comparative Study
October 1, 2025 Comparison of Efficacy of Autologous Blood Injection versus Steroid Injection in Treatment of Lateral Epicondylitis: A Comparative Study