
Atypical presentation of enchondroma.
Dr. Lakshmana Reddy Satti, Department of Orthopaedic Surgery, GGH, Rangaraya Medical College, Kakinada - 533 001, Andhra Pradesh, India. E-mail: slakshmanareddy@gmail.com
Introduction: Enchondroma is a solitary, benign, and intramedullary cartilaginous tumor occurring most commonly in small bones of hands and feet contributing to 3–10% of all bone tumors. They originate from the growth plate cartilage which later on proliferates to form enchondroma. Lesions are central or eccentric and metaphyseal involvement is most common for long bones. We report a case of atypical occurrence of enchondroma in the head of femur in a young male.
Case Report: A 20-year-old male patient presented with a history of pain in the left groin for 5 months. Radiological examination showed a lytic lesion in the head of femur. The patient was managed by safe surgical dislocation of the hip, curettage with autogenous iliac crest bone graft with countersunk screw fixation. Histopathology confirmed the lesion to be enchondroma. At the latest follow-up after 6 months, the patient was symptom-free and there was no evidence of any recurrence.
Conclusion: Lytic lesions in the neck femur can have a good prognosis provided timely diagnosis and interventions are done. The present case of enchondroma in the head of femur represents a very rare differential diagnosis for the same and this must be kept in mind. So far, no such case has been reported in the literature. Magnetic resonance imaging and histopathology are of the essence to confirm this entity.
Keywords: Enchondroma, atypical presentation, safe surgical dislocation of hip.
Enchondroma is a solitary, benign, and intramedullary cartilaginous tumor occurring most commonly in small bones of hands and feet. The distal femur and proximal humerus are other less common locations. Enchondroma consists of 3–10% of all bone tumors, while they constitute 12–24% of benign bone tumors. They originate from the growth plate cartilage which later on proliferates to form enchondroma. Radiographs reveal a localized, radiolucent lytic bone defect usually with punctuating calcifications often associated with “pop-corn” stippling, arcs, whorls, or rings. Lesions are central or eccentric and metaphyseal involvement is most common for long bones. Magnetic resonance imaging (MRI) and histopathological examination can be used to confirm the diagnosis. Asymptomatic cases can be managed conservatively with serial radiological follow-ups. Cases with symptoms are managed operatively. The recurrence rate is very low (<5%), which suggests malignancy. We report a case of atypical occurrence of enchondroma in the head of femur in a young male.
A 20-year-old male presented with a 5 months history of gradually progressive pain in the right hip region. The pain was dull aching in nature and aggravated on standing from a sitting posture. 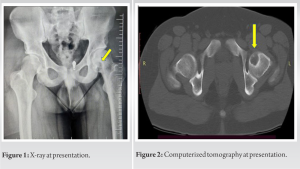 There was no radiation of pain, no history of trauma, fever, or night pains. On examination, the patient had no evidence of any systemic illness. Local examination revealed painful hip movements. There was no wound, sinus, swelling, or discharge found. There was no raised local temperature, lymphadenopathy, and neurovascular deficit. The blood workup showed normal hemogram, renal, and liver functions. Erythrocyte sedimentation rate, C-reactive protein, and parathyroid hormone levels were within normal limits. Anteroposterior radiograph of pelvis with both hips showed a well-defined geographic, predominantly lytic lesion in the head of the femur, anteroinferior in location, with a small amount of calcified matrix, with a narrow zone of transition (Fig. 1). It revealed no periosteal reaction, cortical destruction, and soft-tissue involvement. Computerized tomography (CT) impression was a 2×2.5 cm lytic lesion in the femoral head, with mild expansion. There was no obvious adjacent cortical breach to suggest pathological fracture. Findings were suggestive of benign bone lesion (Fig. 2). After careful pre-anesthetic evaluation, the patient was taken up for “safe surgical dislocation of hip (Fig. 3), curettage, and excision biopsy with autogenous iliac crest bone graft with Herbert screw fixation” (Fig. 4). A biopsy specimen was collected intraoperatively and sent later for histopathological examination, which revealed lobules of mature cartilage, separated by fibrous septa and bony spicules, features suggestive of enchondroma (Fig. 5).
There was no radiation of pain, no history of trauma, fever, or night pains. On examination, the patient had no evidence of any systemic illness. Local examination revealed painful hip movements. There was no wound, sinus, swelling, or discharge found. There was no raised local temperature, lymphadenopathy, and neurovascular deficit. The blood workup showed normal hemogram, renal, and liver functions. Erythrocyte sedimentation rate, C-reactive protein, and parathyroid hormone levels were within normal limits. Anteroposterior radiograph of pelvis with both hips showed a well-defined geographic, predominantly lytic lesion in the head of the femur, anteroinferior in location, with a small amount of calcified matrix, with a narrow zone of transition (Fig. 1). It revealed no periosteal reaction, cortical destruction, and soft-tissue involvement. Computerized tomography (CT) impression was a 2×2.5 cm lytic lesion in the femoral head, with mild expansion. There was no obvious adjacent cortical breach to suggest pathological fracture. Findings were suggestive of benign bone lesion (Fig. 2). After careful pre-anesthetic evaluation, the patient was taken up for “safe surgical dislocation of hip (Fig. 3), curettage, and excision biopsy with autogenous iliac crest bone graft with Herbert screw fixation” (Fig. 4). A biopsy specimen was collected intraoperatively and sent later for histopathological examination, which revealed lobules of mature cartilage, separated by fibrous septa and bony spicules, features suggestive of enchondroma (Fig. 5).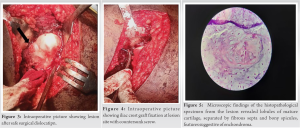 Postoperatively, the patient was advised bed rest with a derotation boot and restricted weight bearing. Static exercises were started on 2nd day. The patient was discharged on the 10th day and bed rest with a derotation boot was advised until 3 weeks. On follow-up, the patient was subjected to partial weight bearing after 6 weeks. At 6 months follow-up, the patient was able to bear complete weight, was symptom-free, and was able to perform activities of daily living (Fig. 6). No local recurrence was noted on repeat radiological examinations (Fig. 7). No further treatment was required.
Postoperatively, the patient was advised bed rest with a derotation boot and restricted weight bearing. Static exercises were started on 2nd day. The patient was discharged on the 10th day and bed rest with a derotation boot was advised until 3 weeks. On follow-up, the patient was subjected to partial weight bearing after 6 weeks. At 6 months follow-up, the patient was able to bear complete weight, was symptom-free, and was able to perform activities of daily living (Fig. 6). No local recurrence was noted on repeat radiological examinations (Fig. 7). No further treatment was required.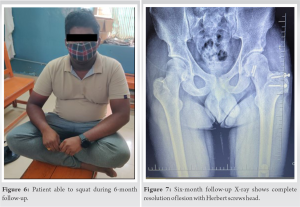
Enchondroma is the 2nd most common benign tumor of bone (after osteochondroma) having a hyaline cartilaginous origin. The tumor arises inside the medullary cavity of the bone, hence called enchondroma. This is the most common benign tumor of small bones of hands and feet; other locations such as long tubular bones (proximal humerus, distal femur, and proximal tibia) are rare. The occurrence of enchondroma in the head of the femur is one of the rarest locations for enchondroma to occur. The presence of pathology in the head of femur arouses suspicion of various other differential diagnoses. Hence, enchondroma should be kept in mind in such cases [1, 2]. Enchondroma is usually observed in 10–30 years of age group with equal gender distribution, being discovered incidentally in almost all cases. Mostly, they are asymptomatic. Pain may be the presenting symptom in some cases. Bone scan shows increased uptake when there are associated pathological fractures or cortical expansion in small bone [3]. An enchondroma may present as multiple enchondromas called Ollier’s disease [4]. It may also have associated with soft-tissue hemangiomas called Maffucci syndrome [5]. Enchondroma arises from the cartilaginous rests of the physeal plate. The lesion of enchondromas is closely related to physeal plate as 71% of enchondromas are within 1.5 cm of the epiphyseal plate of which 43% abutt the physeal plate and only 29% are more than 1.5 cm away from the physeal plate [6]. The patient, in the present study, was a 20-year-old male with a complaint of pain in the hip for 5 months. Careful clinical and radiological evaluation of the patient revealed a lytic cavity in the neck of the femur with no cortical breach and CT finding of a hyperintense lesion in the head of femur. A provisional diagnosis of enchondroma was made which was later confirmed on histopathology. The differential diagnosis of a lytic bone lesion in the proximal femur includes chondroblastoma, giant cell tumor, simple bone cyst, aneurysmal bone cyst, fibrous dysplasia, chondrosarcoma, chondromyxoid fibroma, and osteoblastoma [7]. Chondroblastoma is an epiphyseal lesion that presents in the young age group (<20 years) with pain and swelling, having a thin sclerotic rim and internal calcification on the radiograph, MRI shows surrounding edema with a typical chicken wire fence appearance on histology. A giant cell tumor is an epiphyseal tumor occurring commonly around the knee, having typical osteoclastic giant cells, and areas of hemorrhage on microscopic view and the lesions about the articular surface. Simple bone cyst occurs in children and contains clear serosanguinous fluid surrounded by a lining membrane. X-ray shows a lucent lesion with sclerotic margins in a skeletally immature patient. Aneurysmal bone cyst consists of blood-filled, lytic, and septate lesions. Fibrous dysplasia is usually detected in young individuals having ground-glass opacities and homogenously cystic or sclerotic lesions with MRI appearance of heterogeneous signal on T1 and T2 sequences. Chondrosarcomas are malignant cartilaginous tumors that occur in the 5th decade of life. On radiography, they show a lytic pattern with typical matrix mineralization, cortical breach, deep endosteal scalloping, and soft-tissue extension. Bone scan shows increased uptake. Differentiation of low-grade chondrosarcoma from enchondroma is very difficult as both are histologically and radiographically very similar. This needs a careful evaluation of such cases. Chondromyxoid fibromas are extremely rare benign neoplasms presenting with progressive pain and long-standing swelling. Grossly, they are solid glistening intraosseous masses. On a radiograph, they show a lobulated, eccentric radiolucent lesion with well-defined sclerotic margins. Osteoblastoma is rare occurring most commonly in the spinal column having a radiographic appearance on an expansile lytic lesion with a rim of reactive sclerosis and internal calcification. MRI shows an isointense or hypointense signal on the T2 sequence. As far as the treatment is concerned, asymptomatic cases are managed conservatively with serial radiographic follow-ups. Symptomatic cases require surgical intervention. Extended curettage with hydrogen peroxide lavage of the lytic cavity is done and filled with bone graft. Recent advancement permits the treatment of femoral head enchondroma using arthroscopic curettage and fixation which is a less invasive procedure with better clinical outcome [8]. In the present study, the treatment done was a safe surgical dislocation of the hip, curettage, and excision biopsy with autogenous iliac crest bone graft with Herbert screw fixation. On extensive review of the literature, very few reports of such cases were found. In 1925, LeConte et al. reported a case of enchondroma of the neck of femur with repeated recurrences which lead to mortality [9]. Another case of solitary enchondroma in the neck of femur was reported in 1986 by Mori et al., in a 7-year-old girl [10]. Hence, we emphasize the fact that although enchondroma in the neck of femur is extremely rare, timely diagnosis and treatment can lead to a good prognosis.
Lytic lesions in the neck femur can have a good prognosis provided timely diagnosis and interventions are done. The present case of enchondroma in the head of femur represents a very rare differential diagnosis for the same and this must be kept in mind. So far, no such case has been reported in the literature. MRI and histopathology are of the essence to confirm this entity.
Enchondroma should be considered in differential diagnosis of lytic lesions of the femoral head. Timely diagnosis and proper surgery have good prognosis and prevent recurrence.
References
- 1.Dorfman DD, Bogdan C. Bone Tumours. St. Louis, MO: Mosby; 1998. p. 253-76. [Google Scholar]
- 2.Skinner HB. Current Diagnosis and Treatment in Orthopedics. New York: McGraw-Hill Medical; 2003. [Google Scholar]
- 3.Ferrer-Santacreu EM, Ortiz-Cruz EJ, González-López JM, Fernández EP. Enchondroma versus low-grade chondrosarcoma in appendicular skeleton: Clinical and radiological criteria. J Oncol 2012;2012:437958. [Google Scholar]
- 4.Sadiqi J, Rasouly N, Hamidi H, Siraj S. Radiographic features of Ollier’s disease-two case reports. BMC Med Imaging 2017;17:58. [Google Scholar]
- 5.Lewis RJ, Ketcham AS. Maffucci’s syndrome: Functional and neoplastic significance. Case report and review of the literature. J Bone Joint Surg Am 1973;55:1465-79. [Google Scholar]
- 6.Walden MJ, Murphey MD, Vidal JA. Incidental enchondromas of the knee. AJR Am J Roentgenol 2008;190:1611-5. [Google Scholar]
- 7.Burgener FA, Kormano M, Pudas T. Differential Diagnosis in Conventional Radiology. United States: Thieme; 2008. [Google Scholar]
- 8.Leal F, Nellensteijn JM, Frada R, Teixeira J, Queirós C, Padin M, et al. Arthroscopic treatment for femoral neck enchondroma: Case report. J Hip Preserv Surg 2015;2:428-30. [Google Scholar]
- 9.LeConte RG, Lee WE, Belk WP. Enchondroma of the femur with repeated recurrences and ultimate death. Arch Surg 1925;11:93-9. [Google Scholar]
- 10.Mori S, Miyazaki N, Inoue Y. A case report of the solitary enchondroma originating from neck of the femur. Orthop Traumatol 1986;35:377-9. [Google Scholar]
- 11.






