
To avoid arterial injury during THA, surgeons should preoperatively assess the location of the intrapelvic vessels around the acetabulum by three-dimensional CT angiography in cases with complicated hip anatomy.
Dr. Masahiro Suzuki, Department of Orthopedic Surgery, Eniwa Hospital, 2-1-1 Koganechuo, Eniwa, Hokkaido 061-1449, Japan. E-mail: 0321suzuki@gmail.com
Abstract
Introduction: Total hip arthroplasty (THA) is widely accepted as a safe and effective procedure to relieve hip pain and restore function, but complications can lead to a poor outcome. Although major vascular injuries during THA are rare, when they do occur, massive bleeding may threaten life.
Case Report: We describe a case of a 72-year-old woman who underwent THA after rotational acetabular osteotomy (RAO). When the soft tissue in the acetabular fossa was dissected with electrocautery, massive pulsatile bleeding suddenly occurred. A blood transfusion and metal stent graft repair saved her life. We assume that the cause of the arterial injury was a bone defect of the acetabulum and relocation of the external iliac artery after RAO.
Conclusion: To avoid arterial injury during THA, pre-operative three-dimensional computed tomographic angiography to locate the intrapelvic vessels around the acetabulum is recommended in cases with complex hip anatomy.
Keywords: Major vascular injury, total hip arthroplasty, periacetabular osteotomy.
Total hip arthroplasty (THA) is widely accepted as a safe and effective treatment for patients with advanced osteoarthritic hips to relieve hip pain and restore function. However, serious complications that sometimes threaten life do occur. Of these, major vascular injury is the most devastating. Recent large studies have reported that the incidence of vascular injury during primary THA is 0.03–0.12% [1,2,3,4]. Particular attention should be paid to cases with developmental hip dysplasia and/or previous pelvic surgery. Here, we describe a case of external iliac artery injury due to a bone defect in the acetabulum during THA after rotational acetabular osteotomy (RAO) [5]. To the best of our knowledge, there have been no prior reports of external iliac artery injury caused by this mechanism.
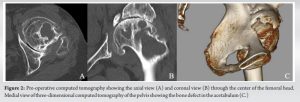
A 72-year-old woman first presented to us with severe pain in the left hip. She had received a right shelf procedure 33 years earlier and a left RAO 25 years earlier for developmental dysplasia of the hip at another hospital. For the past 7 years, the patient had complained of increasing pain with activity limitation, which had recently severely affected her daily life. An anteroposterior radiograph revealed severe osteoarthritic changes in the left hip joint with irregular narrowing of the joint space (Fig. 1), and we diagnosed advanced osteoarthritis of the hip.  Computed tomography (CT) revealed a large bone defect from the medial side to the anterior aspect of the acetabulum (Fig. 2).
Computed tomography (CT) revealed a large bone defect from the medial side to the anterior aspect of the acetabulum (Fig. 2).
 Therefore, we planned a THA with a bulk bone graft. After lumbar anesthesia, the patient was placed in the right lateral position. The surgery was performed using a posterolateral approach. After incision of the pisiform tendon, external rotators, and posterior capsule, the femoral head was dislocated and the neck was osteotomized. When the soft tissue in the acetabular fossa was dissected with electrocautery, massive pulsatile bleeding was suddenly encountered. Attempts to stop the bleeding such as tight packing with gauze, using microfibrillar collagen in sheet form, and intravenous tranexamic acid were unsuccessful. The bleeding gradually diminished, but the patient went into shock. The wound was closed without implanting the components and the patient was sent to the emergency hospital 4 h after the incident. Angiography was performed with the femoral artery by an expert interventional radiologist. The definitive diagnosis was achieved by selective digital subtraction angiography of the left external iliac artery, and active contrast extravasation was depicted near the inner wall of the acetabulum (Fig. 3). The lacerated portion of the artery was small and it was repaired with metal stent grafting (Fig. 4). Due to the massive blood loss, 16 units of red blood cell transfusion, 18 units of fresh frozen plasma transfusion, and 20 units of platelet concentrate were required. Three-dimensional computed tomographic angiography after stent grafting showed that the left external iliac artery was extremely close to the acetabulum (Fig. 5). The patient recovered well after the stent graft and was readmitted to our hospital 4 days later. THA was performed 2 weeks after the stent graft, and the post-operative course was uneventful.
Therefore, we planned a THA with a bulk bone graft. After lumbar anesthesia, the patient was placed in the right lateral position. The surgery was performed using a posterolateral approach. After incision of the pisiform tendon, external rotators, and posterior capsule, the femoral head was dislocated and the neck was osteotomized. When the soft tissue in the acetabular fossa was dissected with electrocautery, massive pulsatile bleeding was suddenly encountered. Attempts to stop the bleeding such as tight packing with gauze, using microfibrillar collagen in sheet form, and intravenous tranexamic acid were unsuccessful. The bleeding gradually diminished, but the patient went into shock. The wound was closed without implanting the components and the patient was sent to the emergency hospital 4 h after the incident. Angiography was performed with the femoral artery by an expert interventional radiologist. The definitive diagnosis was achieved by selective digital subtraction angiography of the left external iliac artery, and active contrast extravasation was depicted near the inner wall of the acetabulum (Fig. 3). The lacerated portion of the artery was small and it was repaired with metal stent grafting (Fig. 4). Due to the massive blood loss, 16 units of red blood cell transfusion, 18 units of fresh frozen plasma transfusion, and 20 units of platelet concentrate were required. Three-dimensional computed tomographic angiography after stent grafting showed that the left external iliac artery was extremely close to the acetabulum (Fig. 5). The patient recovered well after the stent graft and was readmitted to our hospital 4 days later. THA was performed 2 weeks after the stent graft, and the post-operative course was uneventful.
Although major vascular injuries during THA are rare, they may pose a serious threat to the involved limb and the patient’s life. Causes of direct intraoperative major vessel injury include improper placement of retractors, inadvertent screw insertion for fixation of acetabular components or bone grafts, and excessive acetabular reaming [2,6,7]. Previous surgery to the hip is also a risk factor for direct vascular injury during THA [2,8]. In this case, direct injury to the external iliac artery occurred during dissection of the soft tissue in the acetabular fossa in THA after RAO. Several types of periacetabular osteotomy (PAO) have been developed to treat symptomatic acetabular dysplasia, including RAO, transposition osteotomy of the acetabulum, Bernese PAO, curved PAO, and University of Colorado PAO. There are several reports that THA after PAO demonstrates the following characteristics: large osteophytes, acetabular sclerosis, and acetabular wall defects [9,10,11,12]. The cause of bone defect in this case was considered to be due to the chisel cutting into the cartilage around the acetabular fossa during the initial RAO and further abduction and retroversion of the osteotomized acetabulum. Therefore, it is important that surgeons understand the precise hip anatomy of each case. In our case, the bony morphology of the acetabulum was abnormal, with a medial bony defect. A previous study based on three-dimensional CT angiography of the normal hip joint reported that the mean shortest distance between the external iliac artery and the osseous surface of the pelvis was at least 10 mm at any level of the acetabulum [13]. In contrast, in the present case, the distance from the bone defect to the external iliac artery was 3.4 mm. Considering that the external iliac artery runs along the iliacus muscle, the course of the external iliac artery may change with acetabular rotation in RAO.
To avoid arterial injury during THA, careful attention should be paid to patients with previous RAO, which may have resulted in distortion of the acetabular anatomy. It is advisable to preoperatively assess the location of the intrapelvic vessels around the acetabulum by three-dimensional CT angiography in cases with complicated hip anatomy.
The acetabulum after PAO, including RAO, has a significantly altered anatomic morphology compared to pre-operative. To avoid arterial injury during THA, surgeons should preoperatively assess the location of the intrapelvic vessels around the acetabulum by three-dimensional CT angiography in cases with complicated hip anatomy.
References
- 1.Abularrage CJ, Weiswasser JM, Dezee KJ, Slidell MB, Henderson WG, Sidawy AN. Predictors of lower extremity arterial injury after total knee or total hip arthroplasty. J Vasc Surg 2008;47:803-7; discussion 807-8. [Google Scholar | PubMed]
- 2.Parvizi J, Pulido L, Slenker N, Macgibeny M, Purtill JJ, Rothman RH. Vascular injuries after total joint arthroplasty. J Arthroplasty 2008;23:1115-21. [Google Scholar | PubMed]
- 3.Troutman DA, Dougherty MJ, Spivack AI, Calligaro KD. Updated strategies to treat acute arterial complications associated with total knee and hip arthroplasty. J Vasc Surg 2013;58:1037-42. [Google Scholar | PubMed]
- 4.Avisar E, Elvey MH, Bar-Ziv Y, Tamir E, Agar G. Severe vascular complications and intervention following elective total hip and knee replacement: A 16-year retrospective analysis. J Orthop 2015;12:151-5. [Google Scholar | PubMed]
- 5.Ninomiya S, Tagawa H. Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am 1984;66:430-6. [Google Scholar | PubMed]
- 6.Mallory TH. Rupture of the common iliac vein from reaming the acetabulum during total hip replacement. A case report. J Bone Joint Surg Am 1972;54:276-7. [Google Scholar | PubMed]
- 7.Wasielewski RC, Galat DD, Sheridan KC, Rubash HE. Acetabular anatomy and transacetabular screw fixation at the high hip center. Clin Orthop Relat Res 2005;438:171-6. [Google Scholar | PubMed]
- 8.Shoenfeld NA, Stuchin SA, Pearl R, Haveson S. The management of vascular injuries associated with total hip arthroplasty. J Vasc Surg 1990;11:549-55. [Google Scholar | PubMed]
- 9.Ito H, Takatori Y, Moro T, Oshima H, Oka H, Tanaka S. Total hip arthroplasty after rotational acetabular osteotomy. J Arthroplasty 2015;30:403-6. [Google Scholar | PubMed]
- 10.Fukui K, Kaneuji A, Sugimori T, Ichiseki T, Matsumoto T. Does rotational acetabular osteotomy affect subsequent total hip arthroplasty? Arch Orthop Trauma Surg 2015;135:407-15. [Google Scholar | PubMed]
- 11.Tamaki T, Oinuma K, Miura Y, Shiratsuchi H. Total hip arthroplasty after previous acetabular osteotomy: Comparison of three types of acetabular osteotomy. J Arthroplasty 2016;31:172-5. [Google Scholar | PubMed]
- 12.Osawa Y, Hasegawa Y, Okura T, Morita D, Ishiguro N. Total hip arthroplasty after periacetabular and intertrochanteric valgus osteotomy. J Arthroplasty 2017;32:857-61 [Google Scholar | PubMed]
- 13.Kawasaki Y, Egawa H, Hamada D, Takao S, Nakano S, Yasui N. Location of intrapelvic vessels around the acetabulum assessed by three-dimensional computed tomographic angiography: Prevention of vascular-related complications in total hip arthroplasty. J Orthop Sci 2012;17:397-406. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report
August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report