
Nodular fasciitis should be kept as a differential diagnosis for locally aggressive non-cystic soft-tissue lesions.
Dr. Ashootosh Batra, Department of Orthopedic Surgery, Medeor Hospital, Abu Dhabi, UAE. E-mail: medeorhospi@gmail.com
Abstract
Introduction: Nodular fasciitis is a benign, reactive fibroblastic tumor that usually presents as a rapidly growing lesion with occasional involvement of the deep fascia and muscle. We present a case of nodular fasciitis over the dorsum of the wrist. In our knowledge, this is the first reported case of nodular fasciitis at this location in the literature.
Case Report: A 33-year-old South Asian male with a desk job, presented with a rapidly growing lesion over the dorsum of the left wrist over 5 months, associated with pain and restriction of dorsiflexion of wrist. The X-ray, ultrasound, and magnetic resonance imaging images were inconclusive and excisional biopsy was done for definitive diagnosis.
Conclusion: Nodular fasciitis is a relatively uncommon but important differential diagnosis for any rapid soft-tissue growth. It is a self-limiting proliferative fibroblastic lesion, with excisional biopsy as the gold standard for diagnosis of this condition.
Keywords: Nodular fasciitis, dorsum of wrist, excisional biopsy.
Nodular fasciitis, described for the first time by Kon waler et al. [1], often presents as a rapidly growing mass, with high cellularity and mitotic activity that can be both clinically and histologically misdiagnosed as a soft- tissue sarcoma. It is a proliferative fibroblastic lesion, like fibromatosis [2], and has relatively rare occurrence. It usually develops in the subcutaneous fascia of the extremities and trunk and sometimes in the superficial portions of the deep fascia of the underlying muscle sheath. This case report describes the clinical presentation, diagnostic work up, surgical intervention, and post-operative course of a rare case of nodular fasciitis over the dorsum of the wrist. In our knowledge, this is the first documented case report of this lesion over the dorsum of the wrist.
History and presentation
A 33-year-old male, an electrical engineer with a desk job by profession, presented with a history of the left wrist pain with stiffness and restriction of movements for the past 5 months. The pain was persistent with no associated par esthesia or weakness. There was no antecedent history of injury or trauma. The pain was associated with a swelling in the dorsum of the wrist which had progressively increased over time. Overlying skin was normal. On physical examination, the mass was well- defined, firm, and approximately 2.5 cm (about 0.98 in) in diameter over the dorsum of the wrist with no attachment to skin, but firmly anchored to the dorsum of the wrist and immobile. The dorsiflexion of the wrist was restricted to 10° due to the mass effect. However, no apparent tendon adhesion was noted with full extension over the digits at the inter-phalangeal and metacarpophalangeal joints.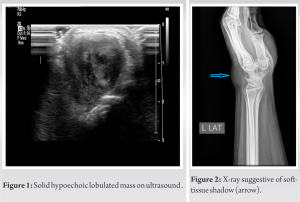
Diagnostic workup
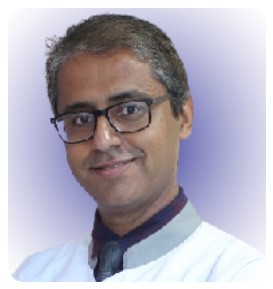
The initial ultrasound (USG) examination (Fig. 1) revealed a solid hypoechoic lobulated mass lesion measuring 27 × 16 mm seen at the dorsal aspect of the left wrist. Differential diagnosis of giant cell tumo r and soft- tissue sarcoma was placed, and further, investigations were advised. X-ray of the wrist was suggestive of soft-tissue shadow in the lateral view (Fig. 2) of wrist with no bony abnormality noted. Magnetic resonance imaging (MRI) scan (Fig. 3 and 4) revealed an irregular intensely enhancing soft- tissue mass at the dorsal aspect of the wrist, interposed between the 4th and the 5th extensor tendon compartments, at the level of the carpal bones. The margins of the mass were well-defined with no evidence of any invasion or encasement of the adjoining vessels or tendons. MRI findings were consistent with a benign soft- tissue neoplasm. To obtain a definitive diagnosis, the patient was scheduled for an excisional biopsy.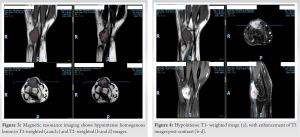
Surgical intervention
The excisional biopsy was done under general an esthesia, 4 cm curvilinear incision was made over the dorsum of wrist, centered over the lesion. Sharp and blunt dissection was done to expose a 3 cm × 3 cm (about 1.18 in) non-cystic hard soft-tissue mass (Fig. 4), found attached to the dorsal joint capsule (Fig. 5). The lesion was well circumscribed, and complete excision of the encapsulated lesion was done. The adjacent tendons and vessels were taken care of to avoid any damage. The surgery was uneventful with patient being discharged the same day.
Histopathology findings
The following immunohistochemistry markers were performed:
- Smooth Muscle Actin: Patchy strong staining in lesional spindle cells
- Calponin: Patchy moderately strong staining in lesional spindle cells
- Desmin: Negative in lesional spindle cells ( 6).
- CD 34: Negative in lesional spindle cells ( 7).
- S100: Negative in lesional spindle cells
- Ki 67: Stains < 1% of the lesional spindle cells.
Sections studied showed well- circumscribed neoplasm composed of interlacing and intersecting fascicles of bland smooth muscle cells (Fig. 8 and 9). Few thick-walled blood vessels could be seen ( Fig. 10). Mitoses were absent. No evidence of atypia / malignancy in the sections studied.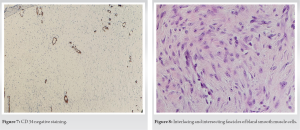
Outcome
The patient had an uneventful post- operative recovery. He came for a follow-up visit in 2 weeks for suture removal and physical therapy was started. He reported complete recovery of range of motion and wrist function without any complications. There was no recurrence till 1 year of follow-up.
Nodular fasciitis is a rare benign reactive lesion presenting as a rapidly growing mass predominantly in young adults between 20 and 40 years of age but with no racial or gender predilection. In about 10 –50% of patients, there is associated pain or tenderness [3,4]. It is usually subcutaneous, although occasional cases involving muscle and fascia have been reported. Nodular fasciitis is commonly found in the volar aspect of the forearm, followed by chest wall and back, and rarely in head and neck [3,5]. There are limited case reports of nodular fasciitis in the hand and wrist, with none of them over the dorsum of wrist [3,5,6]. The macroscopic appearance of nodular fasciitis is characterized by well-circumscribed single mass, and usually measuring <2 cm in diameter; only 8% are larger than 4 cm [3]. Rapid growth of lesion often makes biopsy essential to rule out sarcoma. It is not a true neoplasm and is occasionally associated with history of trauma [3]. The etiology of nodular fasciitis remains unclear. Hara et al. enumerated a list of 13 published case reports of nodular fasciitis in hand and five out of these 13 cases (38.5%) had history of trauma. They summarized that nodular fasciitis of the hand seems to have a close association with trauma compared to occurrence of nodular fasciitis at other locations [7]. The features of nodular fasciitis on USG and MR I are non-specific. The lesions appear as well circumscribed, round to oval masses [8]. Literature descriptions of the signal intensity of the condition, including the contrast enhancement pattern, are variable [8-12]. On MRI, intramuscular lesions appear mildly inhomogeneous and hyper intense to skeletal muscle on T1-weighted spin-echo images; whereas on T2-weighted spin-echo images, the lesions are relatively homogeneous with hyper intense signal to subcutaneous fat. Subcutaneous lesions, typically more fibrous than intramuscular lesions, are markedly hypo intense to skeletal muscle on all spin-echo sequences and appear homogeneous in texture [11-13]. High cellularity and micro vessel density may directly influence the early enhancement after intravenous gadolinium injection and compact cellularity with a prominent capillary network. A myxoid pattern may be responsible for the enhancement on MRI [13]. In our case, intense enhancement of the mass was seen on post- contrast scans. Histopathology of the lesion is suggestive of regular spindle-shaped fibroblasts or myofibroblasts lacking nuclear hyper chromatic and pleomorphism with high cellularity. Although mitotic figures are common, atypical mitoses are almost never seen. Spindle-shaped fibroblasts, clefts separating the fibroblasts, extravasated erythrocytes, interstitial mucoid material, and a loosely textured “ feathery” pattern of the mucopolysaccharide ground substance are diagnostic of nodular fasciitis on histopathology [4]. Immunostains of desmin, cytokeratin, and S-100 are typically negative. In view of inconclusiveness of imaging for diagnosis, biopsy is often the gold standard of diagnosis. Plaza et al. reported that nodular fasciitis remained a difficult diagnosis by fine-needle aspiration biopsy , particularly when it occurred in locations such as the hand [14]. We recommend excisional biopsy where possible, as a diagnostic and therapeutic modality for this condition. Most lesions are effectively treated by local excision, as reflected by a recurrence rate of 1 –2% [3,5,15,16].
Nodular fasciitis of dorsum of wrist has not been documented in the literature and is evidently very rare. Our case emphasized the significance of keeping it as a differential diagnosis for non-cystic well circumscribed soft-tissue mass, especially as clinical and radiological findings, including MRI with contrast, were inconclusive. The prognosis of this condition in the wrist is excellent with very low risk of recurrence. Differential diagnosis of nodular fasciitis will also avoid anxiety and overtreatment associated with fear of malignancy.
Nodular fasciitis should be kept as differential diagnosis for a soft- tissue non- cystic mass even at unexpected clinical locations, with a good prognosis for treatment.
References
- 1.Konwaler BE, Keasbey L, Kaplan L. Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol 1955;25:241-52. [Google Scholar | PubMed]
- 2.Yamane H, Tanaka Y, Shimono M, Yamamura T, Takano N, Saito C, et al. Nodular fascitis of the mandible in a child. Int J Oral Maxillofac Surg 1986;15:499-502. [Google Scholar | PubMed]
- 3.Bernstein KE, Lattes R. Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: Clinicopathologic study of 134 cases. Cancer 1982;49:1668-78. [Google Scholar | PubMed]
- 4.Rankin G, Kuschner SH, Gellman H. Nodular fasciitis: A rapidly growing tumor of the hand. J Hand Surg Am 1991;16:791-5. [Google Scholar | PubMed]
- 5.Shimizu S, Hashimoto H, Enjoji M. Nodular fasciitis: An analysis of 250 patients. Pathology 1984;16:161-6. [Google Scholar | PubMed]
- 6.Kijima H, Okada K, Ito H, Shimada Y, Nanjo H, Itoi E. Nodular fasciitis of the finger. Skeletal Radiol 2005;34:121-3. [Google Scholar | PubMed]
- 7.Hara H, Fujita I, Fujimoto T, Hanioka K, Akisue T, Kurosaka M. Nodular fasciitis of the hand in a young athlete. A case report. Ups J Med Sci 2010;115:291-6. [Google Scholar | PubMed]
- 8.Katz MA, Beredjiklian PK, Wirganowicz PZ. Nodular fasciitis of the hand: A case report. Clin Orthop Relat Res 2001;382:108-11. [Google Scholar | PubMed]
- 9.Frei S, de Lange EE, Fechner RE. Case report 690. Nodular fasciitis of the elbow. Skeletal Radiol 1991;20:468-71. [Google Scholar | PubMed]
- 10.Hymas DC, Mamalis N, Pratt DV, Scott MH, Anderson RL, Langer PD. Nodular fasciitis of the lower eyelid in a pediatric patient. Ophthalmic Plast Reconstr Surg 1999;15:139-42. [Google Scholar | PubMed]
- 11.Leung LY, Shu SJ, Chan AC, Chan MK, Chan CH. Nodular fasciitis: MRI appearance and literature review. Skeletal Radiol 2002;31:9-13. [Google Scholar | PubMed]
- 12.Meyer CA, Kransdorf MJ, Jelinek JS, Moser RP Jr. MR and CT appearance of nodular fasciitis. J Comput Assist Tomogr 1991;15:276-9. [Google Scholar | PubMed]
- 13.Wang XL, De Schepper AM, Vanhoenacker F, De Raeve H, Gielen J, Aparisi F, et al. Nodular fasciitis: Correlation of MRI findings and histopathology. Skeletal Radiol 2002;31:155-61. [Google Scholar | PubMed]
- 14.Plaza JA, Mayerson J, Wakely PE Jr. Nodular fasciitis of the hand: A potential diagnostic pitfall in fine-needle aspiration cytopathology. Am J Clin Pathol 2005;123:388-93. [Google Scholar | PubMed]
- 15.Evans HL, Bridge JA. Nodular fasciitis. In: Fletcher CD, Unni KK, Mertens F, editors. Pathology and Genetics Tumours of Soft Tissue and Bone. Lyon: IARC; 2002. p. 48-9. [Google Scholar | PubMed]
- 16.Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. 5th ed. St. Louis: Mosby: 2007. p. 177-89. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 A Case Report of a Rare Entity – Lateral End of Clavicle Chondromyxoid Fibroma which was Mistaken as Giant Cell Tumor and Aneurysmal Cyst
August 1, 2025 A Case Report of a Rare Entity – Lateral End of Clavicle Chondromyxoid Fibroma which was Mistaken as Giant Cell Tumor and Aneurysmal Cyst January 1, 2025 Giant Cell Tumor of Distal Radius Treated with Wide Local Excision and Reconstruction with Ipsilateral Proximal Fibular Autograft – A Follow-Up
January 1, 2025 Giant Cell Tumor of Distal Radius Treated with Wide Local Excision and Reconstruction with Ipsilateral Proximal Fibular Autograft – A Follow-Up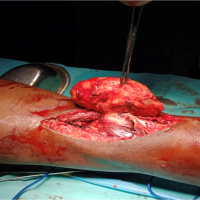 August 10, 2023 Dilemmas in Diagnosing Popliteal Swellings: Nodular Fasciitis Masquerading as Baker’s Cyst
August 10, 2023 Dilemmas in Diagnosing Popliteal Swellings: Nodular Fasciitis Masquerading as Baker’s Cyst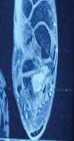 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report