
To consider TO in the talus in the differential diagnosis in patients who underwent gastric sleeve surgery with bone pain.
Dr. E M S Badghish, Department of Surgery, Bisha University, Bisha, Saudi Arabia. E-mail: emran.b11@gmail.com
Introduction: Transient osteoporosis (TO) is a rare diagnosis usually observed in the hip and it is extremely rare to identify TO in the talar bone. Bariatric surgery and other weight loss treatments for obesity are linked to decreased bone mineral density and a possible risk factor of TO.
Case Report: A 42-year-old man, known case of gastric sleeve surgery 3 years back otherwise medically free, presented with unusual symptoms in an outpatient setting with on and off pain for the past 2 weeks that increased with walking and reduced by rest. Magnetic resonance imaging (MRI) of the left ankle 2-month post-pain showed diffused edema of the talus body and neck. He was diagnosed with TO and started the recommendation of nutritional supplementation therapy of calcium and Vitamin D. It was also advised to start protected weight bearing (pain free activity), and to wear air cast boot for at least 4 weeks. Only paracetamol was prescribed as pain relief medication and light activities for 6–8 weeks. At follow-up, 3 months after the MRI of the left ankle showed marked improvement and decrease of talar edema. At the final follow up, 9 months after the diagnosis, the patient presented a successful follow-up with no trace of edema nor pain.
Conclusion: TO is a rare disease and recognizing TO in the talus is extraordinary. The supplementation, protected weight bearing, and wearing air cast boot were effective in the management of our case, correlation between bariatric surgery and TO should be investigated.
Keywords: Transient osteoporosis, obesity, bariatric surgery, magnetic resonance imaging, talus.
Osteoporosis that spontaneously resolves is a defining feature of a self-limiting syndrome known as transient osteoporosis (TO) [1]. Men are more usually affected than women by the illness, which is typically encountered in middle-aged persons (40–70 years of age) [2]. It is a rare diagnosis which is commonly recognized in the hip region in men or during pregnancy [2]. The use of bariatric surgery has increased at least seven-fold globally in the past 10 years [3], making it the most effective treatment for obesity for attaining significant and long-lasting weight loss. Bariatric surgery has been shown to have a detrimental effect on bone health, as seen by raised bone turnover indicators and decreased bone mineral density (BMD), which speed up bone loss and increase skeletal fragility [4, 5, 6, 9]. In addition, 34–50% of people who complain of musculoskeletal pain are bariatric surgery candidates, who are overrepresented among people with musculoskeletal discomfort [7, 18]. Here, we present a rare case of unexplained foot and ankle pain followed bariatric surgery, and diagnosed with TO of the talus.
A 42-year-old man, known case of gastric sleeve 3 years back, presented to our clinic with the left ankle pain on and off which increased with walking and reduced by rest, and a limping gait for the past week. For the 1st time after the bariatric surgery, he went for a 30 min jog 2 weeks ago with no history of trauma. Post-sleeve he lost an approximate of 55 kg weighing from 153 kg to 98 kg. On examination, he had mild swelling at the dorsal aspect of the hind foot, decreased range of motion, tenderness on lateral aspect of left ankle, and intact neurovascular. The basic laboratory investigations were within normal range, including the erythrocyte sedimentation rate was 14 mm/h. (Normal: 0–15 mm/h.), and C-reactive protein was 6.23 (Normal: <10 mg/L). X-ray anterior posterior, mortise, and lateral view of the affected ankle illustrated apparent abnormalities (Fig. 1).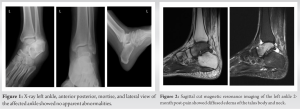 The patient was reassured and discharged from the clinic with a follow-up outpatient appointment after 4 weeks. The patient presented with the same complaints with even more pain, aggravated with walking. Magnetic resonance imaging (MRI) was arranged for the patient for the left ankle 2-month post pain, which showed diffused bone marrow edema of the talus body and neck (Fig. 2). According to MRI results and excluding other pathology, the patient was diagnosed with TO of the talus. It was recommended by the department to start the patient with nutritional supplementation therapy of calcium 650 mg daily and Vitamin D 50,000 IU weekly with no role for bisphosphonate or other bone resorptive initially. We also recommended protected weight bearing (pain free activity) and to wear an air cast boot to avoid complications. Paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) were prescribed as pain relief medication and he was recommended rest for 6–8 weeks. At follow-up, 3-month post-presentation following the previous recommendation, the patient could walk on air boot cast with reduction of pain to 50%, and the MRI of the left ankle showed marked improvement of talar edema (Fig. 3). At the final follow-up, 9 months after the diagnosis, the patient presented as pain free with no complaint.
The patient was reassured and discharged from the clinic with a follow-up outpatient appointment after 4 weeks. The patient presented with the same complaints with even more pain, aggravated with walking. Magnetic resonance imaging (MRI) was arranged for the patient for the left ankle 2-month post pain, which showed diffused bone marrow edema of the talus body and neck (Fig. 2). According to MRI results and excluding other pathology, the patient was diagnosed with TO of the talus. It was recommended by the department to start the patient with nutritional supplementation therapy of calcium 650 mg daily and Vitamin D 50,000 IU weekly with no role for bisphosphonate or other bone resorptive initially. We also recommended protected weight bearing (pain free activity) and to wear an air cast boot to avoid complications. Paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) were prescribed as pain relief medication and he was recommended rest for 6–8 weeks. At follow-up, 3-month post-presentation following the previous recommendation, the patient could walk on air boot cast with reduction of pain to 50%, and the MRI of the left ankle showed marked improvement of talar edema (Fig. 3). At the final follow-up, 9 months after the diagnosis, the patient presented as pain free with no complaint.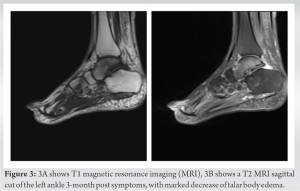
TO is a rare manifestation of bone marrow edema and the underlying cause is still unknown. Many theories have been illustrated regarding the pathophysiology and non are widely recognized [8]. Among successful bariatric patients, fast post-surgical weight loss of 55 kg is not unusual [10]. The time period during which weight loss is achieved is crucial [11], as it is associated with a higher risk of developing bone fatigue [10]. An exceedingly uncommon condition of the foot and ankle and a diagnosis of exclusion known as TO causes pain and swelling without any prior history of trauma [2, 12]. For MRI presentations of bone marrow edema, the radiological differential diagnosis is broad [2]. It is theorized that mechanical stress and bone bruising are examples of mechanically induced causes which highly correlates with our case. Reactive causes such as tumors, osteomyelitis, and reflex sympathetic dystrophy are examples of reactive causes. The other illnesses may typically be ruled out in cases with TO because they lack the corresponding clinical, laboratory, and radiological symptoms. Bone biopsy may be required in the few instances where there is still diagnostic uncertainty [2, 12]. Here, we presented a rare case of unexplained ankle pain following bariatric surgery, and diagnosed as TO, where his MRI showed diffused bone marrow edema of the talus without history of trauma. Synovial fluid analysis and other laboratory results of TO are typically unremarkable [13]. Regarding our case, the laboratory investigations were within normal range. Mechanical, hormonal, and malabsorptive variables are some of the possible mechanisms behind decreases in bone density and strength brought on by weight loss that may cause bone edema [14]. Sclerostin levels rise as a result of the reduction in pressure on bones brought on by weight loss, which suppresses osteoblastic activity and bone formation [14], whereas markers of bone turnover significantly rise [14]. Supplementation, such as Vitamin D supplementation, may be necessary to prevent secondary hyperparathyroidism as a result of malabsorption of micronutrients such as Vitamin D, protein, and calcium, especially following specific bypass procedures [15]. In addition, historically, conservative techniques have been used to treat temporary localized osteoporosis, such as shielded weight-bearing to prevent pain and stress fractures and the administration of analgesics and NSAID to relieve symptoms. In more recent times, oral and injectable bisphosphonate medications have been successfully utilized to ease symptoms and speed up ambulation, especially in patients with refractory instances and those who also have widespread osteoporosis [16]. Regarding our case, we recommended the patient for protected weight bearing (pain free activity), wearing an air boot cast when weight bearing, and to start nutritional supplementation therapy of calcium and Vitamin D supplementation with no role for bisphosphonate or other bone resorptive. Although it is advised that patients take additional nutrient supplements after bariatric surgery [14], compliance is low. For example, Vitamin D supplementation has been reported to be as low as 33% at 1 year [15], with factors like male sex and full-time employment associated with poor compliance [17]. When BMD loss caused by these factors is combined with a rapid increase in physical activity in an adult who had previously been sedentary, it may put the bone under more stress and increase the likelihood of such pathology [10]. Luckily, we mismatched with these studies where after 3 months, our case could walk on an air cast boot with reduction of pain to 50%, and the MRI of the left ankle showed marked improvement of talar edema, and at the final follow-up, 9 months after the diagnosis, the patient presented with no complaint. It is highly important to further investigate the correlation of bariatric surgery and TO as there could be a significant associative factor.
TO of the talus is a unique case with limited resources in the literature. MRI is the main tool to diagnose TO. We believe that there could be a frank correlation between TO and bariatric surgery. Further investigation on the correlation of bariatric surgery and TO should be considered.
TO is a rare diagnosis found usually in the hip; however, talar bone is also involved in extremely rare occasions. Considering bariatric surgery could be an associate factor for TO, further research is needed to identify correlation.
References
- 1.Korompilias AV, Karantanas AH, Lykissas MG, Beris AE. Transient osteoporosis. J Am Acad Orthop Surg 2008;16:480-9. [Google Scholar]
- 2.Froberg PK, Braunstein EM, Buckwalter KA. Osteonecrosis, transient osteoporosis, and transient bone marrow edema: Current concepts. Radiol Clin North Am 1996;34:273-91, X. [Google Scholar]
- 3.Angrisani L, Santonicola A, Iovino P, Vitiello A, Zundel N, Buchwald H, et al. Bariatric surgery and endoluminal procedures: IFSO worldwide survey 2014. Obes Surg 2017;27:2279-89. [Google Scholar]
- 4.McGee DL, Diverse Populations Collaboration. Body mass index and mortality: A meta-analysis based on person-level data from twenty-six observational studies. Ann Epidemiol 2005;15:87-97. [Google Scholar]
- 5.Hachem A, Brennan L. Quality of life outcomes of bariatric surgery: A systematic review. Obes Surg 2016;26:395-409. [Google Scholar]
- 6.Bond DS, Vithiananthan S, Nash JM, Thomas JG, Wing RR. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology 2011;76:1135-8. [Google Scholar]
- 7.Speck RM, Bond DS, Sarwer DB, Farrar JT. A systematic review of musculoskeletal pain among bariatric surgery patients: Implications for physical activity and exercise. Surg Obes Relat Dis 2014;10:161-70. [Google Scholar]
- 8.Chowdhury FU, Robinson P, Grainger AJ, Harris N. Transient regional osteoporosis: A rare cause of foot and ankle pain. Foot Ankle Surg 2006;12:79-83. [Google Scholar]
- 9.Zibellini J, Seimon RV, Lee CM, Gibson AA, Hsu MS, Shapses SA, et al. Does diet‐induced weight loss lead to bone loss in overweight or obese adults? A systematic review and meta‐analysis of clinical trials. J Bone Miner Res 2015;30:2168-78. [Google Scholar]
- 10.Ablett AD, Boyle BR, Avenell A. Fractures in adults after weight loss from bariatric surgery and weight management programs for obesity: Systematic review and meta-analysis. Obes Surg 2019;29:1327-42. [Google Scholar]
- 11.Haria DM, Sibonga JD, Taylor HC. Hypocalcemia, hypovitaminosis D osteopathy, osteopenia, and secondary hyperparathyroidism 32 years after jejunoileal bypass. Endocr Pract 2005;11:335-40. [Google Scholar]
- 12.Gunaratne I, Singh P, Dega R. Transient migratory osteoporosis of the foot. Foot Ankle Surg 2007;13:51-4. [Google Scholar]
- 13.Gagnon C, Schafer AL. Bone health after bariatric surgery. JBMR Plus 2018;2:121-33. [Google Scholar]
- 14.Bal BS, Finelli FC, Shope TR, Koch TR. Nutritional deficiencies after bariatric surgery. Nat Rev Endocrinol 2012;8:544-56. [Google Scholar]
- 15.Judd DB, Kim DH, Hrutkay JM. Transient osteoporosis of the talus. Foot Ankle Int 2000;21:134-7. [Google Scholar]
- 16.Thereaux J, Lesuffleur T, Païta M, Czernichow S, Basdevant A, Msika S, et al. Long-term follow-up after bariatric surgery in a national cohort. J Br Surg 2017;104:1362-71. [Google Scholar]
- 17.Schapira D, Gutierrez G, Mor M, Nahir AM. Successful pamidronate treatment of severe and refractory regional migratory osteoporosis. J Clin Rheumatol 2001;7:188-90. [Google Scholar]
- 18.Badghish EM, Alsulaimany HH, Schotanus M. A case report and literature analysis: A supracondylar femur fracture in a super-obese patient. J Orthop Case Rep 2019;9:30-3. [Google Scholar]



