
Excision of osteochondroma of hip improves the functional ability. Halts the malignant transformation and improves life expectancy of the patient.
Dr. Damagatla Sreekanth, Department of Orthopaedics, Viswabharathi Medical College, Kurnool, Andhra Pradesh, India. E-mail: kuttisreekanth@gmail.com
Abstract
Introduction: Osteochondroma is the most common primary benign tumor and developmental osseous anomaly resulting in exophytic overgrowth on the surface of bone lined by hyaline cartilage cap. In morphological view, they are sessile or pedunculated forms most commonly occurring in hip, scapula, humerus, and rarely, clavicle. X-ray, MRI, angiogram are useful to know the bony, vascular pathology and histopathological investigation is the gold standard investigation to confirm the diagnosis.
Case Report: A 30-year-old male patient presented to our department with pain and swelling over the right gluteal region followed by difficulty in walking in the past 3 months. On clinical and radiological examination, we observed the findings suggestive of osteochondroma, the patient was planned for excisional biopsy, and the material sent to histopathological examination which confirmed as osteochondroma.
Conclusion: Early diagnosis and excision of tumor prevent functional disability and malignant transformation and improve the life expectancy.
Keywords: Osteochondroma, sessile, pedunculated histopathological examination, malignant transformation.
Osteochondroma is considered as developmental lesion rather than true neoplasm and constitutes 36% to 41% of all tumors, may occur on any bone performed in cartilage but is usually found in metaphysis of long bone near physis. It is a cartilage-covered osseous projection that protrudes from the surface of the bone. Most patients with this disorder have mutation in one of two genes EXT1 and EXT2. Most characteristic feature of lesion is cortical and cancellous components continuously with parental bone [1].
A 30-year-old male patient was admitted in our hospital with pain and swelling over the right gluteal region followed by difficulty in walking, inability to sit on hard surface. The main complaints started 3 months back with swelling insidious in onset, gradually progressive followed by pain. There is no history of fall, trauma, weight loss, and appetite present. On local examination, a diffuse swelling with irregular margins, hard in consistency present on the right gluteal region extending into posteromedial aspect of proximal thigh (Fig. 1).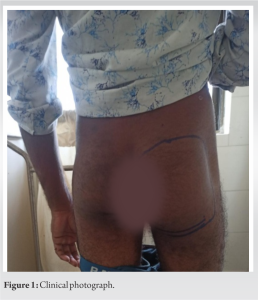 No regional lymphadenopathy. There are no distal neurovascular deficits present. X-ray of pelvis including both hip joints showing cauliflower growth communicating from lesser trochanter of the right femur with corticomedullary continuity has been noticed (Fig. 2).
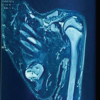
No regional lymphadenopathy. There are no distal neurovascular deficits present. X-ray of pelvis including both hip joints showing cauliflower growth communicating from lesser trochanter of the right femur with corticomedullary continuity has been noticed (Fig. 2).  Further, magnetic resonance imaging (MRI) showed hypointense areas in the lesion raised concern for the presence of necrotic tissue. It shows a low signal on T1, in homogenous high signal on T2 with a peripheral hypointense rim, and edematous infiltration of bone marrow (Fig. 3).
Further, magnetic resonance imaging (MRI) showed hypointense areas in the lesion raised concern for the presence of necrotic tissue. It shows a low signal on T1, in homogenous high signal on T2 with a peripheral hypointense rim, and edematous infiltration of bone marrow (Fig. 3). 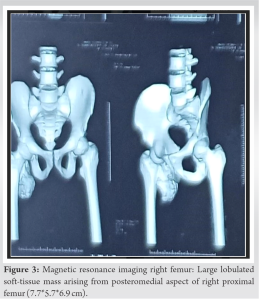 Preliminary blood investigations were done and planned for excisional biopsy through posterior approach (Fig. 4).
Preliminary blood investigations were done and planned for excisional biopsy through posterior approach (Fig. 4).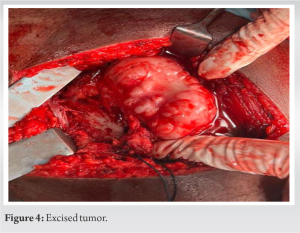 Histopathology tissue has zoned architecture, the superficial part is constructed of well-differentiated chondrocyte, and the cartilaginous depth of tissue is replaced by regular osteoblasts suggestive of osteochondroma. The occurrence of osteochondroma in hip lesion is very rare. Post-operative was uneventful. In postoperative X-ray, complete removal of the lesion was confirmed and patient was mobilized after surgery (Fig. 4). The patient regained near-normal life with no disability and has been in followup without recurrence till date.
Histopathology tissue has zoned architecture, the superficial part is constructed of well-differentiated chondrocyte, and the cartilaginous depth of tissue is replaced by regular osteoblasts suggestive of osteochondroma. The occurrence of osteochondroma in hip lesion is very rare. Post-operative was uneventful. In postoperative X-ray, complete removal of the lesion was confirmed and patient was mobilized after surgery (Fig. 4). The patient regained near-normal life with no disability and has been in followup without recurrence till date.
According to the World Health Organization classification, osteochondroma is defined as cartilage-capped bony projection extending from metaphysis diagnosed as solitary lesion as a part of hereditary multiple osteochondromas involving the hip in 30–90% of patients [1,2]. Sessile and pedunculated are usually symptomless. Cartilage-capped lesions have variable thickness ranging from 0.2 to 1.5 cm traditionally used as a marker for malignant transformation and cutoff of 1 cm to 1.5 cm for excision of osteochondromas for concern of malignant transformation [3]. The continuity of the cortex and medulla of the lesion with that of native bone is path gnomic feature [4]. MRI is useful to know the amount of lesion, soft-tissue involvement, and depth of cartilaginous cap [5]. Histologically, malignant chondrosarcomas are differentiated by hypercellularity, plump nuclei, permeative pattern, and entrapment of bony trabeculae [6]. Complications include nerve, vascular involvement, aneurysmal formation and secondary osteoarthritis, functional disability, and malignant transformation [7]. Biopsy is the gold standard investigation for confirmation of diagnosis and treatment of osteochondromas should be aimed to remove growth, thereby relieving mechanical block [8]. Treatment should consist of the complete lesion removal including cartilage and perichondrium covering it [9]. Inadequacy of removal can lead to recurrence of lesion [10].
Osteochondroma appears in the first and third decades of life, with equal predilection to both males and females with presentation of complaints such as pain and restriction of motion causing disability. Radiological investigations are of more importance and biopsy is the gold standard investigation for the conformation of diagnosis. For patients with painful swelling and restricted joint movement with or without neurovascular deficit, extra periosteal bony excision remains the mainstay of the treatment to prevent malignant transformation.
Early diagnosis and excision of osteochondroma can prevent neurovascular complications, malignant transformation, metastasis and functional disability.
References
- 1.Canella P, Gardin F, Borriani S. Exostosis: Development, evolution and relationship to malignant degeneration. Ital J Orthop Traumatol 1981;7:293-8. [Google Scholar | PubMed]
- 2.Porter DE, Benson MK, Hosney GA. The hip in hereditary multiple exostoses. J Bone Joint Surg Br 2001;83:988-95. [Google Scholar | PubMed]
- 3.Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar | PubMed]
- 4.Haaga JR, Dogra VS, Frosting M, Gilkeson RC, Sundaram M. A case report of osteochondroma with unusual clinical and imaging presentation. Adv Biomed Res 2009;2:2134-5. [Google Scholar | PubMed]
- 5.Douis H, Saifuddin A. The imaging of cartilaginous bone tumours. I. Benign lesions. Skeletal Radiol 2012;41:1195-212. [Google Scholar | PubMed]
- 6.Paik NJ, Han TR, Lim SJ. Multiple peripheral nerve compressions related to malignantly transformed hereditary multiple exostoses. Muscle Nerve 2000;23:1290-4. [Google Scholar | PubMed]
- 7.Feeley BT, Kelly BT. Arthroscopic management of an intraarticular osteochondroma of the hip. Orthop Rev (Pavia) 2009;1:e2. [Google Scholar | PubMed]
- 8.Mehta M, White LM, Knapp T, Kandel RA, Wunder JS, Bell RS. MR imaging of symptomatic osteochondromas with pathological correlation. Skeletal Radiol 1998;27:427-33. [Google Scholar | PubMed]
- 9.Singh R, Jain M, Siwach R, Rohilla S, Sen R, Kaur K. Large para-articular osteochondroma of the knee joint: A case report. Acta Orthop Traumatol Turc 2012;46:139-43. [Google Scholar | PubMed]
- 10.Al Qarni AD. Femoral neck osteochondroma in an athlete: A case report and literature review. Saudi J Sports 2014;14:158-60. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor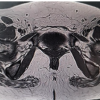 July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report
July 1, 2026 Posterior Femoral Neck Exostosis in a Young Adult: Open Resection and Prophylactic Dynamic Hip Screw Fixation – A Case Report