
The learning point from this report is that uncemented total hip replacement with an autologous structural femoral head graft is a suitable treatment method for neglected Pipkin Type 4 fractures.
Dr. Bhashker Rai, Department of Orthopaedics, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India. E-mail: direct2bhaskar@gmail.com
Introduction: Pipkin type 4 fracture is defined as hip dislocation with femoral head fracture and concomitant acetabular rim fracture. These fractures are rare. Neglected fractures develop adaptive changes in the acetabulum, femoral head, and soft tissues around the hip joint, leading to hip arthritis. Total hip arthroplasty is preferred in such cases. After an extensive literature review, we did not find any guidelines for managing neglected Pipkin type 4 fractures.
Case Report: A 47-year-old male presented with pain in his left hip and an inability to bear weight on his left lower limb. He had a road traffic accident 1 year ago. On clinical examination, there was a shortening of 3 cm and reduced hip range of motion on 3D computed tomography posterosuperior defect of the acetabular wall along with Pipkin type 4 femoral head fracture was detected. Total hip arthroplasty with acetabular reconstruction using a femoral head autograft was done. At 1 year of follow-up, the patient was pain-free and could walk without any assistance with a normal gait.
Conclusion: Uncemented total hip arthroplasty with an autologous structural femoral head graft is a suitable method of treatment for neglected Pipkin type 4 fractures. It preserves bone stock and does not add any financial burden.
Keywords: Pipkin type 4, neglected acetabular fracture, total hip arthroplasty.
Pipkin type 4 fractures are defined as hip dislocations with femoral head fractures and concomitant acetabular rim fractures. These fractures are rare [1]. Although internal fixation is a treatment of choice in fresh cases, it is associated with poor outcomes [2]. Neglected pipkin type 4 fractures present a whole different set of challenges and complications [3]. The neglected fractures develop adaptive changes in the acetabulum, femoral head, and soft tissues around the hip joint, leading to hip arthritis [2, 3]. Total hip arthroplasty is a preferred treatment choice in such neglected cases [4, 5]. The extensive fibrosis, acetabulum defects, and chronic muscular adaptation make the approach more arduous and technically demanding. After an extensive literature review, we found no guidelines for managing neglected Pipkin type 4 fractures. We are reporting this case due to its rarity, where a neglected acetabular fracture with a Pipkin type 4 femoral head fracture has been treated by total hip arthroplasty with femoral head grafting.
A 47-year-old male had a road traffic accident 1 year ago. He presented with pain in his left hip and an inability to bear weight on his left lower limb. Clinical examination showed a shortening of 3 cm and a reduced hip range of motion. There was no distal neurovascular deficit. On the radiograph, an acetabular fracture with a Pipkin type 4 femoral head fracture on the left side was noted (Fig. 1a). On 3-D computed tomography, posterosuperior defects of the acetabular wall (AAOS type 1A, Paprosky type 2B) and a Pipkin type 4 femoral head fracture with posterior hip dislocation were detected (Fig. 1b).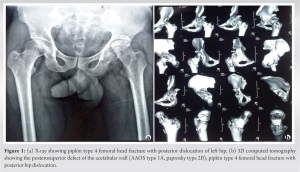 Pseudo-acetabulum formation was also apparent. With the patient in the right lateral position, an incision was given per the standard posterior approach. The gluteus maximus was split, and short external rotators were tagged and cut. A neck cut was taken, and the femoral head was kept carefully. Postero-superior acetabulum wall defect and pseudo-acetabulum were identified (Fig. 2).
Pseudo-acetabulum formation was also apparent. With the patient in the right lateral position, an incision was given per the standard posterior approach. The gluteus maximus was split, and short external rotators were tagged and cut. A neck cut was taken, and the femoral head was kept carefully. Postero-superior acetabulum wall defect and pseudo-acetabulum were identified (Fig. 2).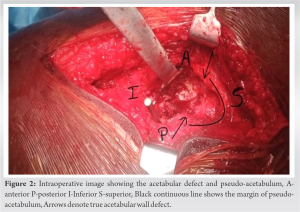 The acetabulum was cleared of all fibrosed tissues to expose the true acetabular margin and transverse acetabular ligament. Then the femoral head was used as an autograft to cover the defect and fixed with two 4mm cancellous screws. Sequential reaming was done in proper orientation to make the graft congruent with the remaining acetabular margin (Fig. 3).
The acetabulum was cleared of all fibrosed tissues to expose the true acetabular margin and transverse acetabular ligament. Then the femoral head was used as an autograft to cover the defect and fixed with two 4mm cancellous screws. Sequential reaming was done in proper orientation to make the graft congruent with the remaining acetabular margin (Fig. 3).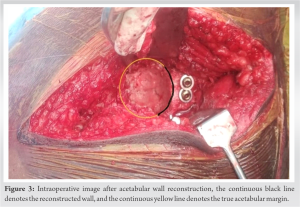 The acetabular shell (Duraloc, DepuyTM, Warsaw) was fitted and fixed with one postero-superior screw. The stability of the cup, along with the graft, was checked. In cases of acetabulam defects where three-point fixation is possible, uncemented cups and cemented cups with impaction grafting have similar results [6, 7]. In segmental acetabular defects where three-point fixation is not possible and a shelf or bulk autograft is required, uncemented cups do well [8]. Seeping of cement between graft and acetabular wall, and hence preventing graft union, was another reason for choosing an uncemented cup. After femoral canal preparation, the femoral stem was inserted. The head was mounted, and a trial reduction was made. The hip was stable within the range of motion with the restoration of the limb length (Fig. 4).
The acetabular shell (Duraloc, DepuyTM, Warsaw) was fitted and fixed with one postero-superior screw. The stability of the cup, along with the graft, was checked. In cases of acetabulam defects where three-point fixation is possible, uncemented cups and cemented cups with impaction grafting have similar results [6, 7]. In segmental acetabular defects where three-point fixation is not possible and a shelf or bulk autograft is required, uncemented cups do well [8]. Seeping of cement between graft and acetabular wall, and hence preventing graft union, was another reason for choosing an uncemented cup. After femoral canal preparation, the femoral stem was inserted. The head was mounted, and a trial reduction was made. The hip was stable within the range of motion with the restoration of the limb length (Fig. 4). The posterior soft tissue capsular repair was done. For the correction of shortening, restoration of the hip center along with soft tissue release was done. The anterior and posterior capsules, gluteus maximus, and rectus femoris were released. Adductor tenotomy was also performed. Abductors and iliopsoas were not released. Achieving a normal hip center intraoperatively also helped to counteract the problem of shortening. The patient was allowed range-of-motion exercises postoperatively. Weight-bearing was restricted for one and a half months. Then, assisted partial weight bearing was allowed until graft union. The patient was allowed to bear full weight after the union. The patient was followed for 1 year to further evaluate clinical and radiological outcomes. At 1 year of follow-up, the patient was pain-free and could walk without assistance with a normal gait. No limb length discrepancy was present. Harris’s hip score improved from 30 to 85. On follow-up radiographs, graft consolidation was evident without any sign of implant loosening or osteolysis in any of the Gruen, DeLee, or Charnley zones (Fig. 5).
The posterior soft tissue capsular repair was done. For the correction of shortening, restoration of the hip center along with soft tissue release was done. The anterior and posterior capsules, gluteus maximus, and rectus femoris were released. Adductor tenotomy was also performed. Abductors and iliopsoas were not released. Achieving a normal hip center intraoperatively also helped to counteract the problem of shortening. The patient was allowed range-of-motion exercises postoperatively. Weight-bearing was restricted for one and a half months. Then, assisted partial weight bearing was allowed until graft union. The patient was allowed to bear full weight after the union. The patient was followed for 1 year to further evaluate clinical and radiological outcomes. At 1 year of follow-up, the patient was pain-free and could walk without assistance with a normal gait. No limb length discrepancy was present. Harris’s hip score improved from 30 to 85. On follow-up radiographs, graft consolidation was evident without any sign of implant loosening or osteolysis in any of the Gruen, DeLee, or Charnley zones (Fig. 5).
Total hip arthroplasty is a well-accepted treatment for neglected Pipkin type 4 fractures [4, 5]. In our pre-operative planning, we have anticipated the deficient bone stock, restoration of a normal hip center, and pseudo-acetabulum as potent challenges. For the reconstruction of acetabular defects, multiple techniques have been advocated. These include autograft, allograft, oblong acetabular cups, and trabecular metal augments with or without reinforcement cages [9, 10, 11]. Bone grafting is suitable for managing acetabular defects [9]. Structural grafts restore the center of rotation and bone stock, which may be beneficial if subsequent surgeries are required [9]. Vascularization and osteointegration are added benefits that minimize the risk of loosening and dislodgement. Accepting a high hip center, using the jumbo cup, or creating a near-normal hip center using grafts are different choices for managing the hip center and pseudo-acetabulum. The jumbo cup eats much of the native bone, whereas the high hip center leads to abnormal biomechanics. In our case, the hip center was restored with the help of a bone graft to fill the defect. The C-arm image intensifier was a helpful tool for intraoperative assessment of hip center restoration [12]. Uncontained defects involving <50% of the acetabulum (type 3) can be managed with a structural graft [10]. As this graft supports <50% of the cup, an uncemented component can be used without the assistance of a cage [10]. In uncemented total hip arthroplasty with acetabular reconstruction, 88% and 76% cup survival have been demonstrated after 10 and 20 years of follow-up [8]. Implant loosening, sciatic nerve injury, injury to gluteal vessels, infection, and dislocation are some anticipated complications of total hip arthroplasty in post-traumatic cases [3]. The limitation of this study is the shorter duration of follow-up.
Uncemented total hip replacement with an autologous structural femoral head graft is a suitable treatment method for neglected Pipkin type 4 fractures. They also preserve bone stock and do not add any extra financial burden. Extensive pre-operative planning is most important when dealing with these patterns of fractures.
In neglected Pipkin type 4 fractures, total hip arthroplasty with acetabular reconstruction using a femoral head autograft can be a viable and cost-effective solution in a resource-constrained setting.
References
- 1.Enocson A, Wolf O. Pipkin fractures: Epidemiology and outcome. Eur J Trauma Emerg Surg 2022;48:4113-8. [Google Scholar]
- 2.Engel JL, Johnsen P, Patel NK, Satpathy J, Mounasamy V. Pipkin Type IV femoral head fractures: A case series and review of literature. Eur J Orthop Surg Traumatol 2021;31:791-5. [Google Scholar]
- 3.Gautam D, Gupta S, Malhotra R. Total hip arthroplasty in acetabular fractures. J Clin Orthop Trauma 2020;11:1090-8. [Google Scholar]
- 4.Veerappa LA, Tripathy SK, Sen RK. Management of neglected acetabular fractures. Eur J Trauma Emerg Surg 2015;41:343-8. [Google Scholar]
- 5.Ranawat A, Zelken J, Helfet D, Buly R. Total hip arthroplasty for posttraumatic arthritis after acetabular fracture. J Arthroplasty 2009;24:759-67. [Google Scholar]
- 6.Ghanem M, Zajonz D, Heyde CE, Roth A. Acetabular defect classification and management: Revision arthroplasty of the acetabular cup based on 3-point fixation. Orthopade 2020;49:432-42. [Google Scholar]
- 7.Colo E, Rijnen WH, Schreurs BW. The biological approach in acetabular revision surgery: Impaction bone grafting and a cemented cup. Hip Int 2015;25:361-7. [Google Scholar]
- 8.Sternheim A, Abolghasemian M, Safir OA, Backstein D, Gross AE, Kuzyk PR. A long-term survivorship comparison between cemented and uncemented cups with shelf grafts in revision total hip arthroplasty after dysplasia. J Arthroplasty 2013;28:303-8. [Google Scholar]
- 9.Oommen AT, Krishnamoorthy VP, Poonnoose PM, Korula RJ. Fate of bone grafting for acetabular defects in total hip replacement. Indian J Orthop 2015;49:181-6. [Google Scholar]
- 10.Gross AE, Goodman S. The current role of structural grafts and cages in revision arthroplasty of the hip. Clin Orthop Relat Res 2004;429:193-200. [Google Scholar]
- 11.Gill K, Wilson MJ, Whitehouse SL, Timperley AJ. Results using trabecular metalTM augments in combination with acetabular impaction bone grafting in deficient acetabula. Hip Int 2013;23:522-8. [Google Scholar]
- 12.Schofer MD, Pressel T, Heyse T, Schmitt J, Boudriot U. Radiological determination of the anatomic hip centre from pelvic landmarks. Acta Orthop Belg 2010;76:479-85. [Google Scholar]







