
The posterior capsule of the knee plays an important role in maintaining the integrity of the knee joint, and arthroscopic capsulotomy is proposed as a safer, minimally invasive option that has been gaining recent favor compared to open approaches.
Dr. Andrea Montalbano, Department of Orthopedic Surgery, University of Toledo, 3000 Arlington Drive, Toledo, OH 43614, United States. E-mail: andrea.montalbano@utoledo.edu
Abstract
Introduction: The posterior capsule of the knee plays an important role in maintaining the integrity of the knee joint. Pathologies involving the posterior capsule have been implicated in developing flexion contractures. Posterior capsulotomy is a well-studied modality for this issue, performed through either an open or arthroscopic approach.
Case Report: A 74-year-old Caucasian male presented with a complex extensor lag of his right knee and an inability to gain full extension either actively or passively. Through the use of standard knee arthroscopy, the authors were able to not only correct his posterior capsular pathology but also address anterior knee lesions. Only the combination of both allowed a full extension of the joint.
Conclusion: Posterior capsulotomy of the knee may be carried out successfully and safely through either an open or arthroscopic approach. Arthroscopic capsulotomy is proposed as a safer, minimally invasive option that has been gaining recent favor compared to open approaches.
Keywords: Posterior capsulotomy, arthroscopy, extensor lag, knee.
The posterior capsule of the human knee is a synovial structure that plays an important role in maintaining the integrity of the knee joint [1]. The structure is formed by the confluence of several tendons on the posterior aspect of the knee and spans from the posteromedial and posterolateral aspects of the femoral condyles inferiorly to the posterior aspect of the tibia [2,3]. Pathologies involving the posterior capsule have been implicated in the development of flexion contractures. These contractures occur most commonly due to immobility and have been implicated in prolonged healing times and morbidity [4]. Following arthroscopic and open procedures of the knee, it is common to develop a persistent knee contracture. Wierer et al. demonstrated that the median postoperative extension deficit was 15° [5]. These contractures can be difficult to treat with conservative management alone, as the problem is caused by cellular change. Animal models have suggested prolonged immobility leads to increased intimal adhesions in the tissue of the posterior capsule. Synovial proliferation is also decreased in the immobile state [4]. These changes decrease the ability of the capsular tissue to meet the demands of rehabilitation in the postoperative state. Surgical management of flexion contractures of the knee is necessary when conservative treatment modalities fail. The purpose of this review is to investigate surgical techniques of both open and arthroscopic posterior capsular releases. In addition, we will share a novel technique performed at our institution that has not previously been described to the best of our knowledge.
A 74-year-old male presented with a significant extensor lag of his right knee and an inability to gain full extension either actively or passively. Subsequent magnetic resonance imaging revealed a medial meniscus tear and the presence of an anterior loose body (Fig. 1).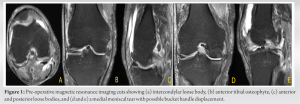 A shared decision was made to proceed with arthroscopic surgical intervention. Arthroscopy of the knee was performed using standard portals. After removing the previously visualized anterior loose body, an osteoplasty of an anterior tibial osteophyte was performed. At this point, the patient was still unable to achieve full extension of the knee. It was then decided to perform a posterior capsular release. Beginning with the posteromedial compartment, inflammation and thickening of the posterior capsule were directly visualized. The posteromedial capsule was then released using a standard arthroscopic electrocautery tool. The posterolateral compartment was subsequently visualized, which also demonstrated inflammation and thickening. It was also released in a likewise fashion. At this time, we were still unsatisfied with the degree of knee extension on manipulation and revisited the anterior aspect of the joint. Further synovectomy and debridement were carried out, addressing remnant intra-articular adhesions surrounding the patella. After releasing the posterior capsule both medially and laterally, in combination with the thorough release of anterior adhesions, full extension was achieved with manual pressure and manipulation (Fig. 2).
A shared decision was made to proceed with arthroscopic surgical intervention. Arthroscopy of the knee was performed using standard portals. After removing the previously visualized anterior loose body, an osteoplasty of an anterior tibial osteophyte was performed. At this point, the patient was still unable to achieve full extension of the knee. It was then decided to perform a posterior capsular release. Beginning with the posteromedial compartment, inflammation and thickening of the posterior capsule were directly visualized. The posteromedial capsule was then released using a standard arthroscopic electrocautery tool. The posterolateral compartment was subsequently visualized, which also demonstrated inflammation and thickening. It was also released in a likewise fashion. At this time, we were still unsatisfied with the degree of knee extension on manipulation and revisited the anterior aspect of the joint. Further synovectomy and debridement were carried out, addressing remnant intra-articular adhesions surrounding the patella. After releasing the posterior capsule both medially and laterally, in combination with the thorough release of anterior adhesions, full extension was achieved with manual pressure and manipulation (Fig. 2). 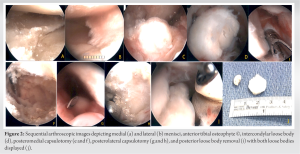 Postoperatively, the patient was placed in a hinged knee brace locked in extension. He was seen at 2 and 8 weeks for follow-up. The patient was subsequently lost to follow-up. However, he had regained full motion, ambulated without a limp, and was pain-free at 8-week post-operative. The authors believe this case demonstrates the viable use of posterior capsulotomy of the knee using an arthroscopic approach to regain complete knee extension. Furthermore, it also suggests the importance of concomitantly addressing anterior blocks to extension in addition to the capsule itself. For this patient, posterior capsular release alone did not provide full motion, and only with thorough release of anterior adhesions was he able to reach maximal extension. This may represent a crucial advantage of arthroscopic versus open capsulotomy, as the latter would not have readily available access to the anterior knee.
Postoperatively, the patient was placed in a hinged knee brace locked in extension. He was seen at 2 and 8 weeks for follow-up. The patient was subsequently lost to follow-up. However, he had regained full motion, ambulated without a limp, and was pain-free at 8-week post-operative. The authors believe this case demonstrates the viable use of posterior capsulotomy of the knee using an arthroscopic approach to regain complete knee extension. Furthermore, it also suggests the importance of concomitantly addressing anterior blocks to extension in addition to the capsule itself. For this patient, posterior capsular release alone did not provide full motion, and only with thorough release of anterior adhesions was he able to reach maximal extension. This may represent a crucial advantage of arthroscopic versus open capsulotomy, as the latter would not have readily available access to the anterior knee.
Open procedures of the knee were the standard of care for operative knee joint pathologies until arthroscopic techniques and technology drastically improved. This included surgical management for posterior capsular release. The open technique has been implemented with success, especially in patients with prolonged contracture for >1 year. Lobenhoffer et al. showed that using an open technique, extension was increased from an average of 17° of deficit preoperatively to 2° after 18 months [6]. Vahedi et al. examined flexion contractures after total knee arthroplasty (TKA) in 21 patients with post-operative contractures [7]. Their surgical technique included posterior capsule and hamstring tendon release, peroneal nerve decompression, and botulinum toxin injection into the gastrocnemius and hamstrings. The reported increase in extension in this cohort of patients increased from a 27° deficit to full extension by 31 months. Open capsular release has also been demonstrated to be a safe procedure regarding the neurovascular structures of the posterior knee. Pinter et al. studied the role of posterior capsular release as an adjunct for patients undergoing TKA with concomitant flexion contracture [8]. Cadaveric knees underwent open posterior capsular release using anterior incisions, mimicking the approach for TKA. A curved osteotome was used to complete the posterior capsular release. In the midline, the osteotome was able to be inserted an average of 13.6 cm. The popliteal fossa was dissected to search for evidence of a neurovascular injury. None of the cadaveric specimens demonstrated damage to the tibial nerve, popliteal artery, or popliteal vein. It has been generally accepted that the necessary distance required to complete a posterior capsule release during TKA is around 5–10 cm. This study demonstrated larger penetrating distances in the midline and no damage to the popliteal fossa, suggesting a surgeon can safely complete a posterior capsule release with an osteotome during TKA to treat pre-operative flexion contracture. The arthroscopic technique has also been studied at length. LaPrade et al. demonstrated that posterior capsule release can be successfully completed during routine knee arthroscopy [9]. Their technique consisted of using standard anterior portals to completely visualize the posterior aspect of the knee. The posteromedial capsule was released using a blunt obturator. The remainder of the capsule was released using the shaver blade facing away from the neurovasculature bundle. After capsular release, the knee was then manipulated to full extension. At 24-month follow-up, the average knee motion improved from a 14.7° extension deficit to a near-complete extension (0.7° deficit). Pace and Wahl investigated the distances between standard arthroscopic portals and the important ligamentous and neurovascular structures of the knee using cadaveric specimens [10]. They examined the distance between the popliteal artery and posterior capsule, as well as the posteromedial and posterolateral portals to the saphenous neurovascular bundle and peroneal nerve, respectively. They demonstrated that the average distance between the posterior border of the posterior cruciate ligament (PCL) and the popliteal artery was 19 mm ± 4.3 mm. This was determined to be a safe distance for both posterior capsular release and manipulation of the knee under anesthesia following the release. The average distance between the posteromedial portal and the saphenous vein was 22.7 mm ± 6.7 mm. The posterolateral portal is, on average, 41.3 mm ± 7.94 mm from the peroneal nerve. The authors of this study suggested that these measurements represent a safe distance from the necessary portals needed to completely release the posterior capsule. Further support for the safety of crucial structures in the knee during arthroscopy has been demonstrated by Matava et al., showing the PCL-popliteal artery distance increased with progressive knee flexion in arthroscopic conditions [11]. Although the capsule itself was not used as a marker in the study, this finding is useful when considering optimal patient and positioning during surgery. In addition, Ahn et al. and Ramos et al. have shown space exists between the PCL and the capsule, and the PCL-popliteal artery interval increases with careful release of the capsule [3,12]. Recently, an arthroscopic technique for posterior capsular release has been characterized [13]. Standard anteromedial and anterolateral arthroscopic portals were created. Metzenbaum scissors were inserted to release the posteromedial capsule. After creating an additional portal between the lateral collateral ligament and the lateral head of the gastrocnemius, the Metzenbaum scissors were utilized to release the posterolateral capsule. Finally, the central posterior capsule was released with the Metzenbaum scissors through a trans-septal portal. At this point, the knee was manipulated into full extension. The authors conclude that their technique allows for complete capsulotomy in the medial, lateral, and central compartments of the posterior knee. This review of current literature on both open and arthroscopic techniques and associated outcomes for posterior capsulotomy has demonstrated both methods are efficacious. The arthroscopic method has been demonstrated to be an effective intervention which, when implemented by an experienced surgeon, can achieve fantastic results.
Posterior capsulotomy of the knee may be carried out successfully and safely through either an open or arthroscopic approach. For specific indications, open release has been suggested to offer superior efficacy [6]. Alternatively, arthroscopic capsulotomy is proposed as an even safer, minimally invasive option. It provides additional ability to address all other major areas of the knee without converting to open approaches. This is particularly useful during cases such as ours where release of the posterior capsule does not fully correct passive motion and other pathologies about the joint must be explored and addressed.
The posterior capsule of the knee plays an important role in maintaining the integrity of the knee joint. A 74-year-old Caucasian male presented with a complex extensor lag of his right knee and inability to gain full extension either actively or passively. Through the use of standard knee arthroscopy, the authors were able to not only correct his posterior capsular pathology but also address anterior knee lesions. Only the combination of both allowed a full extension of the joint. Arthroscopic capsulotomy is proposed as a safer, minimally invasive option that has been gaining recent favor compared to open approaches.
References
- 1.Campbell TM, Trudel G, Laneuville O. Knee flexion contractures in patients with osteoarthritis: Clinical features and histologic characterization of the posterior capsule. PM R 2015;7:466-73. [Google Scholar | PubMed]
- 2.LaPrade RF, Morgan PM, Wentorf FA, Johansen S, Engebretsen L. The anatomy of the posterior aspect of the knee. An anatomic study. J Bone Joint Surg Am 2007;89:758-64. [Google Scholar | PubMed]
- 3.Ramos LA, De Carvalho RT, Cohen M, Abdalla RJ. Anatomic relation between the posterior cruciate ligament and the joint capsule. Arthroscopy 2008;24:1367-72. [Google Scholar | PubMed]
- 4.Trudel G, Jabi M, Uhthoff HK. Localized and adaptive synoviocyte proliferation characteristics in rat knee joint contractures secondary to immobility. Arch Phys Med Rehabil 2003;84:1350-6. [Google Scholar | PubMed]
- 5.Wierer G, Runer A, Gföller P, Fink C, Hoser C. Extension deficit after anterior cruciate ligament reconstruction: Is arthroscopic posterior release a safe and effective procedure? Knee 2017;24:49-54. [Google Scholar | PubMed]
- 6.Lobenhoffer HP, Bosch U, Gerich TG. Role of posterior capsulotomy for the treatment of extension deficits of the knee. Knee Surg Sports Traumatol Arthrosc 1996;4:237-41. [Google Scholar | PubMed]
- 7.Vahedi H, Khlopas A, Szymczuk VL, Peterson MK, Hammouda AI, Conway JD. Treatment with posterior capsular release, botulinum toxin injection, hamstring tenotomy, and peroneal nerve decompression improves flexion contracture after total knee arthroplasty: Minimum 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 2020;28:2706-14. [Google Scholar | PubMed]
- 8.Pinter Z, Staggers R, Lee S, Bergstresser S, Shah A, Naranje S. Open posterior capsular release with an osteotome in total knee arthroplasty does not place important neurovascular structures at risk. Knee Surg Sports Traumatol Arthrosc 2019;27:2120-3. [Google Scholar | PubMed]
- 9.LaPrade RF, Pedtke AC, Roethle ST. Arthroscopic posteromedial capsular release for knee flexion contractures. Knee Surg Sports Traumatol Arthrosc 2008;16:469-75. [Google Scholar | PubMed]
- 10.Pace JL, Wahl CJ. Arthroscopy of the posterior knee compartments: Neurovascular anatomic relationships during arthroscopic transverse capsulotomy. Arthroscopy 2010;26:637-42. [Google Scholar | PubMed]
- 11.Matava MJ, Sethi NS, Totty WG. Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804. [Google Scholar | PubMed]
- 12.Ahn JH, Wang JH, Lee SH, Yoo JC, Jeon WJ. Increasing the distance between the posterior cruciate ligament and the popliteal neurovascular bundle by a limited posterior capsular release during arthroscopic transtibial posterior cruciate ligament reconstruction: A cadaveric angiographic study. Am J Sports Med 2007;35:787-92. [Google Scholar | PubMed]
- 13.Malinowski K, Góralczyk A, Hermanowicz K, LaPrade RF, Więcek R, Domżalski ME. Arthroscopic complete posterior capsulotomy for knee flexion contracture. Arthrosc Tech 2018;7:e1135-9. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management
August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain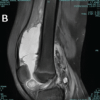 July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study