
Although rare but bifid tibialis anterior tendon is a possibility in congenital talipes equinovarus which needs to be addressed.
Dr. Rajan Gupta, Department of Orthopaedics, LTMMC and GH, Sion, Mumbai, India, Email- rajan4gupta@gmail.com
Abstract
Introduction: Idiopathic congenital talipes equinovarus (CTEV) is one of the most extensively researched topics for decades. It has been associated with various musculoskeletal anomalies which maybe bony, vascular or involving the ligaments and muscles which may have a direct or indirect impact on its pathoanatomy. This report describes an unusual presentation of a bifid tibialis anterior tendon (TAT) in a case of CTEV. This is the first report of this kind in the literature to the best of our knowledge.
Case Report: A 4-year-old female presented with bilateral relapsed CTEV with dynamic supination previously treated with standard Ponseti protocol. The patient was treated with TAT transfer on the left side with a rare presentation of a bifid TAT where both the slips of the tendon were transferred to dorsum of the foot onto the lateral cuneiform.
Conclusion: When treating a patient of CTEV surgically, it is important to consider the possibility of a bifid TAT which is a rare musculoskeletal association. It is recommended to carefully dissect TAT to prevent under correction of the deformity in case either one of the tendon slips remains attached to its original site.
Keywords: Congenital talipes equinovarus, bifid tibialis anterior tendon, tibialis anterior tendon transfer.
Clubfoot is one of the most common anomalies found in approximately 1 in 1000 live births. It was introduced in the medical literature in 400 BC by Hippocrates [1] and has been extensively researched but still lacks a clear understanding about the etiology, pathogenesis, treatment, and other associated anomalies which commonly include congenital muscular torticollis, congenital dislocation of hip, absences of tarsal bones, polydactyly, and many others. We present a case through which we wish to report a bifid tibialis anterior tendon (TAT) with an implication on the treatment of a relapsed clubfoot with dynamic supination treated with TAT transfer.
A 4-year-old female child referred to congenital talipes equinovarus (CTEV) clinic at a tertiary care center with complaints of recurrent clubfoot. She was a diagnosed case of idiopathic CTEV since birth, treated with Ponseti protocol of serial casting, tenotomy, and bracing. She had a normal perinatal history with no significant family/sibling history. The patient had been non-compliant to bracing protocol and lost to follow-up which accounts for the relapsed clubfoot. On examination, both the feet had passively correctible forefoot adduction with cavus and lateral border thickening and callosities with Pirani score being midfoot contracture score-1 and hindfoot contracture score-0 bilaterally (Fig. 1). She had a normal hip and spine examination. On gait examination, weight bearing on the lateral border of the foot with dynamic supination. As the deformities were passively corrected, a trial of 3 serial casting was given with slight improvement on the right side but not so much on the left side (Figs. 2 and 3) hence was planned for TAT transfer.
Under general anesthesia, supine position, and all aseptic precautions, plantar fascia release was performed to correct cavus; dorsomedial incision was taken over TAT, carefully dissected up to the insertion site onto the medial cuneiform, and base of first metatarsal and was found to be bifurcated at a level just distal to extensor retinaculum (Fig. 4).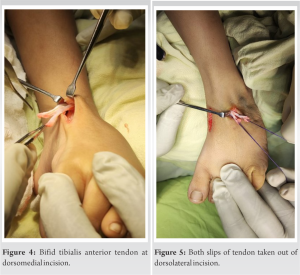
Dorsolateral incision taken over lateral cuneiform under fluoroscopy guidance, both slips of tendon passed subcutaneously out of the dorsolateral incision (Fig. 5) and passed through a transosseous tunnel through lateral cuneiform and anchored at the sole with the use of a button.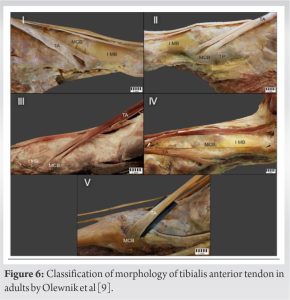
Postoperatively, lower limb immobilized in a long leg cast for 6 weeks. The patient was regularly followed up at our institution with complete recovery and no residual component of dynamic supination in gait at 6-month follow-up.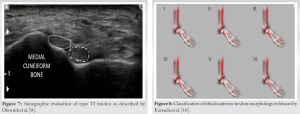
Clubfoot was described in Egyptian hieroglyphs and was described by Hippocrates [1] around 400 BC. He advised treatment with bandages and manipulation “manipulate the foot as if holding a wax model, not by force, but gently.” In 1929, Böhm [2] wrote at the beginning of his article on CTEV: “I feel there is a deficiency in the field of scientific orthopedic surgery relative to the question of the origin of the deformities and their pathological anatomy.” Although the topic CTEV has been extensively researched but still lacks a consensus concerning the etiology, pathogenesis, treatment, and its associated syndromic and non-syndromic associations. Idiopathic CTEV is associated with joint laxity, congenital dislocation of the hip, tibial torsion, ray anomalies of the foot, absences of some tarsal bones, and history of other foot anomalies in the family [3,4]. In CTEV, the ligaments on the medial and posterior sides of the tarsal and ankle joints are extremely thick and stiff, causing the foot to remain in an equinus position with the calcaneus in inversion and the navicular in adduction [5]. The severity of a CTEV malformation is inversely proportional to leg muscle size. In the most severe cases, the gastrosoleus muscle appears as a minute muscle in the proximal portion of the calf. Excess collagen formation in the muscles, tendons, and ligaments can result in relapses up until the age of 3–4 years [6]. Residual dynamic and structural deformities following clubfoot surgery are commonly due to residual muscle imbalance from a strong tibialis anterior muscle (TAM) and weak antagonists. When the child walks, the strong tibialis anterior produces dynamic supination. It can also be a contributing factor in cavus deformities, hindfoot varus and forefoot adduction, and other structural deformities, such as rotatory dorsal subluxation of the navicular following surgical treatment [7]. TAT transfers from base of the first metatarsal to cuboid changes the vector of pull of the muscle and helps to correct the dynamic supination. In this particular case report, we would like to discuss one such muscular anomaly, i.e., bifid TAT. TAM belongs to the anterior compartment of the leg, it arises from the lateral condyle of tibia, and upper two-thirds of lateral surface of tibia. Its distal attachment is on the medial cuneiform and base of the first metatarsal. It plays a role in dorsiflexion and inversion of the foot and is supplied by the deep peroneal nerve [8]. The insertion of TAM is morphologically variable, which has led many authors to develop various classification systems. The most common variant is the occurrence of an additional band but may also have an third band [9]. In a comprehensive review by Zielinska et al., anatomical variants of the TAT insertion describes the classification system of morphological variants of TAM insertion by Olewnik et al. in adults and Karauda et al. in fetuses [10]. Interestingly, Olewnik et al. divided their research into two parts: an anatomical part, which included the anatomical preparation of the TAT in cadavers, and a sonographic part, which included the USG examination in human subjects (Fig. 6). Type I is characterized by two insertions of equal size located on the medial cuneiform and the first metatarsal. Type II is represented by two bands, the wider one inserted on the medial cuneiform and the narrower one on the base of the first metatarsal; this was the most common type in the subjects in the sonographic study. Type III was characterized by the tendinous portion splitting into two ligaments, one inserted at the medial cuneiform (smaller portion) and the other at the base of the first metatarsal (larger portion). As mentioned above, type IV was only observed in the anatomical part of this study; no sonographically examined specimen showed this type. It was characterized by three tendons, one of which attached distally to the medial cuneiform bone, the other two to the base and shaft of the first metatarsal. Type V was characterized by a single ligament attached to the medial cuneiform bone, and this was the most common type among the dissected cadavers. The presence of Type VI was only detected on ultrasound examination; it consisted of two equal-sized ligaments, both attached to the medial cuneiform bone [9] (Fig. 7). The classification system for fetuses proposed by Karauda et al. was based only on the anatomical part of the study of adults (characterized by five types) (Fig. 8). A new type of TAT was identified in fetuses; it has been called type VI. Importantly, it is not the same as type VI (two equal-sized ligaments attaching to the medial cuneiform bone) identified in the sonographic part of the study by Olewnik et al. In the fetuses, type VI was characterized by the tendinous part of the TAM being divided into three distinct ligaments. The distal attachment of the smallest component was at the medial cuneiform bone. The middle and larger components attached to the base of the first metatarsal. This type was found in four lower limbs (two right and two left). It was the basis for the extension of the previous classification. Although the fourth type (three distal attachments, one to the medial cuneiform, and two to the first metatarsal [base and shaft]) was not found in this group, it was not removed from the classification. One possible reason for its absence could be that the group of fetuses was too small; type IV could possibly be found in a larger population of fetuses. However, considering that the characteristic feature of type IV is its three distal appendages, it is possible that the thinnest tendon has not yet developed in fetuses. Other morphological variations of the TAT in fetuses were similar to those in human adults. For example, type I was characterized by a tendon component divided into two ligaments attached to the medial cuneiform bone and the base of the first metatarsal; and type II had the larger component attached to the medial cuneiform bone and the smaller component attached to the base of the first metatarsal. A similar morphological variation is also associated with type III, which is characterized by a tendon component divided into two distal attachments located at the medial cuneiform bone (smaller component) and at the base of the metatarsal bone (larger component). The final example of a close resemblance between fetuses and adults is type V, which had a single ligament attached to the medial cuneiform bone [7]. In our case, we found the tendon split into two equal parts being attached to the medial cuneiform and base of 1st metatarsal which is equivalent to type I, according to the classification proposed by Olewnik et al. Hence, it is important to consider the possibility of a bifid TAT when undergoing a tendon transfer for dynamic supination. It might be feasible to perform an ultrasonographic evaluation preoperatively to have a better understanding before performing the procedure to avoid under correction of the deformity.
Bifid TAT is a rare presentation in a case of CTEV and needs to be considered a possibility before surgically transferring it to correct dynamic supination. It should be aided with a pre-operative sonographic evaluation of the morphology of the TAT.
- Bifid TAT is a rare but real possibility in a case of CTEV
- Careful dissection should be performed during TAT transfer to ensure entire tendon being removed from its insertion to avoid under correction of the deformity
- Preoperative sonographic evaluation might be feasible to diagnose such a condition.
References
- 1.Sarangi PK, Kumar ES, Mohant y J. Calcaneal osteosarcoma: An unusual cause of chronic pediatric heel pain. Oncol J India 2017;1:31. [Google Scholar | PubMed]
- 2.Böhm M. The embryologic origin of club-foot: The krüppelfürsorgestelle of the City of Berlin in St. Hildegard’s Hospital. J Bone Joint Surg 1929;11:229-59 [Google Scholar | PubMed]
- 3.Wynne-Davies R. Genetic and environmental factors in the etiology of talipes equinovarus. Clin Orthop Relat Res 1972;84:9-13. [Google Scholar | PubMed]
- 4.Ippolito E, Gorgolini G. Clubfoot pathology in fetus and pathogenesis. A new pathogenetic theory based on pathology, imaging findings and biomechanics-a narrative review. Ann Transl Med 2021;9:1095. [Google Scholar | PubMed]
- 5.Kadhum M, Lee MH, Czernuszka J, Lavy C. An analysis of the mechanical properties of the Ponseti method in clubfoot treatment. Appl Bionics Biomech 2019;2019:4308462. [Google Scholar | PubMed]
- 6.Thompson GH, Hoyen HA, Barthel T. Tibialis anterior tendon transfer after clubfoot surgery. Clin Orthop Relat Res 2009;467:1306-13. [Google Scholar | PubMed]
- 7.Moore KL, Dalley AF, Agur AM. Clinically Oriented Anatomy. United States: Lippincott Williams & Wilkins; 2013. [Google Scholar | PubMed]
- 8.Holt JB, Westerlind B, Morcuende JA. Tibialis anterior tendon transfer for relapsing idiopathic clubfoot. JBJS essential surgical techniques. 2015;5(3).e16. [Google Scholar | PubMed]
- 9.Karauda P, Podgórski M, Paulsen F, Polguj M, Olewnik Ł. Anatomical variations of the tibialis anterior tendon. Clin Anat 2021;34:397-404 [Google Scholar | PubMed]
- 10.Zielinska N, Tubbs RS, Paulsen F, Szewczyk B, Podgórski M, Borowski A, et al. Anatomical variations of the tibialis anterior tendon insertion: An updated and comprehensive review. J Clin Med 2021;10:3684. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study
June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method
March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method January 1, 2026 Management of Relapsed, Residual, and Resistant Idiopathic Congenital Talipes Equinovarus
January 1, 2026 Management of Relapsed, Residual, and Resistant Idiopathic Congenital Talipes Equinovarus November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet
November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet