
Spinal cord decompression with occipitocervical fusion is the keystone of atlanto-occipital assimilation management.
Dr. Kaman Kuity, Department of Orthopaedic Surgery, Dr. D.Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune - 411 018, Maharashtra, India. E-mail: Kamaniimsar11@gmail.com
Introduction: Atlanto-occipital assimilation is the most common osseous anomaly of the cervical-occipital junction. The incidence rate of occipitalization has been reported 1.42.5/1000 children. Most of the patients are asymptomatic initially. Clinical features usually appear after 3rd decade depending on the level and degree of spinal cord compression with surrounding vital structures such as vertebral artery involvement. Hence, early definitive diagnosis and subsequent successful treatment are necessary in such cases to prevent life-threatening complications.
Case Report: A 16-year-old male presented with neck pain and progressive weakness of the bilateral lower limb since the past 2 months suffering from difficulty in walking, giddiness, and numbness of his fingertips.Hoffman’s sign was positive. Plain cervical spine radiography (AP and lateral) is falsely suggestive of the absence of an atlas. MRI revealed the tip of the dens projecting 1314 mm above the Chamberlains line suggestive of basilar invagination. Occipito-cervical fixation was planned with an occipital plate, laminar, pedicle screw, and rods. Occipital plate fixed with screws (6,8 mm). C2 vertebra fixation with pedicle screw and laminar screws and C3 vertebra with a lateral mass screw under C-arm guidance.The patient mobilized with a walker from post-operative day 2 and then he ambulated unaided.
Conclusion: Different types of atlanto-occipital assimilation have been reported. Treatment modality completely depends on neurological symptoms and instability.Although, different surgical options are available, occipito-cervical fixation with occipital plate, screws, and rod fixation is the most superior surgical technique for atlanto-occipital assimilation with atlanto-occipital instability.
Keywords: Atlanto-occipital assimilation, basilar invagination, occipito-cervical fixation.
Atlanto-occipital assimilation is one of the most common osseous anomalies of the cervical-occipital junction [1]. Atlas assimilation defined as a congenital fusion of atlas with occiput and basilar invagination is prolapse of odontoid into the foramen magnum. Atlanto-occipital assimilation may be complete or partial based on the area of atlas and occipital fusion [2].The incidence rate of occipitalization has been reported 1.42.5/1000 children. It may associated with other osseous anomalies of the craniovertebral junction, occipital condylar hypoplasia, atlas hypoplasia, and incomplete C1 ring with spreading of lateral mass [3]. Most of the patients are asymptomatic initially. clinical features usually appear after 3rd decade of life because the spinal cord and vertebral arteries are less resistant to compression at an older age. Features of the disease depend on the level and degree of spinal cord compression [4]. Anterior spinal cord compression causes muscle weakness, ataxia, wasting, and spasticity. Posterior cord impingement causes loss of light touch, proprioception, and deep pain. Involvement of the vertebral artery leads to vertigo,giddiness, and unsteady gait [5]. Hence, early definitive diagnosis and subsequent successful treatment are necessary in such cases to prevent life-threatening complications. The following case report describes the unique earlier presentation of atlantooccipital assimilation with atlanto-occipital instability and the most superior modality of treatment in such cases by occipito-cervical fusion utilizing occipital plates, screws, and rods.
A 16-year-old male presented with neck pain and progressive weakness of the bilateral lower limb since the past 2 months. The pain was sudden onset, dull aching in character, and radiating toward both the shoulder and occipital region of the head. He was also suffering from difficulty in walking, giddiness, and numbness in his fingertips. No history of bowel and bladder involvement. Hoffman sign was positive and the supinator reflex was inverted. There had been no history of recent trauma before the onset of symptoms, and no history of any constitutional symptoms.
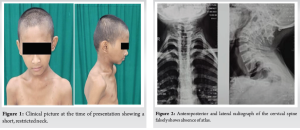
On general examination low set of hairline, short neck, and restricted neck movement (Fig. 1). His cranial nerve function was normal. Lower limb muscles (hip flexors, knee extensors, extensor hallucis longus, and flexor hallucis longus) power was MRC grade 4, and upper limbmuscles power was normal (MRC grade 5). Deep tendonreflexes were exaggerated with patellar and ankle clonus. Babinski’s sign was positive. The sensation had been preserved.
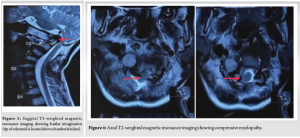
Plain cervical spine radiography (AP and lateral) is falsely suggestive of the absence of an atlas (Fig. 2).
MRI revealed tip of the dens projecting 1314 mm above the Chamberlains line suggestive of basilar invagination (Fig. 3).
The foramen magnum was narrowed (approximately 7.5 mm) (Fig. 4).
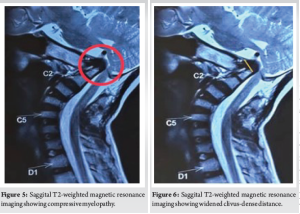
Tip of dense displaced posteriorly and compressing cervical medullary junction. The anterior arch of the atlas is not well visualized, suggestive of aphasia and posterior arch is hypo-plastic (Fig. 5).
Increase clivus-dense distance (56 mm)-suggestive of dislocation (Fig. 6).
Occipito-cervical fixation was planned after a pre-anesthetic check-up under image intensifier guidance. The procedure was done in a prone position under general anesthesia. A 5 cm vertical incision over posterior aspect of the neck and base of the skull under strict aseptic condition. After soft-tissue dissection and semispinalis capitis retraction C1, C2, and C3 spinous process and base of the skull are exposed. C2 fixation with 3.5 mm pedicle screw (24 mm), laminar screw (26 mm), and C1 with 3.5 mm lateral mass screw (28 mm) under C-arm guidance.The occipital plate was fixed with five screws (68 mm) after identifying following landmarks external occipital protuberancesuperior nuchal line, foramen magnum, and ensuring that the plate is flush with the skull. Decompression was done by excision of posterior arch of C1. Extra precaution was taken during occipital drilling and the drill guide was set at 8 mm. Occipital plate, C2, and C3 screws were connected with pre-bending rods (Fig. 7 and 8).

Bone graft is placed against decorticated dorsal element of the spine by local bone. Routine closure in layers and antiseptic dressing were done. Neck immobilized with hard cervical collar for 2 months. Postoperatively neurological symptoms and instability disappear after 1 month.

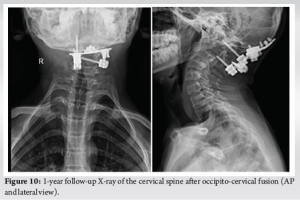
The patient mobilized with a walker from post-operative day 2 and then he ambulated unaided (Fig. 9). Gradually he started daily living activities with no complications at 1-year follow-up (Fig. 10).
Atlanto-occipital fusion occurs due to the failure of segmentation between the 4th occipital sclerotome and 1st cervical sclerotome in embryonic period [6]. The incidence of atlanto-occipital assimilation has been reported to be 0.08 to 3% of general population where males and females are equally affected [7]. Patients with atlas occipitalization often present with neurological symptoms after patients are associated with low hairlines, short necks, and restricted neck movement [8]. The position of odontoid is one of the keys to neurological features. When the odontoid lies above the foramen magnum, basilar invagination is present, and when lies below foramen magnum, the patient is generally asymptomatic. If basilar invagination remains untreated symptoms progressively worsen and it may lead to death. Symptoms of this condition may vary from a simple headache to myelopathic symptoms such as limb weakness, giddiness, numbness and mimic with spinal infection, spinal tumors, etc. It is very challenging to diagnose and manage such cases to prevent morbid conditions. A routine radiograph is not useful for atlanto-occipital assimilation determination. CT scan and MRI have a great role to diagnose cranio-vertebral anomalies. Radiological diagnosis of basilar invagination is based on Chamberlain’s line, McGregor line, and Fischgold’s line [9,10]. Treatment of atlanto-occipital fusion based on degree of cord compression. Atlanto-occipital assimilation without cervical cord compression is conservatively treated with cervical interferential therapy, rigid cervical orthosis, hard cervical collar, and Miami-j collar [11]. A variety of operative techniques are available for atlanto-occipital assimilation with basilar invagination such as occipital wiring, hook fixation, and occipito-cervical fusion with occipital plate, screws, and rods. Rarely, patients with neurological symptoms by minor spinal cord compression without instability are treated with simple decompression by laminectomy.The extent of laminectomy as small as possible because wide laminectomy may lead to post-operative instability [12]. Jain et al. described the techniques of drilling the occipital bone close to the foramen magnum and forming an artificial arch of the atlas, which is used for fixation [13]. Occipito cervical fixation was first described by Pincher in 1910 [14]. Few studies reported good clinical and radiological outcomes with sufficient correction of deformity and high fusion rate achieved through occipito-cervical fusion by utilizing plate, screw, and rods in osseous anomalies at craniocervical junction [15, 16]. Among the all surgical techniques occipito-cervical fusion utilizing occipital plate, screws, and rod fixation is the most effective treatment modality in atlanto-occipital assimilation with instability and myelopathic symptoms due to cord compression. It provides rigid fixation of occipito-cervical region. Hence, prolong post-operative immobilization is not required. The patient had a complete recovery from the pre-operative symptoms such as numbness of fingers and giddiness with no complications in a follow-up of 1 year. Occipito-cervical fusion looks like the most reliable management of atlanto-occipital assimilation with no major complications and good functional outcomes.
Different types of atlanto-occipital assimilation have been reported. Most of the patients are asymptomatic till adulthood, but some show neurological symptoms earlier. Treatment modality completely depends on neurological symptoms and instability. Although, different surgical options are available but decompression of the spinal cord with occipito-cervical fusion utilizing occipital plate, screws, and rod fixation is the most superior surgical technique for atlanto-occipital assimilation with atlanto-occipital instability.
Atlanto occipital assimilation should always be a differential diagnosis of cervical myelopathy in young patients. Decompression of the spinal cord with a combination of occipito-cervical fusion provides good functional outcomes and excellent prognosis in such cases.
References
- 1.Lang J. Skull Base and Related Structures. Atlas of Clinical Anatomy. New York: Shattauer, Stutgart; 1995. p. 54. [Google Scholar]
- 2.Hensinger RN. Congenital anomalies of the cervical spine. Clin Orthop Relat Res 1991;264:16-38. [Google Scholar]
- 3.Smith JS, Shaffrey CI, Abel MF, Menezes AH. Basilar invagination. Neurosurgery 2010;66:A39-47. [Google Scholar]
- 4.Kim HJ. Cervical anomalies in children and adolescents. Curr Opin Pediatr 2013;25:72-7. [Google Scholar]
- 5.Hensinger RN. Osseous anomalies of the craniovertebral junction. Spine (Phila Pa 1976) 1986 11:323-33. [Google Scholar]
- 6.Tsou PM, Yau A, Hodgson AR. Embryogenesis and prenatal development of congenital vertebral anomalies and their classification. Clin Orthop Relat Res 1980;152:211-31. [Google Scholar]
- 7.Martellacci S, Ben Salem D, Méjean N, Sautreaux JL, Krausé D. A case of foramen magnum syndrome caused by atlanto-occipital assimilation with intracanal fibrosis. Surg Radiol Anat 2008;30:149-52. [Google Scholar]
- 8.Spillane JD, Pallis C, Jones AM. Developmental abnormalities in the region of the foramen magnum. Brain 1957;80:11-48. [Google Scholar]
- 9.Smoker WR, Khanna G. Imaging the craniocervical junction. Childs Nerv Syst 2008;24:1123-45. [Google Scholar]
- 10.McGregor M. The significance of certain measurements of the skull in the diagnosis of basilar impression. Br J Radiol 1948;21:171-81. [Google Scholar]
- 11.Electricwala AJ, Harsule A, Chavan V, Electricwala JT. Complete Atlantooccipital assimilation with basilar invagination and atlantoaxial subluxation treated non-surgically: A case report. Cureus 2017;9:e1327. [Google Scholar]
- 12.Jain VK, Takayasu M, Singh S, Chharbra DK, Sugita K. Occipital-axis posterior wiring and fusion for atlantoaxial dislocation associated with occipitalization of atlas: Technical note. J Neurosurg 1993;79:142-4. [Google Scholar]
- 13.Kim KR, Lee YM, Kim YZ, Cho YW, Kim JS, Kim JH, et al. Cervical myelopathy secondary to atlanto-occipital assimilation: The usefulness of the simple decompression surgery. Korean J Spine 2013;10:189-91. [Google Scholar]
- 14.Pilcher LS. V. Atlo‐ axoid fracture-dislocation. Ann Surg 1910;51:208-11. [Google Scholar]
- 15.Abumi K, Takada T, Shono Y, Kaneda K, Fujiya M. Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine (Phila Pa 1976) 1999;24:1425-34. [Google Scholar]
- 16.Ding X, Abumi K, Ito M, Sudo H, Takahata M, Nagahama K, et al. A retrospective study of congenital osseous anomalies at the craniocervical junction treated by occipitocervical plate-rod systems. Eur Spine J 2012;21:1580-9. [Google Scholar]





