
A combined transfer of the middle trapezius tendon (MTT) and lower trapezius tendon (LTT), along with a split Achilles tendon allograft, could be another alternative treatment to address posterior superior irreparable rotator cuff tears without arthritis
Dr. Chang Hee Baek, Department of Orthopaedic Surgery, Yeosu Baek Hospital, Jeollanam-Do, Republic of Korea. E-mail: yeosubaek@gmail.com
Abstract
Introduction: Irreparable rotator cuff tears (IRCTs) often deteriorate shoulder function, necessitating careful consideration of treatment approaches. While reverse total shoulder arthroplasty (RTSA) is the first line of treatment in patients with arthropathy, preserving the joint is crucial for highly demand patients without arthritis. For those patients, various tendon transfer techniques have been established to address different types of IRCTs, including lower trapezius tendon (LTT) transfer for posterior superior IRCTs (PSIRCTs) and middle trapezius tendon (MTT) transfer for isolated supraspinatus IRCTs (ISIRCTs).
Case Report: A 66-year-old male with persistent right shoulder pain and weakness for 2 years, diagnosed with PSIRCTs, sought an alternative to RTSA due to occupational concerns as a restaurant owner. Preoperatively, patients showed limited range of motion (ROM) and weakness, especially in forward elevation (FE) and external rotation (ER). Radiography and magnetic resonance imaging (MRI) scan indicated superior humeral head translation without advanced arthritis and concurrent tears in the supraspinatus and infraspinatus with atrophy. After the consultation, patients underwent a combined transfer of LTT and MTT with a split Achilles tendon allograft in Y-configuration. By post-operative 1 year, the patient exhibited notable improvement, including reduced pain (VAS 4–2), enhanced function (ASES 50–83, Constant 42–78), and increased ROM (FE, 120°–160° and ER, 10°–40°). Radiographic assessments demonstrated an increased in acromiohumeral distance without arthritic progression. Post-operative MRI confirmed tendon integrity, and the patient successfully resumed work at 6 months.
Conclusion: A combined transfer of the MTT and LTT with a split Achilles tendon allograft in Y-configuration has been shown to alleviate pain, enhance functional scores, and improve the ROM in patients with PSIRCTs without arthritis.
Keywords: Lower trapezius tendon transfer, middle trapezius tendon transfer, irreparable rotator cuff tear, joint preserving, tendon transfer.
Irreparable rotator cuff tears (IRCTs) can significantly impact shoulder function on a daily basis. While reverse total shoulder arthroplasty (RTSA) is a successful option, it is crucial to consider joint-preserving procedures, especially for highly demanding and active patients without arthritis. Various tendon transfer techniques have been developed based on the type of IRCTs [1]. Lower trapezius tendon (LTT) transfer has demonstrated promising clinical outcomes for posterior superior IRCTs (PSIRCTs) [2,3], while middle trapezius tendon (MTT) transfer has shown satisfying results for isolated supraspinatus IRCTs (ISIRCTs) [4]. Biomechanically, the line of pull of the LTT closely mimics the physiological line of pull of the native infraspinatus [5]. Furthermore, LTT provides sufficient excursion and tension to effectively substitute for the function of the infraspinatus [5,6]. On the other hand, MTT mimics the supraspinatus vector, and therefore, the MTT transfer aims to biomechanically reconstruct the supraspinatus by relocating MTT attached with an interpositional graft from the medial half of the scapular spine to the supraspinatus footprint [4,7]. Given that a PSIRCTs involves irreparable tears of both the supraspinatus and infraspinatus, the combined transfer of both MTT and LTT may allow for the emulation of both supraspinatus and infraspinatus. In this report, we present a case of a 66-year-old male patient with PSIRCTs but without arthritis who underwent combined MTT and LTT with a split Achilles tendon allograft in a Y-configuration.
A 66-year-old right-handed male patient has been admitted to our hospital, reporting persistent pain (Visual Analog Score [VAS] 5) and weakness in his right shoulder for 2 years, without any associated trauma. Before visit at our hospital, he had visited another hospital where the recommendation for RTSA was made due to IRCTs. Clinical evaluation revealed active forward elevation (FE) of 120°, abduction (ABD) of 90°, external rotation at side (ERS) of 10°, and internal rotation (IR) to the back at the level of T7 (Fig. 1a and b).
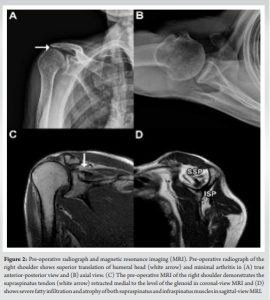
Pain and functional assessment scores specific to the shoulder indicated dissatisfaction, with a Constant score of 42/100 and an American Shoulder and Elbow Surgeons (ASES) score of 50/100. Standard radiography showed superior translation of the humeral head, with no signs of advanced arthritis (Fig. 2a and b). The magnetic resonance imaging (MRI) scan showed PSIRCTs with advanced atrophy and high-grade fatty infiltration (Fig. 2c and d). Given his occupation as a self-employed restaurant owner, he expressed reluctance toward undergoing RTSA and was actively seeking alternative treatment options. The patient had chosen to undergo a tendon transfer procedure, a combined transfer of LTT and MTT with a single split Achilles tendon allograft in Y-configuration.
Surgical procedure
The patient was positioned in the lateral decubitus position and administered general anesthesia. Arthroscopic interventions, involving the rotator interval and capsule release, and acromioplasty were performed. After debriding any non-feasible tissues of torn rotator cuffs (Fig. 3a), two triple-loaded medial-row anchors (5.5-mm Healicoil, Smith and Nephew, Andover, MA, USA) were placed in the supraspinatus footprint.
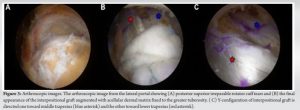
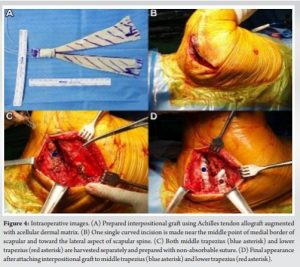
For interpositional graft, an Achilles tendon allograft was augmented with an acellular dermal matrix (ADM) graft to provide a spacer effect, ensure high tensile strength, and promote strong suture retention (Fig. 4a). The graft was split approximately 6 cm from one end, forming a “Y”-shaped configuration. To harvest the MTT and LTT, a curved incision was made from the lateral scapular spine to the middle medial border of the scapula (Fig. 4b). After meticulous dissection, the MTT was detached from the insertion site of the medial half of the scapular spine to the lateral scapular border and the acromion attachment site. The LTT was similarly detached from the scapular spine after meticulous dissection and release of the deep fascia. Both harvested MTT and LTT were sutured with No. 2 non-absorbable sutures in a continuous locking suture (Fig. 4c). Subsequently, small incisions were made in both the supraspinatus fascia and infraspinatus fascia for the graft’s passageway. Using a long curved clamp, the graft was delivered into the subacromial space. Two suture limbs from the medial-row anchor were threaded through the remaining posterior cuff muscle for a side-to-side suture with the graft, while the remaining limbs were threaded through the graft. Secure fixation of the graft was achieved with three knotless lateral-row anchors (4.75-mm Swivelock anchors, Arthrex, Naples, FL, USA) using a suture bridge technique. Finally, each end of the Y-configuration of the graft (Fig. 3b and c) was attached to the MTT and LTT, with the patient’s arm placed in maximum external rotation at a 60° abduction angle (Fig. 4d).
Post-operative rehabilitation protocol
Patients wore an abduction brace for the initial 4 weeks followed by active-assisted range of motion (ROM) exercises after brace discontinuation at 4 weeks. Strengthening exercises in all directions begun at 3-month postoperatively. However, heavy labor work and sports were strictly prohibited until 6-month postoperatively to ensure proper healing.
Post-operative 1-year clinical outcome
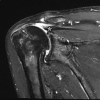
The patient underwent follow-up at post-operative intervals of 1, 3, 6 months, and 1 year. At the 1-year mark, the patient experienced reduced pain (VAS score 2) and demonstrated improved function with Constant score of 78/100 and ASES score of 83/100. Shoulder ROM increased: FE to 170°, ABD to 140°, and ERS to 40° (Fig. 1c and d). IR at back has slightly decreased to T10. Acromiohumeral distance (AHD) increased from 5.2 mm to 8.1 mm without signs of arthritic progression (Fig. 5a). A 1-year post-operative MRI scan showed no evidence of re-tear in the transferred tendon (Fig. 5b, c, d), and there were no infection and nerve-related complication. The patient successfully returned to work at his restaurant at the 6-month post-operative mark and has continued working since.

The present case report is the first to detail the outcomes of a single patient who underwent a combined transfer of MTT and LTT with split Achilles tendon allograft. The patient experienced pain relief, enhanced ROM, and no further arthritic progression. Remarkably, 6-months postoperatively, the patient returned to work with no significant complications. Various surgical options have been proposed for IRCTs without arthropathy, such as rotator cuff debridement, partial rotator cuff repair with or without patch augmentation, balloon procedures, biceps tenotomy or tenodesis, and tendon transfers [8,9]. The RTSA can also be considered, but concerns exist regarding its longevity in younger, more active patients. Tendon transfers emerge as a potentially more viable option for pain reduction and improved function, especially for highly active patients without arthropathy. Tendon transfer, particularly in LTT and MTT transfer, has been indicated in patients who (1) do not respond to conservative treatment, (2) have irreparable tears in the supraspinatus (for MTT transfer) and infraspinatus (for LTT transfer), (3) exhibit poor muscle quality in the posterior supraspinatus (for MTT transfer) and infraspinatus (for LTT transfer) with Goutallier grade ≥3, and (4) have minimal to mild glenohumeral arthritis with Hamada grade ≤2. LTT transfer has proven effective in alleviating pain and enhancing shoulder ROM, especially in external rotation, for patients with PSIRCTs [2,10,11,12]. In our previous paper involving 36 patients treated with LTT transfer, pain relief and shoulder function scores were effectively maintained even at the mid-term duration (mean follow-up of 58.2 months) [11]. While short-term clinical studies [12,13] have reported no significant arthritis progression following LTT transfer, mid-term studies [2,11] have shown arthritis progression over time, with an increase in AHD and a decrease in Hamada grade. This suggests that a single transfer of LTT may not be sufficient to prevent superior humeral migration and long-term arthritis progression. Nonetheless, our clinical experience of MTT transfer in cases of ISIRCTs yielded promising outcomes with the prevention of superior humeral migration [4]. This procedure aimed to reconstruct the irreparable supraspinatus and to provide a spacer effect in subacromial space, contributing to the dynamic stability of the glenohumeral joint [7].
There have been several successful reports that involve a combination of two procedures to address IRCTs. For instance, there have been reports of successful combinations of LTT transfer with superior capsular reconstruction [14] and LTT transfer with biceps superior capsule reconstruction [15]. In addition, the versatility of RTSA is demonstrated in its combination with l’Episcopo transfer [16]. In addition, a novel procedure suggests combining Latissimus dorsi transfer with a Subacromial Balloon Spacer to restore shoulder external rotational coupling, optimize deltoid loading, center the humeral head, and protect the transferred tendon from subacromial compression stresses [17]. In the current case report, we combined the transfer of LTT with MTT with a single split Achilles tendon allograft. The patient exhibited improvement in both pain and ROM without signs of arthritis by post-operative 1 year. We believe that the observed improvement in clinical scores can be attributed to the replacement of both supraspinatus and infraspinatus irreparable tendon portions by both MTT and LTT with different vectors. The combination of both MTT and LTT transfers may have further enhanced the dynamic stability of the glenohumeral joint, preventing superior migration of the humeral head and halting arthritis progression. In addition, the increased AHD and no further arthritic changes indicate that augmentation of ADM graft might have provided a spacer effect and biologic tuberoplasty effect [18]. However, these findings are based on a single patient and were assessed over a relatively short period of time, so future study is warranted.
The surgical procedure described has several drawbacks. First, it is relatively bulky, and there may be potential issues associated with the Achilles tendon allograft. Second, it is difficult to distinguish the poorly defined anatomy of the trapezius muscle, particularly in differentiating its upper, middle, and lower thirds. Yet, surgeons may benefit from locating the scapular spine, where the upper LTT is found underneath, and the lower part of the MTT is located just above. Third, concerns exist regarding denervation during the splitting of the middle and lower trapezius, given the unclear relationship of the neurovascular pedicle within the muscle belly. However, cadaveric study [5] has shown that the surgical anatomy of LTT transfers offers safe and reliable anatomic relationships. Finally, we acknowledge that determining the true effectiveness of the procedure based on a single case is challenging; therefore, future studies with a larger number of patients and longer follow-up durations are warranted.
A combined transfer of the MTT and LTT with split Achilles tendon graft has been shown to alleviate pain, enhance functional scores, and improve the ROM in patients with PSIRCTs without arthritis. Nevertheless, it is important to note that the current report is based on the clinical outcome of a single patient. For a more comprehensive understanding, longer-term and broader clinical studies involving a larger number of patients are necessary to establish the efficacy and durability of this procedure.
A combined transfer of the middle trapezius tendon (MTT) and lower trapezius tendon (LTT), with a split Achilles tendon allograft could be another alternative to address posterior superior irreparable rotator cuff tears.
References
- 1.Li X, Galvin JW, Zalneraitis BH, Gasbarro G, Parada SA, Eichinger JK, et al. Muscle tendon transfers around the shoulder: Diagnosis, treatment, surgical techniques, and outcomes. J Bone Joint Surg Am 2022;104:833-50. [Google Scholar | PubMed]
- 2.Elhassan BT, Wagner ER, Werthel JD. Outcome of lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tear. J Shoulder Elbow Surg 2016;25:1346-53. [Google Scholar | PubMed]
- 3.Clouette J, Leroux T, Shanmugaraj A, Khan M, Gohal C, Veillette C, et al. The lower trapezius transfer: A systematic review of biomechanical data, techniques, and clinical outcomes. J Shoulder Elbow Surg 2020;29:1505-12. [Google Scholar | PubMed]
- 4.Baek CH, Kim JG. Outcomes of arthroscopic-assisted middle trapezius tendon transfer for isolated irreparable supraspinatus tendon tears: Minimum 2-year follow-up. Arch Orthop Trauma Surg 2023;143:2547-56. [Google Scholar | PubMed]
- 5.Omid R, Lee B. Tendon transfers for irreparable rotator cuff tears. J Am Acad Orthop Surg 2013;21:492-501. [Google Scholar | PubMed]
- 6.Moraiti K, Zampeli F, Reinares F, Gantsos A, Valenti P. Feasibility of lower trapezius transfer extended by the infraspinatus fascia for restoration of external rotation in irreparable posterosuperior rotator cuff tears: An anatomical study. Eur J Orthop Surg Traumatol 2021;31:661-7. [Google Scholar | PubMed]
- 7.Moroder P, Akgün D, Lacheta L, Thiele K, Minkus M, Maziak N, et al. Middle trapezius transfer for treatment of irreparable supraspinatus tendon tears- anatomical feasibility study. J Exp Orthop 2021;8:5. [Google Scholar | PubMed]
- 8.Kovacevic D, Suriani RJ Jr., Grawe BM, Yian EH, Gilotra MN, Hasan SA, et al. Management of irreparable massive rotator cuff tears: A systematic review and meta-analysis of patient-reported outcomes, reoperation rates, and treatment response. J Shoulder Elbow Surg 2020;29:2459-75. [Google Scholar | PubMed]
- 9.Oh JH, Park MS, Rhee SM. Treatment strategy for irreparable rotator cuff tears. Clin Orthop Surg 2018;10:119-34. [Google Scholar | PubMed]
- 10.Baek CH, Lee DH, Kim JG. Latissimus dorsi transfer vs. lower trapezius transfer for posterosuperior irreparable rotator cuff tears. J Shoulder Elbow Surg 2022;31:1810-22. [Google Scholar | PubMed]
- 11.Baek CH, Kim BT, Kim JG, Kim SJ. Midterm outcome of arthroscopic-assisted lower trapezius transfer using an achilles allograft in treatment of posterior superior irreparable rotator cuff tear. J Shoulder Elbow Surg 2023;S1058-2746(23)00738-3. [Google Scholar | PubMed]
- 12.Elhassan BT, Sanchez-Sotelo J, Wagner ER. Outcome of arthroscopically assisted lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tears. J Shoulder Elbow Surg 2020;29:2135-42. [Google Scholar | PubMed]
- 13.Baek CH, Lim C, Kim JG. Superior capsular reconstruction versus lower trapezius transfer for posterosuperior irreparable rotator cuff tears with high-grade fatty infiltration in the infraspinatus. Am J Sports Med 2022;50:1938-47. [Google Scholar | PubMed]
- 14.McCormick JR, Menendez ME, Hodakowski AJ, Garrigues GE. Superior capsule reconstruction and lower trapezius transfer for irreparable posterior-superior rotator cuff tear: A case report. JBJS Case Connect 2022;8:12. [Google Scholar | PubMed]
- 15.Chiu CH, Yang CP, Tang HC, Weng CJ, Hsu KY, Chao-Yu Chen A, et al. Arthroscopic-assisted lower trapezius tendon transfer with autologous semitendinosus tendon and long head of biceps superior capsule reconstruction for massive irreparable posterosuperior rotator cuff tears. Arthrosc Tech 2022;11:e1251-9. [Google Scholar | PubMed]
- 16.Merolla G, Cuoghi F, Athwal GS, Parel I, Filippi MV, Cutti AG, et al. A kinematic and electromyographic comparison of a Grammont-style reverse arthroplasty combined with a l'Episcopo transfer compared to a lateralized humeral component reverse for restoration of active external rotation. Int Orthop 2021;45:2061-9. [Google Scholar | PubMed]
- 17.Velasquez Garcia A, Osorio Valdivia P, Brito Ayet C, Mendez M. Latissimus dorsi transfer combined with subacromial balloon spacer for bidirectional rotator cuff deficiency. Arthrosc Tech 2022;11:e2327-35. [Google Scholar | PubMed]
- 18.Mirzayan R. Preliminary outcomes of arthroscopic biologic tuberoplasty in the treatment of massive irreparable rotator cuff tears. Cureus 2023;15:e34402. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Dual Reconstruction, Combined Anterior Latissimus Dorsi with Teres Major and Middle Trapezius Tendon Transfer, Reduces Anterior Superior Humeral Subluxation: Case Report
January 1, 2026 Dual Reconstruction, Combined Anterior Latissimus Dorsi with Teres Major and Middle Trapezius Tendon Transfer, Reduces Anterior Superior Humeral Subluxation: Case Report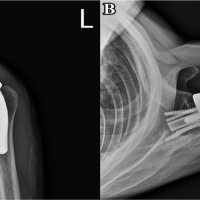 June 10, 2024 Pectoralis Major Transfer For Anterior Recurrent Dislocation of Reverse Total Shoulder Arthroplasty: A Case Report
June 10, 2024 Pectoralis Major Transfer For Anterior Recurrent Dislocation of Reverse Total Shoulder Arthroplasty: A Case Report April 10, 2023 Treating Little Finger’s Flexor Profundus Tendon Rupture after Percutaneous K-wire Fixation of a Bennet Fracture – A Case Report
April 10, 2023 Treating Little Finger’s Flexor Profundus Tendon Rupture after Percutaneous K-wire Fixation of a Bennet Fracture – A Case Report March 1, 2026 Traumatic Tibialis Anterior Muscle Herniation with a Large Fascial Defect Managed by Prolene Mesh Repair: A Rare Case Report
March 1, 2026 Traumatic Tibialis Anterior Muscle Herniation with a Large Fascial Defect Managed by Prolene Mesh Repair: A Rare Case Report