Split Hand and Foot Malformation, Rare Condition, Clinical Presentation, and Management.
Dr. Kartik Dua, Department of Orthopaedic Surgery, Faculty of Medicine and Health Sciences, SGT University, Budhera, Gurugram, Haryana, India. E-mail: kartik_dua22@yahoo.co.in
Introduction: Authors report a rare case report about split hand and foot malformation (SHFM) also sometimes referred to as ectrodactyly.
Case Report: The patient with hand and foot malformations presented to casualty. A 60-year-old male was brought with alleged history of road traffic accident with tenderness and deformity in left thigh. On further physical examination, a malformation was present in bilateral feet and right hand. Plain radiographs were taken after emergency primary management which revealed a fracture of shaft of femur of the left side and absence of 2nd and 3rd phalanges in bilateral feet and lobster claw like malformation in the right hand. The patient was further investigated and operated with femur interlocking nail and later discharged under stable condition. Screening for other congenital defects was done.
Conclusion: Patients with SHFM should undergo screening for other congenital anomalies. Electrocardiogram, 2D ECHO, chest radiograph, and ultrasonography abdomen should be done. Genetic analysis ideally should be done to identify mutations involved. Surgical intervention is only required when patient demands improved function of limb.
Keywords: Split hand and foot malformation, split hand/foot malformation with long bone deficiency, DLX5, DLX6, DSS, Xq26, DACTYLIN, P63, 2q31, WNT10B.
Split hand and foot malformation (SHFM) is a congenital abnormality of the limbs. It is predominantly seen to be affecting the central rays of hand and foot. Bidactyly and monodactyly in hand and foot can also be seen in severe cases. SHFM occurs sporadically but can also be inherited following most commonly an autosomal dominant pattern, but X-linked and autosomal recessive cases have also been reported [1]. The incidence of SHFM – is reported to be as low as 1 in 90,000 [2].
The patient was 60-year-old male with alleged history of road traffic accident under unknown circumstances, was referred from primary health center for management of long bone injury that the patient had sustained. The patient was an unknown accompanied by staff of organization who look after the destitutes. Furthermore, the patient had a low IQ and it was not possible to elicit proper history. On primary survey, the patient was found to have deformity, crepitus, and tenderness at left thigh. There was no external wound and patient was found to be calm, conscious, and hemodynamically stable. Primary emergency management started and IV fluids administered with injectable analgesics. On further physical examination, there was complete absence of 2nd and 3rd digits of both feet along with lobster claw like malformation in the right hand (Fig. 1 and 2).  The patient sent for plain radiographs after stabilization of fractured limb by a splint. Radiographs revealed fracture of shaft of femur left side with absence of 2nd and 3rd proximal and distal phalanges of both feet (Figs. 3 and 4). All routine investigations were sent and skeletal traction applied to fractured limb through upper tibial pin. Ultrasonography (USG) abdomen, electrocardiogram (ECG), 2D ECHO, and chest radiograph showed no abnormality. The fracture shaft of femur was managed with closed reduction and internal fixation with interlocking nail. Since patient was not demanding improved function of deformed limbs, deformity correction was not done.
The patient sent for plain radiographs after stabilization of fractured limb by a splint. Radiographs revealed fracture of shaft of femur left side with absence of 2nd and 3rd proximal and distal phalanges of both feet (Figs. 3 and 4). All routine investigations were sent and skeletal traction applied to fractured limb through upper tibial pin. Ultrasonography (USG) abdomen, electrocardiogram (ECG), 2D ECHO, and chest radiograph showed no abnormality. The fracture shaft of femur was managed with closed reduction and internal fixation with interlocking nail. Since patient was not demanding improved function of deformed limbs, deformity correction was not done.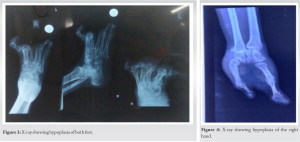
SHFM is a group of hereditary skeletal disorders with possible variable phenotypes. It is a clinically heterogeneous condition and has a wide spectrum ranging from shortening of the single digit to monodactyly [3]. Furthermore, in cases of SHFLD, a variant there is absence of long bones [4]. SHFM can be seen affecting single limb or multiple limbs. It may occur in syndromic forms associated with extra limb formation. Various genetic researches have been conducted and literature reveals mapping of seven different genetic loci associated with the isolated form of SHFM, the chromosomal defects being 7q rearrangements involving genes DLX5, DLX6, DSS1 for SHFM1 [5], Xq26 for SHFM2 [6], 10q24 duplication involving DACTYLIN for SHFM3 [7], mutations in P63 gene at 3q for SHFM4 [8], deletion at 2q31 for SHFM5 [9], WNT10B mutation involving chromosome 12q13 [10] for SHFM6, and duplication 7p13.3 for SHFLD (a variant with absent long bone) [11]. Surgical intervention may be required in SHFM to improve functions or appearance of limb. Prosthesis for SHFM is also available. Possibility of recurrence in future siblings should be explained to the parents. Antenatal diagnosis of SHFM can be done with ultrasonography [12]. Due to rarity of this malformation, the literature on surgical management of SHFM is limited and one such literature published which reports about an individual who was presented with bilateral SHFM and bidactylous hands. The thumbs were hypoplastic, whereas ulnar digit was broad maybe due to fusion of the two rays also known as super digit. During the surgery, they identified all tendons and muscles of forearm. They also managed to identify flexor and extensor tendons of the missing fingers. These tendons were identified in forearm and traced to the hand but tendons were ended in cleft where they formed few loops in middle of cleft. It was reported that extra tendons maybe the reason for camptodactyly (digital flexion deformity of proximal interphalangeal joint) and rotation of fingers while in flexion. It was also stated that cautious division of cleft and lateral side of finger with excision of extra tendons improved functional and cosmetic outcome of patients [13].
Patients with SHFMs should undergo screening for other congenital anomalies. ECG, 2D ECHO, chest radiograph, and USG abdomen should be done. Genetic analysis ideally should be done to identify mutations involved. Surgical intervention is only required when patient demands improved function of limb.
- Diagnosis of associated congenital defects should be done and addressed accordingly.
- Patients to be counseled for malformations if he/she is planning for pregnancy.
- Surgical intervention is required if patient demands improved function of the limb.
References
- 1.Guero S, Holder-Espinasse M. Insights into the pathogenesis and treatment of split/hand foot malformation (cleft hand/foot). J Hand Surg Eur 2019;44:80-7. [Google Scholar]
- 2.Barsky AJ. Cleft hand: Classification, incidence, and treatment. Review of the literature and report of nineteen cases. J Bone Joint Surg Am 1964;46:1707‐20. [Google Scholar]
- 3.Sowińska-Seidler A, Socha M, Jamsheer A. Split-hand/foot malformation-molecular cause and implications in genetic counseling. J Appl Genet 2014;55:105-15. [Google Scholar]
- 4.Klopocki E, Lohan S, Doelken SC, Stricker S, Ockeloen CW, de Aguiar RS, et al. Duplications of BHLHA9 are associated with ectrodactyly and tibia hemimelia inherited in non-Mendelian fashion. J Med Genet 2012;49:119-25. [Google Scholar]
- 5.Crackower MA, Scherer SW, Rommens JM, Hui CC, Poorkaj P, Soder S, et al. Characterization of the split hand/split foot malformation locus SHFM1 at 7q21.3-q22.1 and analysis of a candidate gene for its expression during limb development. Hum Mol Genet 1996;5:571-9. [Google Scholar]
- 6.Haque MF, Uhlhaas S, Knapp M, Schüler H, Friedl W, Ahmad M, et al. Mapping of the gene for X-chromosomal split-hand/split-foot anomaly to Xq26-q26.1. Hum Genet 1993;91:17-9. [Google Scholar]
- 7.Ianakiev P, Kilpatrick MW, Dealy C, Kosher R, Korenberg JR, Chen XN, et al. A novel human gene encoding an F-box/WD40 containing protein maps in the SHFM3 critical region on 10q24. Biochem Biophys Res Commun 1999;261:64-70. [Google Scholar]
- 8.Ianakiev P, Kilpatrick MW, Toudjarska I, Basel D, Beighton P, Tsipouras P. Split-hand/split-foot malformation is caused by mutations in the p63 gene on 3q27. Am J Hum Genet 2000;67:59-66. [Google Scholar]
- 9.Goodman FR, Majewski F, Collins AL, Scambler PJ. A 117-kb microdeletion removing HOXD9-HOXD13 and EVX2 causes synpolydactyly. Am J Hum Genet 2002;70:547-55. [Google Scholar]
- 10.Khan S, Basit S, Zimri FK, Ali N, Ali G, Ansar M, et al. A novel homozygous missense mutation in WNT10B in familial split-hand/foot malformation. Clin Genet 2012;82:48-55. [Google Scholar]
- 11.Lezirovitz K, Maestrelli SR, Cotrim NH, Otto PA, Pearson PL, Mingroni-Netto RC. A novel locus for split-hand/foot malformation associated with tibial hemimelia (SHFLD syndrome) maps to chromosome region 17p13.1-17p13.3. Hum Genet 2008;123:625-31. [Google Scholar]
- 12.Jindal G, Parmar VR, Gupta VK. Ectrodactyly/split hand feet malformation. Indian J Hum Genet 2009;15:140-2. [Google Scholar]
- 13.Durand S, Delmas V, Fox M, Hivelin M, Oberlin C, Guero S. Anatomic variations in a cleft hand of an elder cadaveric specimen. Surg Radiol Anat 2009;31:145-8. [Google Scholar]