
Spinal masses can pose an enigma even with best clinical explanations, and though not common, IgG4-related tumors must be within our horizon of possible etiology.
Dr. Abhijeet Kumar Agrawal, Department of Rheumatology, Max Hospital, Saket, New Delhi, India. E-mail: abhijeet1289x55xx@proton.me
Abstract
Introduction: Immunoglobulin (Ig)G4-related disease belongs to a rare compilation of conditions in rheumatology and may involve a multitude of organs. Amidst the central nervous system (CNS) presentation, involvement of spinal cord is rarer still.
Case Report: A 50-year-old male came with chief complaints of tingling sensation over both soles since 2 months associated with lower back ache and gait disturbance in the form of spastic gait. X-rays of spine were suggestive of a growth at the level of D10–D12 compressing the spinal cord with no focal sclerotic/lytic lesions, and MRI dorsolumbar spine showed dural tail sign. The patient underwent excision of dural mass, and histopathology revealed majority of plasma cells positive for IgG4. Case 2: A 65-year-old female came with complaints of cough, shortness of breath, and fever on and off since 2 months. No history of hemoptysis, purulent sputum, weight loss. On examination: There were bilateral rhonchi in the left upper zone. MRI spine showed focal erosion with soft-tissue thickening at the right paravertebral region extending from D5-9. The patient underwent surgery (fusion D6-8 and ostectomy D7 posterior rib resection D7 right side) with the right pleural biopsy and transpendicular intracorporal biopsy D7. Histopathology was compatible with findings of IgG4 disease.
Discussion: IgG4 tumors presenting in CNS itself is rare and rarer in spinal cord. Histopathological examination is central to diagnose and prognosticate the disease further as IgG4-related disease manifestations may recur without proper treatment.
Keywords: IgG4, spinal mass, central nervous system, pleura.
Immunoglobulin (Ig)G4-related disease belongs to a rare compilation of conditions in rheumatology, its varied manifestation make it a diagnostic challenge among other lesions which more frequently present as mass lesions [1]. The multitude of organs that are affected in IgG4-related disease commonly includes salivary glands, pancreas, liver, lungs, heart, and kidney [2,3]. However, the facade of central nervous system (CNS) manifestations in IgG4-related disease makes them mystifying and is less documented [4]. Amidst the CNS presentation, involvement of spinal cord is rarer still. These patients initially land up in specialties such as orthopedics, neurology, neurosurgery, and oncosurgery given that the mass lesions closely mimic any other and much prevalent mass like lesions. CNS involvement customarily affects meninges or parenchyma of the brain [5]. We present two cases, which presented in the departments of orthopedics and respiratory medicine; one underwent surgery on assumption of meningioma and was diagnosed post-surgery through histopathological examination and found to be IgG4-related mass affecting the spinal cord. The other manifested as pleura-based paraspinal mass later found to be IgG4-related mass.
A 50-year-old male came with chief complaints of tingling sensation over both soles since 2 months associated with the lower back ache which was non radiating, not associated with any log such as sensation over bilateral lower limbs, slipping of slippers, no weakness or tingling sensation in the upper limbs, and negative Lhermitte’s sign. No history of any band like sensation over abdomen. The patient had an associated gait disturbance in the form of spastic gait. History was not suggestive of any trauma in the back or fever. The patient was evaluated by both neurology and orthopedics department. On examination, no obvious swelling was seen in the back with tenderness at thoracolumbar region. Blood reports did not suggest any obvious infection with hemogram being normal. X-rays of spine were suggestive of a growth at the level of D10–D12 compressing the spinal cord with no focal sclerotic/lytic lesions, normal bone density, normal disk space, and no paravertebral soft-tissue abnormalities. MRI dorsolumbar spine showed dural tail sign (Fig. 1). The patient was then operated, underwent laminectomy, excision of dural mass, and reconstruction with dorsolumbar fascia along with pedicle screw fixation in July 2021 (Fig. 2a). The resected mass was sent for histopathological examination with provisional diagnosis of “Meningioma” (Fig. 2b). 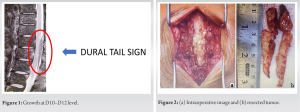 Histopathological examination of the grey-white soft-tissue bits (5.5 × 3 × 1.5 cm) sample revealed densely infiltrated by lymphoplasmacytic cells and histiocytes with presence of a few scattered multinucleated Langerhans giant cells and occasional ill formed epithelioid cell granuloma. No necrosis was seen. Pathologists confirmed a plasma rich lymphoplasmacytic infiltration possibly IgG4-related disease. Immunohistochemistry of the sample showed:
Histopathological examination of the grey-white soft-tissue bits (5.5 × 3 × 1.5 cm) sample revealed densely infiltrated by lymphoplasmacytic cells and histiocytes with presence of a few scattered multinucleated Langerhans giant cells and occasional ill formed epithelioid cell granuloma. No necrosis was seen. Pathologists confirmed a plasma rich lymphoplasmacytic infiltration possibly IgG4-related disease. Immunohistochemistry of the sample showed:
- Majority of plasma cells positive for IgG4
- Diffuse infiltrate of CD3 positive T-cells
- Nodular infiltrate of CD20 positive B-cells
- CD138 marked plasma cells
- Plasma cells positive for kappa and lambda light chains.
However, serum IgG4 estimation could not be done due to financial constraints. The patient was then referred to rheumatology department for further workup and medical management. The patient gave no history of any other symptoms pertaining to IgG4 disease and was subsequently started on methotrexate and glucocorticoids. The patient is on regular follow-up and has had no relapse or new manifestations.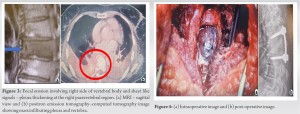
Case No. 2
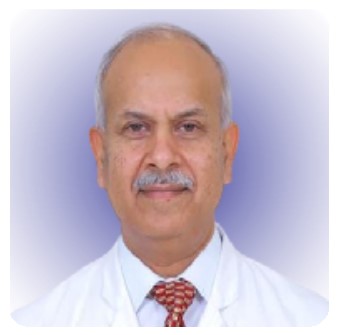
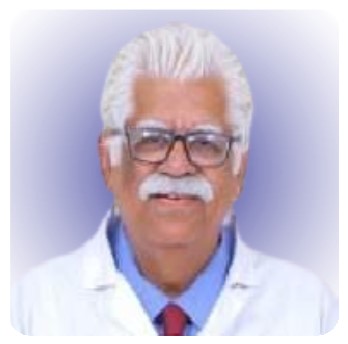
A 65-year-old female came with complaints of cough, shortness of breath, and fever on and off since 2 months. No history of hemoptysis, purulent sputum, and weight loss. On examination: There were bilateral rhonchi in the left upper zone with no other significant systemic findings. Initial investigations showed Hb – 9.3 g/dL, total leukocyte count – 13.4/µL, platelets – 1,66000/µL, serum albumin – 3.1 g/dL, c3 – 201, c4 – 30, serum procalcitonin – 0.187 ng/ml, and CRP – 139 mg/dL. On imaging, CT thorax was suggestive of paravertebral mass and bilateral pleural effusion with bronchiectatic changes. The biopsy of paravertebral mass showed inflammatory changes. The patient was initially started on i.v. antibiotics and supportive treatment, but the fever persisted. The patient was started on anti-tubercular drugs empirically. Subsequent PET scan showed lower lobe mass infiltrating pleura and eroding the adjacent vertebra (D7) (Fig. 3b) with uptake in the left supraclavicular lymph node. MRI spine showed focal erosion involving right side of vertebral body and sheet like signal suggestive of soft-tissue thickening at the right paravertebral region extending from D5-9 (Fig. 3a). Pleural fluid analysis was negative for malignant cells. Bronchoalveolar lavage showed no organisms. Supraclavicular lymph node showed reactive lymphadenitis. The patient underwent surgery (fusion D6-8 and ostectomy D7 posterior rib resection D7 right side) with the right pleural biopsy and transpendicular intracorporal biopsy D7 (Fig. 4a and b). The biopsy later revealed lymphoplasmacytic infiltrates with IgG4 cells with IHC showing majority of plasma cells to be IgG4 positive. Serum IgG4 levels too were raised. The patient was subsequently referred to rheumatology department for further management and no other organ involvement is documented since.
IgG4-related disorders belong to a conglomeration of conditions, although with different presentation yet having similar histopathological findings, the central features being presence of lymphoplasmacytic infiltrates along with storiform fibrosis and obliterative phlebitis [6]. Laboratory analysis may reveal eosinophilia, raised IgG4 levels, hypergammaglobulinemia, hypocomplementemia, and raised IgE levels in serum. Often due to varied manifestations these patients land up in different subspecialties, the amalgamation of each of these subspecialties usually occurs after histopathological analysis showing typical features of IgG4 diseases. IgG4-related disease involving CNS is particularly rare and rarer, which is the instance of spinal involvement in such patients [7]. Winkel et al. presented a case of 48-year-old female, 8 weeks of lower back pain, neurogenic claudication, and right lower extremity radiculopathy. MRI of her lumbar spine with and without contrast showed an enhancing extradural mass at the L2–L3 level extending into the right neural foramen, contributing to severe central and right L2–L3 foraminal stenosis. The tumor was debulked, and specimen sent to histopathology which showed lymphoplasmacytic and histiocytic inflammatory infiltrate with marked stromal fibrosis and a large number of IgG4+ plasma cells with an IgG4/IgG ratio of 27% [8]. Rumalla et al. reported a female patient with neck pain for 4 months duration and associated weakness both upper limbs. Cervical spine MRI revealed paraspinal infiltrate and a mass extending from C4 to T1. Histological examination showed areas of lymphoplasmacytic infiltrates and fibrosis along with obliterative phlebitis [9]. Zhang et al. described a 39 years male, with short history of backache and lower limb weakness showed abnormal MRI signals from C5 to T4 segments. CSF IgG was 718.0 mg/L. Thoracic MRI showed similar altered signals from T1 to T6 segments. Histopathological examination confirmed IgG4-related spinal pachymeningitis [10]. Another case showed, a case of a 76-year-old male with IgG4-related disease presenting primarily with vertebral bone marrow lesions. Histopathology showed the typical features of storiform fibrosis, and increased IgG4 positive plasma cells. Treatment with corticosteroids significantly improved well-being resolved lesion size on MRI [4]. Our cases, however, revealed masses in the thoracic spine and histopathology revealed lymphoplasmacytic infiltrates with histiocytes, plasma cells positive for IgG4 levels. One case had raised serum IgG4 levels, and in another case, serum IgG4 levels could not be done due to financial constraints.
IgG4-related diseases can present in a dicey way, wherein they may mimic much commoner tumor pathologies. Depending on their site of presentation, there can be a wide array of clinical features. IgG4 tumors presenting in CNS itself is rare and rarer in spinal cord. Hence, it actually comes down to the histopathological examination to draw the last straw and give clinicians the accurate etiology and hence helping them to prognosticate the disease further as IgG4-related disease manifestations may recur without proper treatment.
Histopathological diagnosis of every spinal tumor is a must, as the prognosis and further management may depend on the etiology of the tumor.
References
- 1.Williams MM, Mashaly H, Puduvalli VK, Jin M, Mendel E. Immunoglobulin G4-related disease mimicking an epidural spinal cord tumor: Case report. J Neurosurg Spine 2017;26:76-80. [Google Scholar | PubMed]
- 2.Qi Z, Liu J, Li G, Zhang Y. Immunoglobulin G4-related spinal intramedullary inflammatory pseudotumor: A case report and literature review. Front Neurol 2022;13:878414. [Google Scholar | PubMed]
- 3.Abdulla E, Luther H, Shah T, Chandran N. Immunoglobulin G4-related disease masquerading an epidural spinal cord tumor. J Neurosci Rural Pract 2021;12:424-6. [Google Scholar | PubMed]
- 4.Van den Elshout-den Uyl D, Spoto CP, de Boer M, Leiner T, Leavis HL, Leguit RJ. First report of IgG4 related disease primary presenting as vertebral bone marrow lesions. Front Immunol 2019;10:1910. [Google Scholar | PubMed]
- 5.Merza N, Taha A, Lung J, Benderman AW, Wright SE. IgG4-related sclerosing disease causing spinal cord compression: The first reported case in literature. Case Rep Immunol 2019;2019:3618510. [Google Scholar | PubMed]
- 6.Stone JH, Brito-Zerón P, Bosch X, Ramos-Casals M. Diagnostic approach to the complexity of IgG4-related disease. Mayo Clin Proc 2015;90:927-39. [Google Scholar | PubMed]
- 7.Li HX, Zuo L, Peng XX, Zong Q, Zhang K, Liu YZ, et al. Immunoglobulin G4-related hypertrophic pachymeningitis with spinal cord compression: A case report. J Neuroimmunol 2020;347:577325. [Google Scholar | PubMed]
- 8.Winkel M, Lawton CD, Sanusi OR, Horbinski CM, Dahdaleh NS, Smith ZA. Neuro-surgical considerations for treating IgG4-related disease with rare spinal epidural compression. Surg Neurol Int 2018;9:209. [Google Scholar | PubMed]
- 9.Rumalla K, Smith KA, Arnold PM. Immunoglobulin G4-related epidural inflammatory pseudotumor presenting with pulmonary complications and spinal cord compression: Case report. J Neurosurg Spine 2017;26:688-93. [Google Scholar | PubMed]
- 10.Zhang R, Gao J, Zhao T, Zhang B, Wang C, Wang C, et al. A case with IgG4-related spinal pachymeningitis causing spinal cord compression. Front Neurol 2020;11:500. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 A Rare Case of Shoulder Tuberculosis Managed with Anti-tuberculosis Treatment and Antibiotic Coated Cement Spacer
May 1, 2025 A Rare Case of Shoulder Tuberculosis Managed with Anti-tuberculosis Treatment and Antibiotic Coated Cement Spacer March 1, 2026 Primary Intraosseous Malignant Nerve Sheath Tumor of Humerus Presenting With Pathological Fracture: A Rare Case Report With Review of Literature
March 1, 2026 Primary Intraosseous Malignant Nerve Sheath Tumor of Humerus Presenting With Pathological Fracture: A Rare Case Report With Review of Literature December 10, 2022 Medial Meniscus Posterior Root Reconstruction and Open-Wedge High Tibial Osteotomy for Medial Meniscus Posterior Root Tear with Varus Knee: A Case Report
December 10, 2022 Medial Meniscus Posterior Root Reconstruction and Open-Wedge High Tibial Osteotomy for Medial Meniscus Posterior Root Tear with Varus Knee: A Case Report April 10, 2021 Holistic Approach in the Management of Skeletal Deformity in a Case of Homocystinuria
April 10, 2021 Holistic Approach in the Management of Skeletal Deformity in a Case of Homocystinuria