
Unusual cases may be sometimes simple to treat and for good initial treatment strategy; basic principles have to be followed. Emergent reduction of the dislocated joints is of paramount importance.
Dr. Kuldeep Chand Vatsyan, Department of Orthopaedic Surgery, Shri Lal Bahadur Shastri Government Medical College and Hospital, Mandi, Himachal Pradesh, India. E-mail: kuldeepvatsyan64@gmail.com
Abstract
Introduction: A dislocated knee is a potential limb-threatening injury. Simultaneous dislocation of knee and ankle joint in an ipsilateral limb is a very rare pattern of injury. A few cases of ipsilateral hip and knee dislocation were described in literature. Rare injury such as posterior dislocation knee with ipsilateral ankle fracture dislocation cases was also presented. However, lateral dislocation of knee along with the same side ankle fracture dislocation is a rare scenario. To the best of our knowledge, these two simultaneous lesions do not seem to have been reported previously. Immediate management of such injury is to reduce both joint and stabilization with external fixator and definitive surgery in the second stage when soft-tissue condition allows.
Case Report: We describe a rare case of a 37-year-old farmer having injury to his right leg with tiller machine. Lateral right knee dislocation and right ankle fracture dislocation reduced in the emergency department. In emergency OT, external fixator applied for knee and ankle stabilization. When swelling subsides in ankle, fracture fixation is done with plates and screws. Knee fixator is kept for 6 weeks then knee physiotherapy started.
Conclusion: Dislocation of any joint is treated as an orthopedic emergency. Simultaneous dislocation of knee and ankle joints in an ipsilateral limb is a challenging situation for even the experienced surgeon. The outcome of such patients varies with associated injuries and time took for relocation and meticulous physical examination, with a high index of clinical suspicion is needed in diagnosing and management of such cases.
Keywords: Ipsilateral, dislocation, external fixator.
A dislocated knee is a potential limb-threatening injury. Dislocation can damage several important ligaments, blood vessels, and nerves. The health and integrity of the joint and leg may be at risk. Simultaneous dislocation of knee and ankle joint in an ipsilateral limb is a very rare pattern of injury and only few cases have been reported as per literature [1]. A thorough review of literature identified only 15 cases of ipsilateral hip and knee dislocation [2], two cases of ipsilateral hip, knee, and ankle dislocation, but no single case of ipsilateral lateral knee dislocation and ankle fracture dislocation was found [3]. We are going to present and discuss a similar case with ipsilateral knee dislocation along with ankle fracture dislocation of the lower limb and its associated management and difficulties encountered along with it.
A 37-year-old farmer while working in farms sustained injury to his right leg by tiller machine. He was brought to local hospital where he was referred to our institute. On initial examination, his Glasgow Coma Scale was found to be 15, and his vitals were stable. 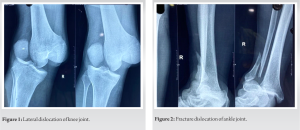 His right knee and ankle were grossly deformed. On clinical examination, right knee and tibia were dislocated laterally. The ankle was also found to be dislocated anteriorly. No other significant systemic or associated musculoskeletal injuries were noted. The patient was adequately resuscitated as per advanced trauma life support protocol. The distal pulses were present on both legs, and capillary flow was adequate. Regular monitoring of the capillary blood flow using continuous pulse oximetry was carried out.
His right knee and ankle were grossly deformed. On clinical examination, right knee and tibia were dislocated laterally. The ankle was also found to be dislocated anteriorly. No other significant systemic or associated musculoskeletal injuries were noted. The patient was adequately resuscitated as per advanced trauma life support protocol. The distal pulses were present on both legs, and capillary flow was adequate. Regular monitoring of the capillary blood flow using continuous pulse oximetry was carried out.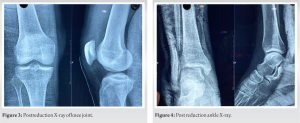 Radiographic examination was carried out, and the patient sustained the following injuries to his right lower limb:
Radiographic examination was carried out, and the patient sustained the following injuries to his right lower limb:
- Lateral dislocation of the knee joint (Fig. 1).
- Anterior fracture dislocation of ankle (Fig. 2).
The patient underwent an immediate closed reduction of the dislocated knee joint (Fig. 3) taking care to prevent further injury to the joint. Simultaneous reduction of ankle joint (Fig. 4) was done, and appropriate splintage was given. Post-reduction distal pulses were palpable, and there was no neural deficit also. The patient was prepared for emergency surgery. On table, knee was examined and found Grade 3 lateral collateral ligament injury and posterior cruciate ligament injury.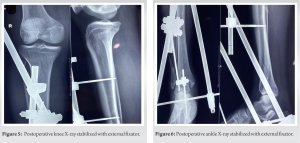 Knee and ankle were stabilized with external fixator (Fig. 5 and 6). At a second stage, after 1 week, the lateral malleolus fracture was operated, and open reduction and internal fixation were done with recon plates and two screws were inserted for syndesmotic injury (Fig. 7).
Knee and ankle were stabilized with external fixator (Fig. 5 and 6). At a second stage, after 1 week, the lateral malleolus fracture was operated, and open reduction and internal fixation were done with recon plates and two screws were inserted for syndesmotic injury (Fig. 7).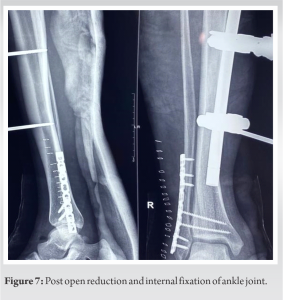 The post-operative period was uneventful. After 6 weeks, the transarticular fixator was removed, and a knee immobilizer was given. The knee joint was further assessed for ligamentous injuries, and a magnetic resonance imaging scan was done which revealed an posterior cruciate and lateral collateral ligament injury. The need for knee ligament reconstruction was discussed with the patient.
The post-operative period was uneventful. After 6 weeks, the transarticular fixator was removed, and a knee immobilizer was given. The knee joint was further assessed for ligamentous injuries, and a magnetic resonance imaging scan was done which revealed an posterior cruciate and lateral collateral ligament injury. The need for knee ligament reconstruction was discussed with the patient.
To our knowledge, there were no reported cases of a patient with simultaneous traumatic ipsilateral dislocations of knee joint with associated ankle joint dislocation with ankle fracture. However, ipsilateral hip, knee, and ankle fracture dislocation was reported earlier. In 2004, Vasali and Seara reported ipsilateral knee, foot, and ankle dislocation and managed with closed reduction of dislocated joints [4]. In 1984, Malimson reported a case of ipsilateral fracture dislocations of the hip and knee and a fracture-dislocation of the tarsometatarsal joints [5]. In 1991, Millea et al. described a case of ipsilateral fracture-dislocations of the hip and knee and an open fracture-dislocation of the ankle [6]. However, in our case, there was no associated fracture with the knee dislocation, but the only fracture involving the ankle joint, making it a unique pattern to be reported [7]. The three dislocations described in these two reports had associated fractures. Pure tibiotalar dislocations, without associated malleolar fractures, are rare [8,9]. In 2011, Waterman and Banerjee had reported a rare case and the only to be reported in the literature so far, of a case of simultaneous hip, knee, and ankle dislocation in a single limb [3]. A study carried out by Jones et al. had concluded that 45% of posterior knee dislocations were associated with a vascular injury which makes it of utmost importance to recognize such dislocations and reduced it immediately [10]. A knee dislocation is the worst of the worst. In broad terms, the knee is stabilized by four ligaments – the anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, and lateral collateral ligament [11]. A knee dislocation means that, at least three and sometimes all four, of these ligaments are ruptured. It is a very high-energy injury, and there is risk of nerve and blood vessel damage when this occurs. There always lies a high risk of hemodynamic instability and other serious and life-threatening injuries due to the high velocity of trauma involved in such cases. A high index of clinical suspicion is required along with the knowledge of mechanism and pattern of these injuries to suspect such injuries which are generally masked by the graveness of other injuries. A thorough and meticulous clinical examination to identify such injuries and rule out any associated neurovascular injury. Computed tomography (CT) scan of the hip, knee, and ankle joints to assess the joint and identify fracture morphologies is also required. CT–angiography of the limb before and after reduction of the joints is also a necessity. Magnetic resonance imaging scans are increasingly being advised to be done at follow-ups to associated meniscal or cruciate injuries in the knee joint. The outcome of ipsilateral knee and ankle dislocation can vary widely depending on the circumstances and other associated injuries. Since there has been no known case of such an injury pattern reported in the literature, this case turns out to be the first and unique case to be reported. Postoperatively, the patient had congruent reduction in knee and ankle joint. Factors that were surgeon controlled that could improve outcome include emergent reduction of the dislocated joint and stabilization of the reduced joint preferably in the emergency room, assessment of neurovascular injury, and management of the multiligament knee injury on an elective basis.
Dislocation of any joint is treated as an orthopedic emergency. Simultaneous dislocation of knee and ankle joints in an ipsilateral limb is a challenging situation for even the experienced surgeon. The outcome of such patients varies with associated injuries and time took for relocation and meticulous physical examination with a high index of clinical suspicion is needed in diagnosing and management of such cases.
Thorough clinical examination in toto is imperative in the setting of high energy trauma. There may be associated injuries of the same limb or elsewhere in the scenario of complex trauma mechanisms. Through this case report, we want to make others aware of the unusual presentations which are less commonly seen in clinical practice and enrich our knowledge in today evidence-based clinical world.
References
- 1.Schmidt GL, Sciulli R, Altman GT. Knee injury in patients experiencing a high-energy traumatic ipsilateral hip dislocation. J Bone Joint Surg Am 2005;87:1200-4. [Google Scholar | PubMed]
- 2.Tabuenca J, Truan JR. Knee injuries in traumatic hip dislocation. Clin Orthop 2000;377:78-83. [Google Scholar | PubMed]
- 3.Waterman BR, Banerjee R. Management of simultaneous ipsilateral dislocation of hip, knee, and ankle. Am J Orthop 2011;40:301-4. [Google Scholar | PubMed]
- 4.Vasali AS, Seara JL. Ipsilateral dislocation of knee, foot and ankle. Arch Orthop Trauma Surg 2020;124:418-20. [Google Scholar | PubMed]
- 5.Malimson PD. Triple fracture-dislocation of the lower limb. Injury 1984;16:11-2. [Google Scholar | PubMed]
- 6.Millea TP, Romanelli RR, Segal LS, Lynch CJ. Ipsilateral fracture-dislocation of the hip, knee, and ankle: Case report. J Trauma 1991;31:416-9. [Google Scholar | PubMed]
- 7.Hatori M, Kotajima S, Smith RA, Kokubun S. Ankle dislocation without accompanying malleolar fracture. A case report. Ups J Med Sci 2006;111:263-8. [Google Scholar | PubMed]
- 8.Rivera F, Bertone C, De Martino M, Pietrobono D, Ghisellini F. Pure dislocation of the ankle: Three case reports and literature review. Clin Orthop 2001;382:179-84. [Google Scholar | PubMed]
- 9.Soyer AD, Nestor BJ, Friedman SJ. Closed posteromedial dislocation of the tibiotalar joint without fracture or diastasis: A case report. Foot Ankle Int 1994;15:622-4. [Google Scholar | PubMed]
- 10.Jones RE, Smith EC, Bone GE. Vascular and orthopaedic complications of knee dislocation. Surg Gynecol Obstet 1979;149:554-8. [Google Scholar | PubMed]
- 11.Gillespie WJ. The incidence and pattern of knee injury associated with dislocation of the hip. J Bone Joint Surg Br 1975;57:376-8. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Medial Subtalar Joint Dislocation in an 18-Year-Old Athlete with Pes Planus: Beyond A Simple Misstep
August 1, 2026 Medial Subtalar Joint Dislocation in an 18-Year-Old Athlete with Pes Planus: Beyond A Simple Misstep August 1, 2026 Complex Irreducible Dislocation of the Fourth Toe Proximal Interphalangeal Joint in a 5-year-old Boy Fixed by Soft Anchor: A Case Report
August 1, 2026 Complex Irreducible Dislocation of the Fourth Toe Proximal Interphalangeal Joint in a 5-year-old Boy Fixed by Soft Anchor: A Case Report May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report
May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report April 1, 2026 Dislocation and Iatrogenic Dissociation of Bipolar Hip Hemiarthroplasty: A Case Series and Literature Review
April 1, 2026 Dislocation and Iatrogenic Dissociation of Bipolar Hip Hemiarthroplasty: A Case Series and Literature Review