
Osteoid osteoma may be a rare cause of unresolved joint pain and effusion. Uncommon location such as the subperiosteal region and adjacent to a joint warrants careful clinical and radiological assessment for the appropriate diagnosis and successful treatment.
Dr. Ganesh Singh Dharmshaktu, Department of Orthopaedics, Government Medical College, Haldwani, Uttarakhand, India. E-mail: drganeshortho@gmail.com
Abstract
Introduction: The elbow pain and restricted movement is a nagging problem and elbow arthropathies need to be excluded. On rare instances, uncommon etiology like a benign lesion is the culprit and the diagnosis would require judicious clinicoradiological correlation. Osteoid osteoma in the intra- or juxta-articular region is reported in the literature as rare, sporadic report.
Case Report: A 23-year-old, Indian male patient presented with a provisional diagnosis of early elbow arthropathy on account of unexplained pain and restricted elbow movement without a history of trauma. He was subjected to appropriate investigations revealing synovial hypertrophy, effusion, and bone edema suggestive of early arthropathy. Additional imaging led to an uncommon definitive diagnosis. An intra-articular osteoid osteoma was found over the medial aspect of the coronoid fossa with a thin rim of cortical rim projecting anteriorly. The lesion was diagnosed and delineated on computerized tomography and an open excision of the lesion and synovectomy was done for histopathological evaluation. Histology confirmed the presence of an osteoid osteoma at an uncommon location.
Conclusion: The careful appreciation of radiological images is critical to not miss significant etiology that may mimic non-specific elbow pain. High index of suspicion coupled with appropriate diagnostic imaging results in early diagnosis and appropriate management. Osteoid osteoma should be a differential diagnosis in cases with pain and restricted elbow movement and excision of which results in recovery of painless range of motion.
Keywords: Elbow, osteoid osteoma, arthritis, coronoid fossa, elbow pain.
Osteoid osteoma is usually a diphyseal, bone-forming, benign lesion affecting the lower extremity in half of the cases [1]. The distal humerus involvement within the elbow joint is an uncommon site for an osteoid osteoma [1,2]. The diagnosis is mostly delayed and often patients have long-standing symptoms and many undergo various tests or procedures before reaching the definitive diagnosis. Restricted elbow range of motion or flexion contracture is common presentation as noted in a large series of elbow osteoid osteoma cases [2]. There may be non-specific clinical features and the characteristic night pain relieved on taking non-steroidal anti-inflammatory drugs may or may not be noted in every case. The use of advance imaging modalities such as computerized tomography (CT) scan or magnetic resonance imaging (MRI) is warranted to identify the lesion, often missed on plain radiographs. Lesions in the juxta-articular or intra-articular location pose further diagnostic challenge due to many differentials for pain and limited movement to exclude [3]. The involvement of the coronoid or olecranon fossa and mimicking early elbow arthritis is uncommon presentation and should be considered as a rare cause of unexplained elbow arthritis in adolescents or young adults [4]. Besides it, cases showing minimal cortical sclerosis pose a diagnostic dilemma [5]. The subperiosteal location in the distal humerus in the intra-articular region is even more uncommon. High index of suspicion and identification of the lesion in the imaging is critical for the appropriate management and good functional outcome.
A 23-year-old male patient presented to us with complaints of atraumatic right elbow pain and restriction of movement for the past 6 and 3 months, respectively. The movement restriction, especially the flexion, was noticed gradually increasing over the past month. For pain, he used to take medicine on need basis from a local practitioner leading to transient relief. Pain, however, had no diurnal variation or association with activities. He was advised MRI of the elbow on account of recurrent pain, the reason for his visit to us. On examination, there was mild swelling around the elbow and anterior elbow tenderness. The active movement of extension was intact but active flexion was restricted and only ninety degree of passive elbow flexion was possible. There was no localized elevation of temperature and distal neurovascular status was intact. There was neither any other joint involvement nor any systemic comorbidity associated. The radiographs of the elbow in initial period did not show any significant abnormality except a small fleck of radio-opacity noted anterior to the distal humerus (Fig. 1). 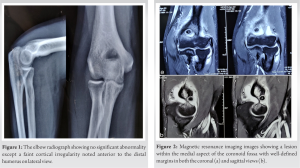 MRI was done to better delineate the etiology and showed effusion in the elbow joint with edema in the bones around the distal humerus. The MRI images were suggestive of elbow arthropathy and considering monoarticular involvement and synovial hypertrophy, a provisional diagnosis of elbow tuberculosis was made. On closer inspection of images, however, a round defect was noted adjacent to the coronoid fossa on its medial aspect, as a clearly evident anomaly on both sagittal and axial images (Fig. 2 and 3a).
MRI was done to better delineate the etiology and showed effusion in the elbow joint with edema in the bones around the distal humerus. The MRI images were suggestive of elbow arthropathy and considering monoarticular involvement and synovial hypertrophy, a provisional diagnosis of elbow tuberculosis was made. On closer inspection of images, however, a round defect was noted adjacent to the coronoid fossa on its medial aspect, as a clearly evident anomaly on both sagittal and axial images (Fig. 2 and 3a).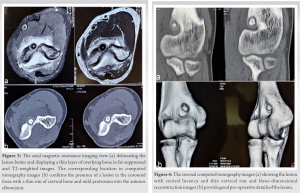 A CT scan better delineated the lesion as a small bony lesion with an overlying thin cortical rim, abutting the coronoid fossa, and protruding anteriorly into the elbow joint (Fig. 3b and 4). Joint effusion and edema corresponding to the area in distal humerus were also noted. The lesion with a rim was considered as an osteoid osteoma and the confirmatory exploration and sample collection for biopsy was planned. The elbow was explored by an anterior approach with a 5-cm longitudinal incision centered over the coronoid fossa under tourniquet. The area near coronoid fossa revealed a protruding bony mass with thin rim of bone in the medial aspect of the fossa (Fig. 5a).
A CT scan better delineated the lesion as a small bony lesion with an overlying thin cortical rim, abutting the coronoid fossa, and protruding anteriorly into the elbow joint (Fig. 3b and 4). Joint effusion and edema corresponding to the area in distal humerus were also noted. The lesion with a rim was considered as an osteoid osteoma and the confirmatory exploration and sample collection for biopsy was planned. The elbow was explored by an anterior approach with a 5-cm longitudinal incision centered over the coronoid fossa under tourniquet. The area near coronoid fossa revealed a protruding bony mass with thin rim of bone in the medial aspect of the fossa (Fig. 5a). The lesion was carefully excised en bloc from the underlying bone and was easily detached owing to its superficial location on the bone (Fig. 5b). The debridement of the adjacent bony and articular area and synovectomy was done and the joint was given a thorough lavage. The wound was then closed in layers followed by a protection elbow plaster slab. The post-operative period was uneventful and there was marked reduction in pain and gradual decrease in the swelling in coming days. The histopathology confirms the presence of an osteoid osteoma (Fig. 5c and d). The slab was removed after 2 weeks and the elbow range of motion exercises started. The patient had good wound healing (Fig. 6a) and full range of motion in flexion (Fig. 6b) and extension (Fig. 6c) with good radiological improvement in the follow-up at 4 months.
The lesion was carefully excised en bloc from the underlying bone and was easily detached owing to its superficial location on the bone (Fig. 5b). The debridement of the adjacent bony and articular area and synovectomy was done and the joint was given a thorough lavage. The wound was then closed in layers followed by a protection elbow plaster slab. The post-operative period was uneventful and there was marked reduction in pain and gradual decrease in the swelling in coming days. The histopathology confirms the presence of an osteoid osteoma (Fig. 5c and d). The slab was removed after 2 weeks and the elbow range of motion exercises started. The patient had good wound healing (Fig. 6a) and full range of motion in flexion (Fig. 6b) and extension (Fig. 6c) with good radiological improvement in the follow-up at 4 months. No recurrence of the lesion or any complication associated were seen in the follow-up of further 9 months.
No recurrence of the lesion or any complication associated were seen in the follow-up of further 9 months.
Pain and limited movement are common complaints and many of these cases with non-specific symptoms witness a delay in the definitive diagnosis. Many are misdiagnosed and treated for synovial disorder, enthesopathy, or sequela of old trauma [6]. Juxta- and intra-articular osteoid osteoma are rare lesions and may arise from any joint but common reported locations are hip, elbow, and talus. Intra-articular lesions, when subperiosteal, may encroach into the joint and present with features of mono-articular arthritis with swelling, pain, and limited joint movements. A case very similar to ours with a subperiosteal lesion having thin cortical shell in the coronoid fossa was reported [7]. Excision of the lesion resulted in marked clinical improvement. Osteoid osteoma has been described as a self-limiting disorder and spontaneous healing is also reported but cases with joint involvement require early treatment and are usually not candidate for conservative expectant management. Thermal ablation by percutaneous radiofrequency (RF) leads to thermal coagulation and induces localized necrosis. This can be an optional management method that is minimal invasive and works well in difficult locations [8]. Arthroscopy-based interventions such as excision, curettage, debridement, and synovectomy have also been frequently reported in recent times [5,6,7,9]. In a recent systematic review, successful outcomes in the range of 93.8% along with zero post-operative complication and recurrence rate have been reported [10]. Major differentials include inflammatory arthritis, seronegative spondyloarthropathy, crystal deposition disorder, infective lesion like Brodie’s abscess, or tuberculosis in endemic regions [11]. Many cases undergo physical therapy and steroid injections for the elbow pain and consult only when conservative treatment fails [12,13]. The presence of lesion is also reported in pediatric elbow (here olecranon fossa is common location) with pain and flexion-extension contracture in the presence of normal prono-supination [14]. Potential complications of childhood intra-articular osteoid osteoma-like skeletal abnormalities and joint movement problems necessitate appropriate diagnosis and treatment [15]. Acknowledgment of an osteoid osteoma in cases with long-standing elbow pain and stiffness as rare etiology should be done to avoid delay in the diagnosis and mismanagement.
This case underlines the importance of careful interpretation of radiological findings to arrive at the diagnosis in a case with unexplained painful restriction of movement. It also highlights that characteristic night pain responding to pain medication may not be found in all cases with osteoid osteoma. Excision leading to full recovery by open methods is a viable option in resource-limited areas where RF ablation or arthroscopic tools are not widely available.
Acknowledgment of the subperiosteal region, as the rare location for the osteoid osteoma, is important for appropriate diagnosis with the help of judicious use of clinical judgment and advanced imaging methods.
References
- 1.Healey JH, Ghelman B. Osteoid osteoma and osteoblastoma. Current concepts and recent advances. Clin Orthop 1986;204:76-80. [Google Scholar | PubMed]
- 2.Weber KL, Morrey BF. Osteoid osteoma of the elbow: A diagnostic challenge. J Bone Joint Surg Am 1999;81:1111-9. [Google Scholar | PubMed]
- 3.Franceschi F, Marinozzi A, Papalia R, Longo UG, Gualdi G, Denaro E. Intra-articular and juxta-articular osteoid osteoma: A diagnostic challenge: Misdiagnosis and successful treatment: A report of four cases. Arch Orthop Trauma Surg 2006;126:660-7. [Google Scholar | PubMed]
- 4.Fukuda R, Matsuoka M, Kawamura D, Endo T, Kanno-Okada H, Urita A, et al. Intra-articular osteoid osteoma at the elbow mimicking arthritis: A case report. Ann Joint 2022;7:20. [Google Scholar | PubMed]
- 5.Alrassasi YM, Almustafa MA, Al Eid ZM, Albattat MY, Al Batran KI. A rare case of intra-articular osteoid osteoma of the elbow managed with arthroscopic excision. Cureus 2021;13:e155666. [Google Scholar | PubMed]
- 6.Segura JF, Barrera-Ocha S, Gargallo-Margarit A, Correa-Vazquez E, Isart-Torruella A, Bullo XM. Osteoid osteoma of the distal humerus mimicking sequela of paediatric supracondylar fracture: Arthroscopic resection- Case report and a literature review. Case Rep Med 2013;2013:247328. [Google Scholar | PubMed]
- 7.Goyal T, Pandita N, Paul S. Arthroscopic excision of intra-articular subperiosteal osteoid osteoma of elbow: A case report. SICOT J 2018;4:25. [Google Scholar | PubMed]
- 8.Motamedi D, Learch TJ, Ishimitsu DN, Motamedi K, Katz MD, Brien EW, et al. Thermal ablation of osteoid osteoma: Overview and step-by-step guide. RadioGraphics 2009;29:2127-41. [Google Scholar | PubMed]
- 9.Hatta T, Hosaka M, Watanuki M, Yano T, Yoshida S, Watanabe M, et al. Arthroscopic excision of intra-articular osteoid osteoma at the elbow. Case Rep Orthop 2019;2019:8505382. [Google Scholar | PubMed]
- 10.Ge SM, Marwan Y, Abduljabbar FH. Arthroscopic management of intra-and juxta-articular osteoid osteoma of the upper extremity: A systematic review of the literature. Eur J Orthop Surg Traumatol 2020;30:1333-44. [Google Scholar | PubMed]
- 11.Jisam MJ, Kandathil JC, Jalal MJ, Manuel E, Chervil B. Osteoid osteoma masquerading mono arthritis of the elbow. Clin Rheumatol 2022;41:313-4. [Google Scholar | PubMed]
- 12.Yano K, Kaneshiro Y, Sakanaka H. Arthroscopic excision for intra-articular osteoid osteoma of the olecranon fossa: A case report and literature review. Case Rep Orthop 2020;2020:4034989. [Google Scholar | PubMed]
- 13.Westbom CM, Nolan JE III, Morrell NT. Intra-articular osteoid osteoma of the elbow: A case report. Western J Orthop 2020;9:160-3. [Google Scholar | PubMed]
- 14.Cassard X, Accadbled F, de Gauzy JS, Cahuzac JP. Osteoid osteoma of the elbow in children: A report of three cases and a review of the literature. J Pediatr Orthop 2002;11:240-4. [Google Scholar | PubMed]
- 15.Song MH, You WJ, Cho TJ, Chung CY, Park MS, Cheap JE, et al. Clinical and radiological features and skeletal sequelae in childhood intra-/juxta-articular versus extra-articular osteoid osteoma. BMC Musculoskelet Disord 2015;16:3. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2021 Arthroscopic Excision of an Intra-articular Osteoid Osteoma in the Trochlear Notch of Ulna – A Case Report
March 10, 2021 Arthroscopic Excision of an Intra-articular Osteoid Osteoma in the Trochlear Notch of Ulna – A Case Report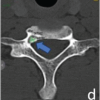 August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report
August 1, 2026 O-arm Navigation-assisted Excision of Cervical Osteoid Osteoma Adjacent to the Vertebral Artery: Technical Note and Case Report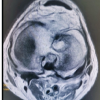 August 1, 2026 Sub-acute Septic Arthritis of the Knee by Candida vishwanathii: Two Rare Case Reports and Review of Literature
August 1, 2026 Sub-acute Septic Arthritis of the Knee by Candida vishwanathii: Two Rare Case Reports and Review of Literature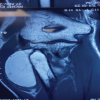 August 1, 2026 A Bilobed Lipoma Presenting in the Post-Excision Space of the Radial Head 5 Years after Radial Head Excision: A Case Report
August 1, 2026 A Bilobed Lipoma Presenting in the Post-Excision Space of the Radial Head 5 Years after Radial Head Excision: A Case Report