
To describe the management of bilateral congenital radioulnar synostosis in a 5-year-old female child using a novel minimally invasive, single-staged procedure and a brief overview regarding various osteotomies for the same.
Dr . Deepak Jain, Department of Orthopaedics, MGM Institute of Health Sciences, Navi Mumbai, Maharashtra, India. E-mail: deepaksjain1993@gmail.com
Abstract
Introduction: Congenital radioulnar synostosis is a rare deformity of the forearm characterized by a malformation of the proximal aspect of the radius and ulna. Various modalities of treatment options available include observation, excision of the synostosis and placing an interposition material, or performing derotation osteotomy. Several types of osteotomies at different forearm levels have been described in the literature.
Case Report: A 5-year-old female presented with bilateral congenital radioulnar synostosis which was treated with percutaneous corrective osteotomy and Joshi’s external stabilizing system fixator application.
Conclusion: We describe the management of congenital radioulnar synostosis in a 5-year-old female child using a novel minimally invasive, single-staged procedure. This innovative technique provided the patient with a good functional outcome and she could return to her daily activities with a satisfactory range of motion.
Keywords: Congenital, synostosis, radioulnar, osteotomies.
Congenital radioulnar synostosis is a rare deformity of the forearm characterized by a malformation of the proximal aspect of radius and ulna. It is caused by failure of longitudinal segmentation with persistence of the bony anlage between the proximal radius and ulna [1]. It is more common in boys and 60% of cases have bilateral occurrence. It has a 20% positive family history and autosomal dominant inheritance. It can also be associated with congenital syndromes such as Apert syndrome, Carpenter syndrome, arthrogryposis, mandibulofacial dysostosis, and Klinefelter’s syndrome. It can also be associated with fetal alcohol spectrum disorder which occurs due to the exposure to alcohol during the intrauterine period [2]. Various treatment modalities have been described in the literature including observation [3], excision of the synostosis and placing an interposition material [4], and derotational osteotomies [5] to prevent the deformity from interfering with the daily activities of the child as he/she progresses into adulthood. In this particular case, we will discuss the management of congenital radioulnar synostosis with a novel minimally invasive, single-staged technique.
A 5-year-old female was brought by her parents when they noticed their child having a deformity and limited range of motion of both elbows. They noticed the deformity when the child was 1 year old. There was no history of any associated trauma, or similar complaints in the family. On examination, no other congenital abnormality was detected. Probing her prenatal, intranatal, and postnatal periods was also uneventful. On inspection, the forearms were thin and a well-marked sulcus was seen at the posterolateral aspect of the proximal forearm corresponding to the normal position of the radial head. There was no swelling or undue bony prominence. No cubitus valgus or valgus instability . The range of motion at the shoulder and elbow was completely unrestricted and painless. Both the forearms were fixed in pronation (Fig. 1). The right side was fixed at 70° of pronation with further pronation up to 90°. The left side was fixed at 10° of pronation with further pronation up to 90°. Hypermobility was seen at the wrist joint due to the laxity of the capsular ligaments. The radiological picture was suggestive of Type 2 congenital radioulnar synostosis according to Cleary’s classification (Fig. 2) [6]. After performing all routine investigations and getting fitness for surgery, the patient was planned for derotation osteotomy for the right side.
The range of motion at the shoulder and elbow was completely unrestricted and painless. Both the forearms were fixed in pronation (Fig. 1). The right side was fixed at 70° of pronation with further pronation up to 90°. The left side was fixed at 10° of pronation with further pronation up to 90°. Hypermobility was seen at the wrist joint due to the laxity of the capsular ligaments. The radiological picture was suggestive of Type 2 congenital radioulnar synostosis according to Cleary’s classification (Fig. 2) [6]. After performing all routine investigations and getting fitness for surgery, the patient was planned for derotation osteotomy for the right side.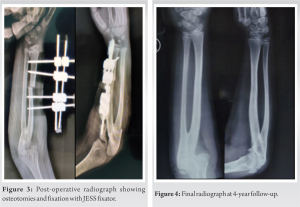 The child was positioned supine on the operating table with the forearm by the side. After appropriate anaesthesia, parts were painted and draped. 2 × 1.2 mm K-wires were passed percutaneously in the shaft of the radius proximal and distal to the desired osteotomy site at an angle of 70°. Then, a 2 cm incision was taken on the dorsolateral aspect of the radius, the soft tissue was dissected, and extensor tendons retracted and protected. The periosteum was incised with number 15 blade, and bone was exposed. The corticotomy was performed with multiple drill holes with 1.5 mm K-wire and was completed using a straight osteotome. After completing the osteotomy, K-wires were made parallel to each other. After getting the K-wires parallel, there was still some resistance to get the desired correction. Hence, we decided to do an ulnar osteotomy. Another 1 cm incision was taken under IITV guidance just distal to the synostosis site, and ulnar osteotomy was performed in a similar fashion as the The K-wires were made parallel to each other and connected to JESS clamps (mini external fixator) and connecting rods after getting the desired correction (Fig. 3). The wound was washed and closed in layers. Postoperatively, the patient was placed in a long-arm slab. The slab was converted to a long-arm cast after suture removal on post-operative day 10. The patient’s right arm was immobilized for a month after which the JESS fixator (mini external
The child was positioned supine on the operating table with the forearm by the side. After appropriate anaesthesia, parts were painted and draped. 2 × 1.2 mm K-wires were passed percutaneously in the shaft of the radius proximal and distal to the desired osteotomy site at an angle of 70°. Then, a 2 cm incision was taken on the dorsolateral aspect of the radius, the soft tissue was dissected, and extensor tendons retracted and protected. The periosteum was incised with number 15 blade, and bone was exposed. The corticotomy was performed with multiple drill holes with 1.5 mm K-wire and was completed using a straight osteotome. After completing the osteotomy, K-wires were made parallel to each other. After getting the K-wires parallel, there was still some resistance to get the desired correction. Hence, we decided to do an ulnar osteotomy. Another 1 cm incision was taken under IITV guidance just distal to the synostosis site, and ulnar osteotomy was performed in a similar fashion as the The K-wires were made parallel to each other and connected to JESS clamps (mini external fixator) and connecting rods after getting the desired correction (Fig. 3). The wound was washed and closed in layers. Postoperatively, the patient was placed in a long-arm slab. The slab was converted to a long-arm cast after suture removal on post-operative day 10. The patient’s right arm was immobilized for a month after which the JESS fixator (mini external
fixator) and cast were removed, and gradual mobilization was started. The patient regained full range of motion at the elbow and wrist at 2-month follow-up. At 4 years old follow-up, the child shows good functional outcome and the radiograph shows complete consolidation of the osteotomy site (Fig. 4 and 5).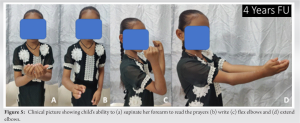
The forearm begins as a single cartilaginous anlage and differentiates into radius and ulna in a caudocephalic direction during the 7th week of the intrauterine life period [6,7]. Failure of this differentiation results in synostosis at the proximal aspect of the forearm. The shoulder joint compensates for complete supination and therefore the deformity can be missed by the child’s parents in the formative years. One of the most widely used classification systems used for congenital radioulnar synostosis is the Cleary classification system. It is based on the radiological appearance of the synostosis and the radial head reduction. In type 1, there is no osseous synostosis, radial head is reduced. In type 2, there is osseous synostosis and the radial head is reduced. In type 3, there is long osseous synostosis with a hypoplastic and posteriorly dislocated radial head. In type 4, there is a short osseous synostosis with a mushroom-shaped and anteriorly dislocated radial head. There are various methods of treating congenital radioulnar synostosis. It can be treated conservatively with observation and regular follow-up but that is generally reserved for asymptomatic and unilateral cases. Operative indications include the deformity limiting the child’s daily activities mainly when the pronation deformity exceeds 60° and when it is bilateral [3]. There are two types of operative treatment. The first being synostosis excision with soft-tissue interposition. The goal of this surgery is to restore active forearm rotation. After excising the synostosis, interposition material is placed between the two bones to prevent recurrence. However, the results of this surgery were unsatisfactory as it led to only a slight gain in the active forearm range of motion. The second and most widely used operative procedure is called the forearm derotational osteotomy as it places the forearm in a more functional resting position and has low recurrence rates. The mean age for performing this procedure is 3–6 years [1]. Osteotomy can be performed at various levels. A comprehensive review of the literature on the various osteotomies has been performed and is shown in Table 1 . The first is proximal to synostosis but this is most often associated with posterior interosseous nerve palsy [8]. Osteotomy just distal to synostosis is preferred as it distributes the rotational correction and decreases the risk of neurovascular complications and compartment syndrome [9]. The deformity can be corrected simultaneously with the osteotomy or after the 10th postoperative day but gradual correction with an external fixator is the most preferred method as studies have demonstrated it to have the lowest rate of neurovascular complications. There is no consensus in the literature on what the final position of the forearm should be [1]. Various surgeons prefer different positions, and the final positioning varies for unilateral and bilateral cases. In unilateral cases, the forearm is fixed in 0–30° of pronation and in bilateral cases, the dominant forearm is fixed at 30° of pronation, and the contralateral one is fixed in a neutral position [1]. Now, the correction can be maintained by cast, K-wire, Titanium Elastic Nail, plate, or external fixator [1,3]. The correction can be stabilized with a cast, but casting has a risk of recurrence with loss of reduction if the cast becomes loose. Furthermore, K-wire and tens may not be able to maintain the rotational alignment which might lead to loss of few degrees of correction. The osteotomy can be fixed with a plate, but such low-profile plates are not easily available. Plating require requires an open procedure and a second surgery for implant removal. Compartment syndrome can occur in up to 36% of the cases, especially when large (>60%) rotational corrections are performed. Therefore, it is of utmost importance to closely monitor the child postoperatively. Nerve palsies are also a common complication [10] of the procedure but most of them are neuropraxia neuropraxias and resolve within 3 months. The unique features of our technique were that both the osteotomies were performed percutaneously. The K-wires helped guide the correction and the same wires were used for fixation into a JESS fixator (mini external fixator).
Failure of this differentiation results in synostosis at the proximal aspect of the forearm. The shoulder joint compensates for complete supination and therefore the deformity can be missed by the child’s parents in the formative years. One of the most widely used classification systems used for congenital radioulnar synostosis is the Cleary classification system. It is based on the radiological appearance of the synostosis and the radial head reduction. In type 1, there is no osseous synostosis, radial head is reduced. In type 2, there is osseous synostosis and the radial head is reduced. In type 3, there is long osseous synostosis with a hypoplastic and posteriorly dislocated radial head. In type 4, there is a short osseous synostosis with a mushroom-shaped and anteriorly dislocated radial head. There are various methods of treating congenital radioulnar synostosis. It can be treated conservatively with observation and regular follow-up but that is generally reserved for asymptomatic and unilateral cases. Operative indications include the deformity limiting the child’s daily activities mainly when the pronation deformity exceeds 60° and when it is bilateral [3]. There are two types of operative treatment. The first being synostosis excision with soft-tissue interposition. The goal of this surgery is to restore active forearm rotation. After excising the synostosis, interposition material is placed between the two bones to prevent recurrence. However, the results of this surgery were unsatisfactory as it led to only a slight gain in the active forearm range of motion. The second and most widely used operative procedure is called the forearm derotational osteotomy as it places the forearm in a more functional resting position and has low recurrence rates. The mean age for performing this procedure is 3–6 years [1]. Osteotomy can be performed at various levels. A comprehensive review of the literature on the various osteotomies has been performed and is shown in Table 1 . The first is proximal to synostosis but this is most often associated with posterior interosseous nerve palsy [8]. Osteotomy just distal to synostosis is preferred as it distributes the rotational correction and decreases the risk of neurovascular complications and compartment syndrome [9]. The deformity can be corrected simultaneously with the osteotomy or after the 10th postoperative day but gradual correction with an external fixator is the most preferred method as studies have demonstrated it to have the lowest rate of neurovascular complications. There is no consensus in the literature on what the final position of the forearm should be [1]. Various surgeons prefer different positions, and the final positioning varies for unilateral and bilateral cases. In unilateral cases, the forearm is fixed in 0–30° of pronation and in bilateral cases, the dominant forearm is fixed at 30° of pronation, and the contralateral one is fixed in a neutral position [1]. Now, the correction can be maintained by cast, K-wire, Titanium Elastic Nail, plate, or external fixator [1,3]. The correction can be stabilized with a cast, but casting has a risk of recurrence with loss of reduction if the cast becomes loose. Furthermore, K-wire and tens may not be able to maintain the rotational alignment which might lead to loss of few degrees of correction. The osteotomy can be fixed with a plate, but such low-profile plates are not easily available. Plating require requires an open procedure and a second surgery for implant removal. Compartment syndrome can occur in up to 36% of the cases, especially when large (>60%) rotational corrections are performed. Therefore, it is of utmost importance to closely monitor the child postoperatively. Nerve palsies are also a common complication [10] of the procedure but most of them are neuropraxia neuropraxias and resolve within 3 months. The unique features of our technique were that both the osteotomies were performed percutaneously. The K-wires helped guide the correction and the same wires were used for fixation into a JESS fixator (mini external fixator).
We describe the management of bilateral congenital radioulnar synostosis in a 5-year-old female child using a novel minimally invasive, single-staged procedure . This innovative technique provided the patient with a good functional outcome and she could return to her daily activities with a satisfactory range of motion.
This article describes a unique case of bilateral congenital radioulnar synostosis which is managed with a new and less invasive operative technique. Various osteotomies used for this deformity have also been overviewed which describes the evolution of operative procedures.
References
- 1.Murase T, Tada K, Yoshida T, Moritomo H. Derotational osteotomy at the shafts of the radius and ulna for congenital radioulnar synostosis. J Hand Surg Am 2003;28:133-7. [Google Scholar | PubMed]
- 2.Hoyme HE, Kalberg WO, Elliott AJ, Blankenship J, Buckley D, Marais AS, et al. Updated clinical guidelines for diagnosing fetal alcohol spectrum disorders. Pediatrics 2016;138:e20154256. [Google Scholar | PubMed]
- 3.Yammine K, Salon A, Pouliquen JC. Congenital radioulnar synostosis. Study of a series of 37 children and adolescents. Chir Main 1998;17:300-8. [Google Scholar | PubMed]
- 4.Wilkie DP. Congenital radio‐ulnar synostosis. Br J Surg 1913;1:366-75. [Google Scholar | PubMed]
- 5.Miura T, Nakamura R, Suzuki M, Kanie J. Congenital radio-ulnar synostosis. J Hand Surg Br 1984;9:153-5. [Google Scholar | PubMed]
- 6.Cleary JE, Omer GE Jr. Congenital proximal radio-ulnar synostosis. Natural history and functional assessment. J Bone Joint Surg Am 1985;67:539-45. [Google Scholar | PubMed]
- 7.Simmons BP, Southmayd WW, Riseborough EJ. Congenital radioulnar synostosis. J Hand Surg Am 1983;8:829-38. [Google Scholar | PubMed]
- 8.Hung NN. Derotational osteotomy of the proximal radius and the distal ulna for congenital radioulnar synostosis. J Child Orthop 2008;2:481-9. [Google Scholar | PubMed]
- 9.Barik S, Farr S, Gallone G, Zarantonello P, Trisolino G, Di Gennaro GL. Results after treatment of congenital radioulnar synostosis: A systematic review and pooled data analysis. J Pediatr Orthop B 2021;30:593-600. [Google Scholar | PubMed]
- 10.Simcock X, Shah AS, Waters PM, Bae DS. Safety and efficacy of derotational osteotomy for congenital radioulnar synostosis. J Pediatr Orthop 2015;35:838-43. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2024 Complete Ankle Joint that is Tibiotalar and Distal Tibiofibular Coalition Presenting with Foot and Ankle Pain – A Case Report
May 10, 2024 Complete Ankle Joint that is Tibiotalar and Distal Tibiofibular Coalition Presenting with Foot and Ankle Pain – A Case Report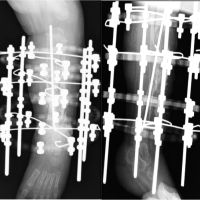 August 10, 2022 Transient Hypertension in a case of Congenital Pseudarthrosis of Tibia treated with Ring Fixator: A Case Report
August 10, 2022 Transient Hypertension in a case of Congenital Pseudarthrosis of Tibia treated with Ring Fixator: A Case Report January 6, 2019 Hoffa’s Fat Pad-associated Solitary Neurofibroma as the Cause of Anterior Knee Pain: A Case Report
January 6, 2019 Hoffa’s Fat Pad-associated Solitary Neurofibroma as the Cause of Anterior Knee Pain: A Case Report March 10, 2018 Solitary Presentation but Multiple Etiologies in Foot: A Case Series
March 10, 2018 Solitary Presentation but Multiple Etiologies in Foot: A Case Series