
All malignant spinal cord compression necessitates Hodgkins lymphoma screening and careful examination of neurological signs is critical during clinical assessments, as timely surgical intervention greatly impacts recovery potential.
Dr. Jenil Patel, A/25 ,Sardar Smriti Bldg. ,S V Road ,Near Chamunda Circle, Borivali West, Mumbai 400092, India. E-mail: jenilpatel.jp23@gmail.com
Abstract
Introduction: Hodgkin's lymphoma has been observed to rarely manifest with extra nodal involvement, typically occurring in the latter stages of the disease. However, spinal cord compression may also be regarded as a rare predominant symptom to occur in this context. In this case report, we discuss the clinical details of a 37-year-old patient who exhibited upper motor neuron symptoms and gait imbalance. The patient's medical history includes a confirmed diagnosis of Hodgkin’s lymphoma.
Case Report: A 37-year-old male patient reported to the outpatient department with bilateral upper limb weakness and gait impairment. The individual presented as a documented case of previous Hodgkin’s lymphoma, with magnetic resonance imaging (MRI) revealing the presence of anterior epidural soft tissue mass at the C6-D1 vertebral levels. This pathological condition resulted in the compression and posterior displacement of the spinal cord. The patient was scheduled to have an emergency decompression surgery involving a C7 corpectomy and C6-D1 fusion procedure utilizing a mesh cage and plate.
Conclusion: The conventional approach of utilizing only Chemotherapy and Radiotherapy for patients with Hodgkin's lymphoma should be reevaluated, as it is imperative to address neurological symptoms resulting from spinal cord compression which also can indicate the stage of the disease. Incorporating surgical interventions into the treatment plan can contribute to the restoration of function in affected patients.
Keywords: Corpectomy, spinal cord compression, Hodgkin’s Lymphoma(HL), Relapse
Cervical myelopathy resulting from more prevalent aetiologies such as intervertebral disc herniation, ossified posterior longitudinal ligament, and congenital spinal canal stenosis is commonly observed. Hodgkin’s lymphoma is predominantly characterised by the affliction of lymph nodes, resulting in the malignant proliferation of lymphocytes and the development of painless lesions in lymph nodes, blood, and other anatomical locations. Although extra nodal involvement is seen in Hodgkin’s lymphoma, it is rare in Primary Hodgkin’s lymphoma. Malignant Hodgkin’s lymphoma (HL) with extra-nodal involvement is observed in approximately 10-20% of cases, with the gastrointestinal tract being the most affected site (44%), followed by the upper airways (19%). In rarer instances, the disease may extend to the bone (8%) and central nervous system (5%) [1,2]. In a study conducted on a cohort of 42 individuals, it was determined that the incidence of primary lymphoma of the bone leading to neurological spine compression is estimated to be 50%. The majority of these patients typically exhibit symptoms in the advanced stages rather than in the early stages of Hodgkin lymphoma (HL). Additionally, in cases with epithelial tumors, a significant proportion of patients do not live beyond 6 months from the initial development of neurological deficits [3]. Here we report an unusual case of a late onset metastasis of relapsed Hodgkins lymphoma who presented with signs and symptoms of spinal cord compression.
A 37-year-old Male presented to the outpatient clinic with a chief complaint of neck pain accompanied by bilateral upper limb radiculopathy, bilateral upper limb weakness, and gait disturbance. These symptoms have been present for a length of two weeks. There was no documented medical history of fever, night sweats, or weight loss.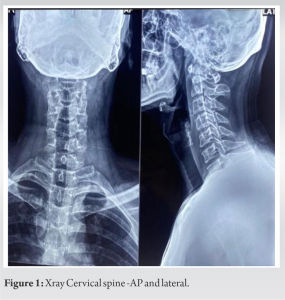 There was no reported history of limb weakness, urine or bowel dysfunction, or trauma. The patient was undergoing treatment with analgesic and neuropathic medications but had no alleviation of symptoms. During the physical examination, the patient exhibited hemodynamic stability, absence of fever, and a normal systemic examination. The patient exhibited pronounced motor weakness in both hand grasp (MRC grade – 3/5) and interossei muscles (MRC grade – 2/5). The observed weakening was found to be correlated with the degeneration of hand muscles.
There was no reported history of limb weakness, urine or bowel dysfunction, or trauma. The patient was undergoing treatment with analgesic and neuropathic medications but had no alleviation of symptoms. During the physical examination, the patient exhibited hemodynamic stability, absence of fever, and a normal systemic examination. The patient exhibited pronounced motor weakness in both hand grasp (MRC grade – 3/5) and interossei muscles (MRC grade – 2/5). The observed weakening was found to be correlated with the degeneration of hand muscles. 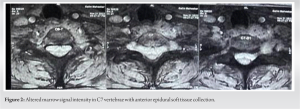 Additionally, the patient exhibited hyperreflexia in both lower limbs, specifically at the knee and ankle joints. There was no detectable presence of lymphadenopathy. The individual in question had a documented diagnosis of Hodgkin’s lymphoma, which had been managed by the administration of chemotherapy and autologous bone marrow transplantation, resulting in a successful remission of the disease.
Additionally, the patient exhibited hyperreflexia in both lower limbs, specifically at the knee and ankle joints. There was no detectable presence of lymphadenopathy. The individual in question had a documented diagnosis of Hodgkin’s lymphoma, which had been managed by the administration of chemotherapy and autologous bone marrow transplantation, resulting in a successful remission of the disease.
Imaging :
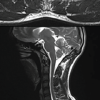
A radiographic examination of the cervical spine was performed, revealing no notable observations. (Fig 1) The results of a cervical MRI scan indicated the presence of an aberration in the marrow signal of the C6-D1 vertebrae.(Fig 2) Additionally, there was anterior epidural soft tissue observed from the C6-D1 vertebral levels, which caused compression and posterior displacement of the spinal cord. (Fig 3) Furthermore, this abnormality encased the bilateral leaving C6 and C7 nerve roots.Prominent paravertebral soft tissues were noted in conjunction with the D1-D3 vertebral levels, exhibiting lateral extension at the apex of the lung.
(Fig 3) Furthermore, this abnormality encased the bilateral leaving C6 and C7 nerve roots.Prominent paravertebral soft tissues were noted in conjunction with the D1-D3 vertebral levels, exhibiting lateral extension at the apex of the lung.
Management :
Due to the presence of observable acute paraparesis and an increased likelihood of progressing to total paraplegia, the patient was scheduled for a surgical procedure known as C7 anterior cervical corpectomy and decompression. Following a corpectomy procedure using a 4mm burr, the spinal cord was decompressed, and the soft tissue mass was carefully retrieved as a specimen for histology and culture analysis. Subsequently, a mesh cage was inserted along with an autologous bone graft to facilitate fusion. Enhanced stability was attained through the utilization of an elongated plate. (Fig 4). The diagnosis of Classical Hodgkin’s Lymphoma was reaffirmed through histopathological analysis of intraoperative samples. (Fig 5). The immunohistochemistry data indicated weak positive expression of CD15 and CD30. The contributions of PAX5 and OCT2 were found to be non-significant. The patient was mobilised postoperatively while wearing a gentle cervical collar on the first day. The patient reported seeing a notable improvement in gait imbalance. Following the surgical procedure, the patient was then referred to his prior oncologist for the purpose of deliberating the initiation of chemotherapy to address the recurrence of the condition.
Hodgkin’s disease primarily manifests as a nodal disorder, frequently affecting lymph nodes, but occurrences of extra nodal illness are infrequent [4]. Magnetic resonance imaging (MRI) is considered the preferred radiological modality for comprehensive examination of the spine in a diagnostic context. The magnetic resonance imaging (MRI) results revealed that secondary involvement in Hodgkin’s lymphoma was characterized by the presence of focal, expansile lesions observed in the cervical and thoracic spine. Conversely, main involvement was associated with multifocal spinal participation. [5] The utilization of FDG-PET scans is crucial in the process of staging, risk stratification, and identification of patients who exhibit insufficient response to chemotherapy and hence require radiation or surgical intervention. The occurrence of additional nodal metastases in Hematological disease are more frequently observed in individuals between the 5th and 6th decade, particularly among males who exhibit a higher prevalence. [6] Patients diagnosed with lymphoma may exhibit distinct epidural masses that exert pressure on the spinal cord. The thoracic and lumbar areas are most susceptible to this compression, although instances of cervical vertebrae involvement have also been documented. [4] A study conducted in China examined the outcomes of five patients diagnosed with non-Hodgkin’s lymphoma and spinal cord compression who received treatment involving radiotherapy and chemotherapy. The results demonstrated notable improvement in neurologic symptoms, even in cases where surgical intervention was not performed. Additionally, the group that underwent surgical decompression exhibited positive outcomes, including improvement in radicular symptoms and neurologic function. [7] Spinal cord compression although an uncommon occurrence outside of the lymph nodes in Hodgkin’s lymphoma (HL), found in approximately 5% of cases and typically associated with worsening or advanced illness.[8] Epidural lesions in Hodgkin’s lymphoma may originate from the spread of blood-borne pathogens, although they are most commonly caused by the invasion of nearby retroperitoneal or thoracic lymph nodes.[9] Given the absence of a conclusive or ideal treatment protocol for such instances, the most effective approach involves administering various methods to address each unique situation and mitigate the risk of neurodeficit. One additional factor that warrants constant consideration and discussion with patients is the existing body of evidence, which indicates that non-ambulatory individuals suffering from spinal cord compression have a relatively low probability, ranging from 10% to 30% of achieving ambulation following surgical interventions. [10,11] Previous research have also indicated that sphincter dysfunction is a prognostic factor that influences the likelihood of recovery.[12]. In the present case, the decision to proceed with surgical decompression was based on the presence of an acute neurodeficit in the patient, as well as the patient’s younger age group. This intervention successfully restored the patient’s normal gait and mitigated the risk of additional deterioration in motor symptoms.
These infrequent case reports provide evidence that Hodgkin lymphoma (HL) should be regarded as a potential end stage etiology for most instances of malignant spinal cord compressions. A comprehensive treatment involving a combination of chemotherapy, radiotherapy, and surgical decompression, when appropriate, can effectively manage patients and yield optimal outcomes. Despite the more diminished likelihood of achieving full remission, the timely identification, classification, and intervention remain crucial in instances with non-Hodgkin’s lymphoma.
Hodgkin’s lymphoma, although infrequent, is a clinically significant condition that can result in spinal cord compression. It is imperative to know the clinical signs and symptoms for prompt and aggressive treatment is sometimes necessary, particularly when accompanied by the acute onset of paraparesis. Effective and timely management strategies can serve to prevent the occurrence of total paraplegia and potentially facilitate the reversal of paraparesis.
References
- 1.Moussaly E, Nazha B, Zaarour M, Atallah JP: Primary non-Hodgkin’s lymphoma of the spine: a case report and literature review. World J Oncol. 2015;6:459-63. 10.14740/wjon947w [Google Scholar | PubMed | CrossRef]
- 2.Ramadan KM, Shenkier T, Sehn LH, Gascoyne RD, Connors JM: A clinicopathological retrospective study of 131 patients with primary bone lymphoma: a population-based study of successively treatedcohorts from the British Columbia Cancer Agency. Ann Oncol 2007;18:129-135. [Google Scholar | PubMed]
- 3.Maranzano E, Latini P. E.ectiveness of radiation therapy without surgery in metastatic spinal cord compression: ®nal results from a prospective trial. Int J Radiat Oncol Biol Physics 1995;32:959-967. [Google Scholar | PubMed]
- 4.Gupta V, Srivastava A, Bhatia B. Hodgkin disease with spinal cord compression. J Pediatric Hematol Oncol. 2009;31(10):771–3. [Google Scholar | PubMed]
- 5.Flanagan EP, O’Neill BP, Porter AB, Lanzino G, Habermann TM, Keegan BM. Primary intramedullary spinal cord lymphoma. Neurology 2011;77(8):784–791. [Google Scholar | PubMed]
- 6.Popescu M, Popov V, Popescu G, Dobrea C, Sandu A, Grigorean VT, Strâmbu V: Spinal involvement with spinal cord compression syndrome in hematological diseases. Rom J Morphol Embryol. 2012;53:1069-72. [Google Scholar | PubMed]
- 7.Peng X, Wan Y, Chen Y, Chen L, He A, Liao W, Shen J, Fu Q, Han S, Li F, Zou X. Primary non-Hodgkin's lymphoma of the spine with neurologic compression treated by radiotherapy and chemotherapy alone or combined with surgical decompression. Oncol Rep. 2009 May;21(5):1269-75. doi: 10.3892/or_00000350. PMID: 19360303. [Google Scholar | PubMed | CrossRef]
- 8.Gupta V, Srivastava A, Bhatia B. Hodgkin disease with spinal cord compression. J Pediatr Hematol Oncol. 2009;31(10):771–773. [Google Scholar | PubMed]
- 9.Ghedira K, Matar N, Bouali S, Zehani A, Boubaker A, Jemel H. Hodgkin Lymphoma revealed by epidural spinal cord compression. J Spinal Cord Med. 2019;42(3):402–404. [Google Scholar | PubMed]
- 10.Makris A, Kunkler IH. The Barthel index in assessing the response to palliative radiotherapy in malignant spinal cord compression: a prospective audit. Clin Oncol 1995;7:82-86. [Google Scholar | PubMed]
- 11.Findlay GF. Adverse e.ects of the management of malignant spinal cord compression. J Neurol Neurosurg Psychiat 1984;47:761-768. [Google Scholar | PubMed]
- 12.Wallington M, Mendis S, Premawardhana U, Sanders P, Shah-savar-Haghighi K. Local control and survival in spinal cord compression from lymphoma and myeloma. Radiother Oncol 1997;42:43-47. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 High-Grade Pancreatic Neuroendocrine Carcinoma Presenting as Dorsal Spinal Cord Compression: A Diagnostic and Surgical Challenge for the Orthopedic Oncologist
December 1, 2025 High-Grade Pancreatic Neuroendocrine Carcinoma Presenting as Dorsal Spinal Cord Compression: A Diagnostic and Surgical Challenge for the Orthopedic Oncologist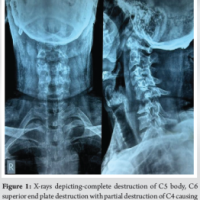 July 10, 2024 Infective Spondylodiscitis of Unknown Origin in a Patient with Chronic Kidney Disease – Case report
July 10, 2024 Infective Spondylodiscitis of Unknown Origin in a Patient with Chronic Kidney Disease – Case report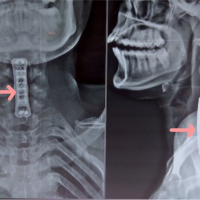 June 10, 2024 A Unique Presentation of Vertebral Body Osteochondroma of Sixth Cervical Spine Causing Myelopathic Symptoms: Management with En bloc Excision and Cervical Fusion
June 10, 2024 A Unique Presentation of Vertebral Body Osteochondroma of Sixth Cervical Spine Causing Myelopathic Symptoms: Management with En bloc Excision and Cervical Fusion March 10, 2024 Discovery of a Novel Yadav–Kunal Reflex in Context of Upper Motor Neuron Lesions: A Report of Three Cases
March 10, 2024 Discovery of a Novel Yadav–Kunal Reflex in Context of Upper Motor Neuron Lesions: A Report of Three Cases