
The learning objective is to explore the benefits and limitations of bone grafts, including autografts, for treating locked posterior shoulder dislocation with a reverse Hill–Sachs lesion, particularly in economically constrained patients.
Dr. Bhagya R Shah, Department of Orthopaedics, Smt. B. K. Shah Medical Institute and Research Center, Sumandeep Vidyapeeth Deemed to be University, Vadodara, Gujarat, India. E-mail: bhagyashah.com@gmail.com
Abstract
Introduction: Posterior glenohumeral joint dislocations are uncommon injuries. The disease often goes undiagnosed and untreated despite positive clinical signs. In the event of a large humeral bone defect, the outcome may be worse.
Case Report: This case report presents a 47-year-old man with a 2-year-old locked posterior shoulder dislocation with a large segmental bone defect involving 40% of the humeral head’s articular surface. We decided to treat the patient with an open reduction of the shoulder dislocation and reconstruction of the articular surface with iliac crest autograft. We observed an improvement in shoulder mobility and range of motion on all planes, which were beneficial to the patient’s daily activities; at follow-up, no pain was reported.
Conclusion: Our case report demonstrates that locked posterior shoulder dislocations with a large bone defect and viable humeral head can be treated using an autograft. This will result in optimal clinical results and avoid early prosthetic replacement surgery. Autograft may be a preferred method in the presence of economic constraints or due to the unavailability of allografts or implants.
Keywords: Posterior shoulder dislocation, locked posterior shoulder dislocation, reverse hill-sachs lesion, impaction fractures of the anterior humeral head, reverse Bankart lesion, posterior bony glenoid and labrum capsular complex lesions, rotator cuff tears.
Posterior glenohumeral joint (GHJ) dislocation is an infrequent injury with an incidence of only 2–5% of all shoulder joint dislocations [1]. Shoulder posterior dislocation has a prevalence of 1.1/100,000 per year. This prevalence has the first peak in male patients aged between 20 and 49 years old and the second peak in the elderly over seventy [2]. Posterior shoulder dislocation is often missed and undertreated in up to 50% of cases admitted to the ER [3]. Classically, a dislocation is defined as chronic when it presents after more than 3 weeks. Diagnosis of posterior shoulder dislocations is often delayed and is prone to becoming chronic, and leading to a locked joint requiring open reduction. Posterior shoulder dislocations can be of two types: (1) Traumatic or (2) Atraumatic: The first might be due to direct high-energy trauma or a repetitive minor injury. A major trauma with a force applied to the arm from the front with the shoulder in adduction, flexion, and internal rotation is the most common mechanism of injury. On the other hand, seizures and electrocution are the major causes of atraumatic dislocations. This is due to the contraction of the internal rotators and disruption of the joint static and dynamic posterior stabilizers [1]. Sometimes, posterior shoulder dislocations may also present in an individual with hyperlaxity (Beighton score >5 out of 9) as a part of global instability but are easily reducible and rarely complicated as a locked posterior dislocation. It may be associated with humeral neck or tuberosity fractures. Reverse Hill-Sachs lesion (impact fractures of the anterior humeral head), reverse Bankart lesion (posterior bony glenoid and labrum capsular complex lesions) and rotator cuff tears. Reverse Hill-Sachs lesions are seen in posterior shoulder dislocations in up to 86% of cases, often requiring open or arthroscopic surgical therapy [1,4,5]. If undiagnosed, it may lead to significant clinical problems, as it can predispose to serious complications, such as chronic instability, osteonecrosis, osteoarthritis, persistent joint stiffness, and pseudoarthrosis, limiting functional outcomes [5]. Management of chronic locked posterior shoulder dislocation associated with a large articular defect is challenging as there is no common consensus around it. The patient gave consent for the case report.
A 47-year-old man, post-seizure, sustained muscle contractions leading to his left shoulder injury. The patient was employed as a housekeeper. At the time of the seizure, he had been admitted to the ER of another hospital, where he had been discharged with the diagnosis of “left shoulder contusion.” The patient was admitted to our clinic 2 years after the trauma, complaining of severe pain and functional limitations of the left shoulder. On physical examination, the patient showed functional limitation of the shoulder motion on all planes, in particular: adduction 10°, abduction 20°, flexion 30°, extension 10°, internal rotation 30°, and external rotation 0°. At palpation, the shoulder was painful. The patient was neurovascular intact. X-ray and CT scans were carried out, showing posterior shoulder dislocation with an osteocartilaginous lesion about 40% of the humeral head surface, localized on its anteromedial edge, representing a reverse Hill-Sachs lesion; type I according to Randelli’s classification (Fig. 1 & Fig. 2).
The patient was neurovascular intact. X-ray and CT scans were carried out, showing posterior shoulder dislocation with an osteocartilaginous lesion about 40% of the humeral head surface, localized on its anteromedial edge, representing a reverse Hill-Sachs lesion; type I according to Randelli’s classification (Fig. 1 & Fig. 2). MRI was done to evaluate associated rotator cuff injury muscle atrophy and cartilage damage (Fig. 3).
MRI was done to evaluate associated rotator cuff injury muscle atrophy and cartilage damage (Fig. 3). The joint was not reducible with close methods, and after a radiological evaluation, the patient was scheduled for surgery. Considering the age of the patient, his high functional demand, and the extension of the lesion, we decided to perform an iliac crest autograft reconstruction. The procedure was performed under general anesthesia, with the patient placed in a beach chair position. A standard deltopectoral approach was used with the release of the upper pectoralis major tendon insertion to improve the exposure of the surgical field. After finding and isolating the anterior humeral circumflex artery and vein, the subscapularis tendon was exposed and cut through 1 cm medial from its insertion. After detaching the subscapularis muscle from the lesser tuberosity, as the long head of the biceps brachii (LHB) tendon tended to dislocate from the bicipital groove, we decided to do a biceps tenotomy. We removed all the fibrosis and adhesion around the humeral head, and then the posteriorly dislocated locked humeral head was gently reduced with the aid of a Schanz pin inserted in the lateral aspect of the humeral shaft used as a joystick and spikes. Subsequently, a large, 40% reverse Hill-Sachs lesion and reverse bankart was exposed (Fig. 4 a, Fig. 4 b).
The joint was not reducible with close methods, and after a radiological evaluation, the patient was scheduled for surgery. Considering the age of the patient, his high functional demand, and the extension of the lesion, we decided to perform an iliac crest autograft reconstruction. The procedure was performed under general anesthesia, with the patient placed in a beach chair position. A standard deltopectoral approach was used with the release of the upper pectoralis major tendon insertion to improve the exposure of the surgical field. After finding and isolating the anterior humeral circumflex artery and vein, the subscapularis tendon was exposed and cut through 1 cm medial from its insertion. After detaching the subscapularis muscle from the lesser tuberosity, as the long head of the biceps brachii (LHB) tendon tended to dislocate from the bicipital groove, we decided to do a biceps tenotomy. We removed all the fibrosis and adhesion around the humeral head, and then the posteriorly dislocated locked humeral head was gently reduced with the aid of a Schanz pin inserted in the lateral aspect of the humeral shaft used as a joystick and spikes. Subsequently, a large, 40% reverse Hill-Sachs lesion and reverse bankart was exposed (Fig. 4 a, Fig. 4 b). The fresh iliac crest autograft was then carefully prepared aside to obtain an anatomical restoration of the head anatomy (Fig. 4 c). The size-matched autograft was prepared, press-fit into the humeral defect, and fixed with two 4.0 mm lag screws (Fig. 4 d). The screws were countersinked to prevent glenoid erosion. Still, the shoulder joint was unstable due to a reverse Bankart defect. The posterior glenoid defect was exposed using the posterior approach of the shoulder with superficial dissection between the deltoid and infraspinatus and deep dissection between the infraspinatus and teres minor. Recurrent posterior translation was fixed via posterior approach using one 4.0mm lag screw, and the defect was filled again with fresh iliac autograft (Figure 4e). The rotator cuff was repaired using a No. 5 ethibond suture. Post op Xray was taken (Fig. 5).
The fresh iliac crest autograft was then carefully prepared aside to obtain an anatomical restoration of the head anatomy (Fig. 4 c). The size-matched autograft was prepared, press-fit into the humeral defect, and fixed with two 4.0 mm lag screws (Fig. 4 d). The screws were countersinked to prevent glenoid erosion. Still, the shoulder joint was unstable due to a reverse Bankart defect. The posterior glenoid defect was exposed using the posterior approach of the shoulder with superficial dissection between the deltoid and infraspinatus and deep dissection between the infraspinatus and teres minor. Recurrent posterior translation was fixed via posterior approach using one 4.0mm lag screw, and the defect was filled again with fresh iliac autograft (Figure 4e). The rotator cuff was repaired using a No. 5 ethibond suture. Post op Xray was taken (Fig. 5). Post-op shoulder arm immobilizer in the neutral rotation was given for 4 weeks. After it, passive range of motion Physiotherapy was done for 4 weeks, followed by active physiotherapy, and a rotator cuff strengthening protocol was initiated. We did Xray and range of movement assessment at week 2,4,6 and 12 (Fig. 6, Fig. 7) . Functionally, the patient was very satisfied with the improved range of motion and strength and was able to join his work, which he could not do for the past 2 years due to this injury.
Post-op shoulder arm immobilizer in the neutral rotation was given for 4 weeks. After it, passive range of motion Physiotherapy was done for 4 weeks, followed by active physiotherapy, and a rotator cuff strengthening protocol was initiated. We did Xray and range of movement assessment at week 2,4,6 and 12 (Fig. 6, Fig. 7) . Functionally, the patient was very satisfied with the improved range of motion and strength and was able to join his work, which he could not do for the past 2 years due to this injury.
The aim of this case report is to present the clinical results using an iliac crest autograft in an active patient affected by a chronic posterior GHJ dislocation with a reverse Hill-Sachs lesion of about 40% and a reverse Bankart lesion. Scientific literature shows scarce consensus about the treatment of this rare injury; there is an ongoing debate about the different treatment options. As well, no consensus exists on which autograft is best. The reverse Hill-Sachs lesion size is the most influencing factor for choosing this type of treatment [3]. The reverse Hill-Sachs (also called McLaughlin lesion) is a wedge-shaped impaction fracture on the anteromedial aspect of the humeral head [4]. Any significant lesion should be treated operatively [5]. According to Guehring et al., for defects involving <25% of the articular surface, closed reduction is the first choice of treatment; patients with unstable joints and bone defects >25% could benefit from operative treatment, with arthroplasty being recommended if the bone defect is >40%. For defects between 25% and 40%, a plethora of treatment modalities can be adopted, including the classical or modified McLaughlin technique, bone grafts, etc. [6,7]. In our patient, we opted for an iliac crest autograft to obtain an anatomical restoration. We preferred this procedure to non-anatomic procedures such as subscapularis tendon transfer (i.e., classic McLaughlin) or the lesser tuberosity transfer (i.e., modified McLaughlin) because, according to the authors, a non-anatomic restoration of the humeral head sphericity can lead to a decreased internal rotation of the shoulder and can complicate a foreseeable prosthetic reconstruction [3]. Our patient had borderline indications for hemiarthroplasty. Considering his age and global clinical assessment, we decided to perform an autograft procedure to respect the patient’s high functional demand for the affected limb. Furthermore, we agree with the author’s alertness on the difficulty to manage moderate-sized Hill Sachs lesions (i.e., sizing between 40 and 55%), even for experienced shoulder surgeons: young and middle-aged individuals with high functional demand can benefit from a delay in hemiarthroplasty surgery by preserving the sphericity of the humeral head [8]. Concerning the graft type, most literature focuses on cancellous allografts or autografts to treat acute posterior shoulder dislocation. These grafts are used as void filler after lifting off the previously impacted articular surface to better stabilize the lesion gap and promote bone healing [1]. No specific guideline has been proposed for the choice of the autograft. Some authors used a fresh-frozen femoral head allograft. In particular, authors report good functional outcomes using a femoral head allograft for treating locked chronic posterior shoulder dislocation in patients with 25–50% articular surface bony defects [1,9,10,11]. The same good results are described in a case report by Patrizio and Sabetta [10]. The most frequent possible complications recorded with this procedure are graft resorption, articular surface flattening, and arthritis. The use of fresh iliac crest autograft has been described by Martinez et al. [1]. in 5 patients affected by GHJ instability after posterior GH dislocation and in 1 patient with chronic GH dislocation. All patients had a 40% humeral defect. The study had a follow-up period of 10 years; 4 patients had satisfying outcomes, while 2 suffered graft collapse. On comparing our case with the above-mentioned paper, we obtained an autograft from the iliac crest of size accurate to the humerus defect. By doing so, we were able to better fill the gap and restore the precise curvature of the humeral head of the patient. Using an autograft from the iliac crest, we preserved shoulder stability, function, and anatomic soft tissue attachments while preserving the remaining articular surface. Our case report showed how operative treatment options must be patient-targeted according to each intrinsic factor (e.g., age, functional demand, comorbidities, etc.), the type of injury (e.g., extension of bone defects), and its severity [12,13]. Our patient had a functional demand influencing his work-related activities and reported consistent pain for up to 2 years. Patients with posterior GHJ dislocation suffer a diagnosis delay and often report specific symptoms during healthcare evaluation [14,15]. Our patient as well had specific symptoms; apart from significant pain and loss of motion, patients with chronic GHJ dislocation may show shoulder muscle atrophy and prominent acromion when compared with the opposite side, while the dislodged humeral head can be palpated on the back of the shoulder. XR findings can mislead clinicians as the AP view could show no sign of posterior GHJ dislocation; axillary-lateral or Y views (hard to obtain if consistent pain is present), CT scan, and/or, as in our case, an MRI can unmask the dislocation. Diagnosis delay pivots the treatment: in a case series study, it is highlighted how patients promptly treated for acute dislocation have a better outcome and are easier to treat [16]. During follow-up, our patient has undergone rehabilitation therapy; post-operative recovery consists of strengthening exercises and neuromuscular re-education while educating the patient to avoid flexion, adduction, and internal rotation movements. We acknowledge that the limitation of this report is its limited follow-up.
In conclusion, early diagnosis of posterior GHJ dislocation is of paramount importance in effectively managing this condition. When a reverse Hill-Sachs lesion is present, it highlights the necessity for standardized treatment protocols to address it. However, it is noteworthy that our literature search encountered a significant limitation due to the limited number of studies investigating locked posterior shoulder dislocation with a reverse Hill–Sachs lesion. Therefore, we strongly advocate for future research that explores the potential benefits and limitations, particularly focusing on the use of bone grafts in such cases. We suggest using bone grafts to preserve anatomy in young and active patients. Even if the graft procedure fails, there is still the possibility to do a salvage procedure (prosthetic replacement) at a later stage. Autograft may be a preferred method in the presence of economic constraints or due to the unavailability of allografts or implants.
The timely identification of posterior GHJ dislocation plays a crucial role in effectively handling this condition. The presence of a reverse Hill-Sachs lesion further emphasizes the need for standardized treatment approaches to specifically address this aspect.
References
- 1.Martinez AA, Calvo A, Domingo J, Cuenca J, Herrera A, Malillos M. Allograft reconstruction of segmental defects of the humeral head associated with posterior dislocations of the shoulder. Injury 2008;39:319-22. [Google Scholar | PubMed]
- 2.Antonio AA, Navarro E, Iglesias D, Domingo J, Calvo A, Carbonel I. Long-term follow-up of allograft reconstruction of segmental defects of the humeral head associated with posterior dislocation of the shoulder. Injury 2013;44:488-91. [Google Scholar | PubMed]
- 3.Aydin N, Kayaalp ME, Asansu M, Karaismailoglu B. Treatment options for locked posterior shoulder dislocations and clinical outcomes. EFORT Open Rev 2019;4:194-200. [Google Scholar | PubMed]
- 4.Shah N, Tung GA. Imaging signs of posterior glenohumeral instability. Am J Roentgenol 2009;192:730-5. [Google Scholar | PubMed]
- 5.Bock P, Kluger R, Hintermann B. Anatomical reconstruction for Reverse Hill-Sachs lesions after posterior locked shoulder dislocation fracture: A case series of six patients. Arch Orthop Trauma Surg 2007;127:543-7. [Google Scholar | PubMed]
- 6.Perrenoud A, Imhoff AB. Locked posterior dislocation of the shoulder. Bull Hosp Jt Dis 1996;54:165-8. [Google Scholar | PubMed]
- 7.Mastrokalos DS, Panagopoulos GN, Galanopoulos IP, Papagelopoulos PJ. Posterior shoulder dislocation with a reverse Hill–Sachs lesion treated with frozen femoral head bone allograft combined with osteochondral autograft transfer. Knee Surg Sport Traumatol Arthrosc 2017;25:3285-8. [Google Scholar | PubMed]
- 8.Murphy LE, Tucker A, Charlwood AP. Fresh frozen femoral head osteochondral allograft reconstruction of the humeral head reverse hill Sachs lesion. J Orthop 2018;15:772-5. [Google Scholar | PubMed]
- 9.Gerber C, Lambert SM. Allograft reconstruction of segmental defects of the humeral head for the treatment of chronic locked posterior dislocation of the shoulder. J Bone Jt Surg Ser A 1996;78:376-82. [Google Scholar | PubMed]
- 10.Patrizio L, Sabetta E. Acute posterior shoulder dislocation with reverse Hill Sachs lesion of the epiphyseal humeral head. ISRN Surg 2011;2011:851051. [Google Scholar | PubMed]
- 11.Provencher MT, LeClere LE, Ghodadra N, Solomon DJ. Postsurgical glenohumeral anchor arthropathy treated with a fresh distal tibia allograft to the glenoid and a fresh allograft to the humeral head. J Shoulder Elbow Surg 2010;19:e6-11. [Google Scholar | PubMed]
- 12.Burkhead WZ, Rockwood CA. Treatment of instability of the shoulder with an exercise program. J Bone Jt Surg Ser A 1992;74:890-6. [Google Scholar | PubMed]
- 13.Fronek J, Warren RF, Bowen M. Posterior subluxation of the glenohumeral joint. J Bone Jt Surg Ser A 1989;71:205-16. [Google Scholar | PubMed]
- 14.Sahajpal DT, Zuckerman JD. Chronic glenohumeral dislocation. J Am Acad Orthop Surg 2008;16:385-98. [Google Scholar | PubMed]
- 15.Rowe CR, Zarins B. Chronic unreduced dislocations of the shoulder. J Bone Jt Surg Ser A 1982;64:494-505. [Google Scholar | PubMed]
- 16.Pavone V, Caruso VF, Chisari E, Mangano S, Testa G, Costa D, et al. Surgical and rehabilitative treatment of misdiagnosed posterior dislocation of the shoulder: Case series. J Funct Morphol Kinesiol 2018;3:30. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Rare Subscapularis Anterior Leading Edge Tear following Traumatic Posterior Shoulder Dislocation: A Case Report
December 1, 2025 Rare Subscapularis Anterior Leading Edge Tear following Traumatic Posterior Shoulder Dislocation: A Case Report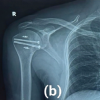 August 1, 2025 Surgical Management of Chronic Locked Posterior Dislocation of Shoulder using the Modified McLaughlin Procedure
August 1, 2025 Surgical Management of Chronic Locked Posterior Dislocation of Shoulder using the Modified McLaughlin Procedure October 10, 2022 Asymmetric Bilateral Chronic Shoulder Dislocation in a Young Patient – A Rare Case Report
October 10, 2022 Asymmetric Bilateral Chronic Shoulder Dislocation in a Young Patient – A Rare Case Report October 1, 2025 Faculty Development and Support in Orthopedic Education: A Narrative Review
October 1, 2025 Faculty Development and Support in Orthopedic Education: A Narrative Review