
Fixation of patella fracture using our described technique with suture anchors can achieve solid fixation and provide promising results.
Dr. Madhav Kukreja, Department of Trauma and Orthopaedics, West Hertfordshire Teaching Hospitals NHS Trust, Watford WD18 0HB, United Kingdom. E-mail: namastemadhav@gmail.com
Introduction: Patella fracture can occur due to direct injury to the knee or indirect eccentric contraction of the quadriceps tendon. These injuries can present in different configurations which require acceptable reduction and good fixation. Patients are at risk of not only losing their knee extensor mechanism but also having a defective patellofemoral articulation. Hence, the main aim in treating such fractures is to restore the knee extensor mechanism. Surgical options for treating patella fracture include tension band wiring, wiring through cannulated screws, fixation with plate, and suture anchor (SA) fixation.
Case Report: We demonstrate a new fixation technique for patella fracture with SAs in two of our patients. They presented with patella fracture following a fall and sustained closed injury with intact distal neurovascular status. The authors describe their technique using double-loaded SAs to obtain anatomical reduction and solid fixation. With three SAs, each inserted in a third portion of a distal fragment.
Conclusion: There are several modalities and techniques available for fixation of patella fracture. However, authors recommend that their described novel technique can provide more strength and satisfactory outcome. Furthermore, this technique uses a smaller incision compared to conventional suture tunnel repair as in this technique only the fracture that needs to be exposed distally.
Keywords: Patella fracture, suture anchor, quadriceps tendon.
Patella fracture can be comminuted, transverse, longitudinal split, superior or inferior pole avulsion [1, 2]. Most of these are comminuted and achieving good fixation is technically challenging [3]. The primary goal of treating such fractures is to restore the knee extensor mechanism. Improper management of these injuries may result in the loss of the knee extensor mechanism and defective patellofemoral articulation [4, 5]. Hence, anatomical reduction with good internal fixation and early rehabilitation are important for satisfactory outcome in patients with patellar fracture. Surgical options for treating patella fracture include tension band wiring (TBW), wiring through cannulated screws, fixation with plate, and suture anchor (SA) fixation [6]. TBW is the conventional surgical intervention for treating patellar fracture. Particularly, transverse fracture with large fragments can be easily reduced to obtain and maintain fracture fixation using TBW [7]. A novel technique using SA for patella inferior pole fracture was introduced [8, 9]. However, SA fixation often could not tolerate the pull-out strength of the knee extensor mechanism and powerful quadriceps tendon [10]. We demonstrate a new patella fracture fixation technique with SAs which provides more strength and satisfactory outcome.
The authors describe their technique in two patients. Both patients were operated by senior author (DM). These patients presented with patella fracture following a fall. They sustained closed injury with intact distal neurovascular status. Surgical intervention, benefits, and risks were discussed with patient to obtain an informed written consent. Standard World Health Organization (WHO) checklist was completed. Patients were given general anesthesia after appropriate pre-operative assessment. We did not use pneumatic tourniquet in any of our patients. Parts were prepped and draped in sterile fashion. A standard midline approach was utilized. Hemostasis achieved throughout. Fracture ends appreciated and freshened. Retinacula were evaluated for rupture. Three 5-mm twin fix anchors (Twin Fix Ti, Smith and Nephew) were placed in the distal fragment. These did provide a good solid hold (Fig. 1). Tunnels made in the proximal fragment using 2.5 mm drill in line with anchors. Sutures from anchor were then passed through each tunnel in proximal fragment (Fig. 2).
Tunnels made in the proximal fragment using 2.5 mm drill in line with anchors. Sutures from anchor were then passed through each tunnel in proximal fragment (Fig. 2).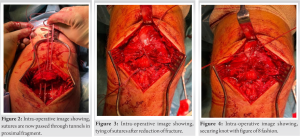 Each anchor is double loaded and one suture of each anchor was whip stitched through the tendon and one left free to pull. The quadriceps tendon was virtually divided into three columns in line with each anchor. The sutures were slid sequentially reducing the bone anatomically. Sutures were then tied (Fig. 3). They were then passed in a Figure of 8 fashion over the bone and into the patellar tendon (Fig. 4). Fracture reduction was confirmed with image intensifier. Knee flexion and stability of repair were checked and was found satisfactory up to 40° of flexion. Medial and lateral retinacula were repaired using size 2 vicryl, followed by closure of subcutaneous tissue and skin.
Each anchor is double loaded and one suture of each anchor was whip stitched through the tendon and one left free to pull. The quadriceps tendon was virtually divided into three columns in line with each anchor. The sutures were slid sequentially reducing the bone anatomically. Sutures were then tied (Fig. 3). They were then passed in a Figure of 8 fashion over the bone and into the patellar tendon (Fig. 4). Fracture reduction was confirmed with image intensifier. Knee flexion and stability of repair were checked and was found satisfactory up to 40° of flexion. Medial and lateral retinacula were repaired using size 2 vicryl, followed by closure of subcutaneous tissue and skin.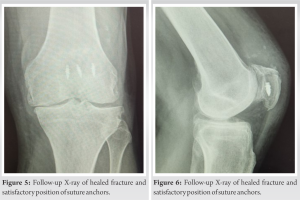
Postoperative rehabilitation involved protecting the repair and wound in an extended knee splint for 2 weeks. This was followed by initiation of flexion in hinged knee brace. From 2nd week postoperatively, knee flexion was allowed up to 30° and this was gradually increased by 30° every 2 weeks. The aim was to obtain full range of movement at 10 weeks postoperatively. Both the patients had adequate input from physiotherapy team throughout the course of rehabilitation. Patients were advised to administer subcutaneous injection of low molecular weight heparin for 6 weeks following surgery. At 6 months post injury, fracture healing was satisfactory with good knee movement and weight bearing in both patients (Fig. 5 and 6).
SAs are used for rotator cuff repairs but, now the indications have been expanded. The suture material is non-absorbable and is composed of an ultra-high molecular weight polyethylene fiber and features a unique braid configuration. Hence, ultrabraid suture offers higher knot breaking strength, increased lubricity, and a stronger resistance to fraying. This is pre-loaded on to TwinFix SA which has two ultrabraid sutures [8]. Egol et al. reported that SA repair provides similar results to metal implants in patellar inferior pole fractures and showed fewer implant-related complications [11]. Anand et al. used two SAs placed at the center of the proximal fragment and reported good clinical outcome [8]. Kadar et al. used two SAs inserted at the center of the proximal fragment and used the Krakow suture technique for the distal fragment and patellar tendon [2]. These SA techniques achieved good fixation with fewer complications without the need for implant removal. However, in the studies, the implant failure or non-union rate was reported to be in the range of 7.6–12% [6, 11]. Despite the satisfactory reduction of fracture using SA fixations, SA may be insufficient or not strong enough to withstand the tensile force on the fracture by the quadriceps tendon. Patella baja has been reported as a potential postoperative complication of patella fractures due to patellar tendon shortening [12]. Patella baja can cause limited knee extension and anterior knee pain [13]. Moreover, patella baja is associated with poor functional outcomes in patella interior pole fractures [14]. Post-operative patella baja is reported in 12–57% of patella fractures [12-15]. Park et al. noted that even though significant patella baja was caused by patellar tendon shortening after tightening the patellar tendon using a SA, there were no postoperative complications related to patella baja, such as patellofemoral pain, instability, or extension limitation of the knee joint [16]. To overcome the pitfalls of SA fixation, the authors describe a novel SA technique: One suture inserted at the center of the distal fragment and two sutures inserted at the medial and lateral sides of the central SA. One end of the three SAs are whip stitched into tendon. The knots of the three SAs are tied proximally and then further strengthened by Figure of 8 configuration. Our proposed technique has several advantages. First, in the case of comminuted patella inferior/superior pole fractures, rigid fixation could be achieved by vertical suturing and tendon grasping using the whip stitch suture technique. Second, when compared to TBW, there were no hardware-related complications such as skin irritation or discomfort. Implant removal was not required. Last but not the least, this technique also uses a smaller incision compared to the conventional suture tunnel repair where the distal patella needs to be exposed to retrieve the sutures whereas in the SA technique, it is only the fracture that needs to be exposed distally. Our novel double-row SA technique provided comparable fixation strength and clinical outcomes with fewer complications in patella fractures.
There are several modalities and techniques available for fixation of patella fracture. However, authors recommend that their described technique of SA fixation for patella fracture can provide good functional outcome and promising results.
Described technique for patella fracture using SAs can restore the extensor mechanism and provide stable knee with good range of movements.
References
- 1.Neumann HS, Winckler S, Strobel M. Long-term results of surgical management of patellar fractures. Unfallchirurg 1993;96:305-10. [Google Scholar]
- 2.Kadar A, Sherman H, Drexler M, Katz E, Steinberg EL. Anchor suture fixation of distal pole fractures of patella: Twenty seven cases and comparison to partial patellectomy. Int Orthop 2016;40:149-54. [Google Scholar]
- 3.Schuett DJ, Hake ME, Mauffrey C, Hammerberg EM, Stahel PF, Hak DJ. Current treatment strategies for patella fractures. Orthopedics 2015;38:377-84. [Google Scholar]
- 4.Yu H, Dong H, Ruan B, Xu X, Wang Y, Hu L. Clinical effect of suture anchor and double-pulley technique in the treatment of inferior patellar fracture. Comput Math Methods Med 2021;2021:4964195. [Google Scholar]
- 5.Cho JH. Percutaneous cannulated screws with tension band wiring technique in patella fractures. Knee Surg Relat Res 2013;25:215-9. [Google Scholar]
- 6.Chang CH, Chuang HC, Su WR, Kuan FC, Hong CK, Hsu KL. Fracture of the inferior pole of the patella: Tension band wiring versus transosseous reattachment. J Orthop Surg Res 2021;16:365. [Google Scholar]
- 7.Lee KW, Ma SB, Yang DS, Oh SH, Park SH. Open reduction and internal fixation using multiple nonabsorbable suture materials in acute patella fracture: Comparison of clinical and radiological outcome with tension band wiring. Knee Surg Relat Res 2021;33:34. [Google Scholar]
- 8.Anand A, Kumar M, Kodikal G. Role of suture anchors in management of fractures of inferior pole of patella. Indian J Orthop 2010;44:333-5. [Google Scholar]
- 9.Patel VR, Parks BG, Wang Y, Ebert FR, Jinnah RH. Fixation of patella fractures with braided polyester suture: A biomechanical study. Injury 2000;31:1-6. [Google Scholar]
- 10.Kim KS, Suh DW, Park SE, Ji JH, Han YH, Kim JH. Suture anchor fixation of comminuted inferior pole patella fracture-novel technique: Suture bridge anchor fixation technique. Arch Orthop Trauma Surg 2021;141:1889-97. [Google Scholar]
- 11.Egol K, Howard D, Monroy A, Crespo A, Tejwani N, Davidovitch R. Patella fracture fixation with suture and wire: You reap what you sew. Iowa Orthop J 2014;34:63-7. [Google Scholar]
- 12.Mariani PP, Del Signore S, Perugia L. Early development of patella infera after knee fractures. Knee Surg Sports Traumatol Arthrosc 1994;2:166-9. [Google Scholar]
- 13.Lancourt JE, Cristini JA. Patella alta and patella infera. Their etiological role in patellar dislocation, chondromalacia, and apophysitis of the tibial tubercle. J Bone Joint Surg Am 1975;57:1112-5. [Google Scholar]
- 14.Veselko M, Kastelec M. Inferior patellar pole avulsion fractures: Osteosynthesis compared with pole resection. Surgical technique. J Bone Joint Surg Am 2005;87 Suppl 1:113-21. [Google Scholar]
- 15.Lazaro LE, Wellman DS, Sauro G, Pardee NC, Berkes MB, Little MT, et al. Outcomes after operative fixation of complete articular patellar fractures: Assessment of functional impairment. J Bone Joint Surg Am 2013;95:e961-8. [Google Scholar]
- 16.Park YG, Choi S, Kim BS, Lee SJ, Kim DY, Lim C. Tension band wiring versus suture anchor technique in patellar inferior pole fracture: Novel double row suture anchor technique. Ann Med Surg (Lond) 2022;84:104822. [Google Scholar]





