
Orthopaedic surgeons should be aware of ACL with MPFL injury patterns and they should be addressed simultaneously followed with aggressive physiotherapy.
Dr. Raj Kumar, Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi, India. E-mail: rajkumargautam122gmail.com
Abstract
Introduction: The study discussed three patients who experienced both anterior cruciate ligament (ACL) injury and patellofemoral instability. This combination of injuries is rare and has a scarcity of published /literature. The study described the mechanism of injury, diagnostic modalities, and the decision-making process for surgical intervention. It emphasizes the importance of a comprehensive clinical evaluation and discusses surgical techniques for combined ACL and medial patellofemoral ligament (MPFL) reconstruction. The study suggests that with careful evaluation and meticulous surgical techniques, patients with concurrent ACL and MPFL injuries can achieve successful outcomes and return to normal activities.
Case Report: The cases presented involve young patients who suffered twisting knee injuries, often resulting from accidents or sporting activities. The surgical technique involved the use of grafts for ACL and MPFL reconstruction. MPFL reconstruction was performed followed by ACL reconstruction. Post-operative rehabilitation included the use of a patellar stabilizing knee brace and gradual mobilization.
Results: The patients experienced moderate pain initially but achieved a full range of motion and stability in the knee after several weeks. At the 1-year follow-up, both patients reported no symptoms of instability or pain.
Conclusion: The article highlights the importance of MPFL reconstruction in preventing ACL reconstruction failures and emphasizes the need for aggressive rehabilitation to prevent knee stiffness. Overall, this study presented important information and added knowledge regarding the diagnosis, surgical management, and post-operative care of patients with concurrent ACL and patellofemoral instability.
Keywords: Anterior cruciate ligament, medial patellofemoral ligament, patellofemoral instability, combined instability, concurrent reconstruction, rehabilitation.
The coexistence of anterior cruciate ligament (ACL) injury and patellofemoral instability presents a complex orthopedics challenge that has limited attention in the medical literature. While ACL and patellofemoral injuries are individually well-documented, their simultaneous occurrence is a relatively rare phenomenon [1-4]. To date, few studies have explored the combined reconstruction of the ACL and the medial patellofemoral ligament (MPFL), highlighting the scarcity of available literature. In this context, this article presents three cases where patients sustained both ACL and MPFL injuries following injury to their affected legs. The mechanism of injury, diagnostic modalities, and the decision-making process for surgical intervention are discussed. These rare combinations of injuries should be kept in mind and emphasize the importance of a comprehensive clinical evaluation [2-4]. Furthermore, the article described surgical techniques for combined ACL and MPFL reconstruction. It outlined the choice of grafts and the sequence of reconstruction. Moreover, the study emphasized the significance of the MPFL in preventing ACL reconstruction failures. The promising outcomes reported in the studies suggested that with careful evaluation and meticulous surgical techniques, patients with concurrent ACL and MPFL injuries can achieve a successful return to normal activities.
dThe study consisted of three patients managed with simultaneous ACL and MPFL reconstruction with similar surgical techniques. The patients underwent postoperative rehabilitation and follow-up for at least 1 year with assessment using Kujala scores.
Case 1
A 19-year-old female presented to our outpatient department with complaints of right patellar instability, knee pain, and instability. The patient suffered a road traffic accident 6 months back involving a twisting knee injury followed by a fall on the knee. There was no previous history of knee pain or dislocation. On clinical examination, the Lachman test was positive, and the grade II anterior drawer test, Grade I pivot shift test, and patellar apprehension test were positive. On performing the patellar quadrant test, the patella was subluxated to the 4th quadrant with apprehension and pain. The range of motion was full but with apprehension for patellar subluxation. The collateral ligament test was negative with no joint line tenderness. The radiographs depicted normal knee joint alignment with a superomedial rim fracture of the patella (Fig. 1).

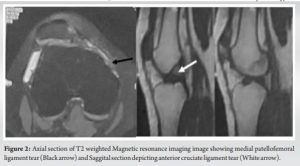
Magnetic resonance imaging (MRI) scans showed a complete ACL tear with MPFL tear from femoral attachment with waviness of the fibers (Fig. 2). Beighton’s score was normal. The patient underwent arthroscopic ACL reconstruction with mini-open MPFL reconstruction.
Case 2
A 23-year-old male presented to the outpatient department after 1.5 years of a knee injury while playing soccer. The gentleman suffered a twisting knee injury followed by knee pain, knee instability, and dislocation of the patella. There were no previous radiographs or other imaging available. The patient was initially managed with an above-knee slab for 4–6 weeks followed by rehabilitation. Since then the patient was not able to return to sports, had two episodes of patella dislocation due to trivial knee jerks and knee pain. On clinical examination, the Grade III anterior drawer Grade II pivot test, patellar apprehension test, and patellar quadrant test (subluxated to the 4th quadrant) were positive. The terminal range of motion was restricted and painful. The radiographs depicted no bony abnormality with normal bone alignment. The computer tomogram depicted normal tibial tuberosity trochlear groove distance with no trochlear dysplasia. The MRI scan depicted a complete ACL tear with MPFL tear with Grade 2 lateral meniscus tear. The patient was managed with arthroscopic ACL reconstruction with mini-open MPFL reconstruction.
Case 3
A 21-year-old male presented to our outpatient department with complaints of right knee pain and a history of patellar dislocation. The patient suffered the injury while playing football 1 month back. The patient had patellar dislocation on the day of injury, which was reduced by the physiotherapist on the field. The patient was initially managed conservatively with a long knee brace but had two more episodes of patellar dislocation without any inciting event. On clinical examination, the Lachman test was positive, and the Grade II anterior drawer test, Grade II pivot shift test, and patellar apprehension test were positive. On performing the patellar quadrant test, the patella was subluxation to the fourth quadrant with apprehension and pain with J sign positive. The collateral ligament test was negative with no joint line tenderness. The radiographs depicted normal knee joint alignment with no fractures. MRI scans showed a complete ACL tear with an MPFL tear. The patient underwent arthroscopic ACL reconstruction with mini-open MPFL reconstruction.
The patients were surgically managed under spinal epidural anesthesia. Examination under anesthesia was performed for the Lachman test, anterior drawer test, pivot shift test, and lateral patellar translation. An arthroscopic examination was then performed using standard anteromedial and anterolateral portals. The arthroscopic surgery was performed under the tourniquet with a duration of around 90 min. The lateral subluxation of the patella and ACL tear was reconfirmed through diagnostic arthroscopy. Gracilis and semitendinosus grafts were harvested from the ipsilateral proximal tibia. Gracilis tendon was measured (6 mm × 110 mm) and prepared for MPFL reconstruction. Peroneus longus was also kept as an option for ACL reconstruction in case of attenuated tendon. The Semitendinosus tendon was prepared for ACL reconstruction. In one patient, the . Arthroscopic knee debridement and removal of cartilage frills were performed followed by creating appropriate femoral and tibia tunnels for ACL reconstruction using out-in technique. The tunnels were reamed according to the length and diameter of the graft. An incision measuring 2–3 cm was given at the supero-medial border of the patella. Under fluoroscopic guidance, two trans-osseous 4.5 mm tunnels were prepared for SwiveLock. The two ends of the gracilis graft with SwiveLock anchors were placed in the tunnels. The isometric point of the femur was marked with the help of an MPFL template. The graft was passed between layers 2 and 3 of the medial aspect of the knee (Fig. 3). The femoral tunnel at the isometric point was created using a 5-mm reamer considering the size of the loop of the gracilis graft tendon. Caution was taken not to disrupt the femoral tunnel for ACL reconstruction. A nitinol guide wire was placed in the ACL femoral tunnel while creating the femoral tunnel for MPFL reconstruction. The loop of the gracilis graft was passed through the 5-mm femoral tunnel and fixed with a 6 × 23 mm interference screw (Fig. 4).
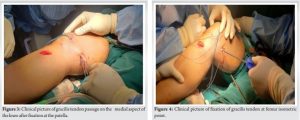
The tensioning of the graft was performed in 30 degrees of knee flexion to prevent over-tensioning. The patellar laxity and tracking were checked throughout the range of motion of the knee before the final tensioning of the graft. Afterward, the prepared graft for ACL was passed through the femoral tunnel and fixed using the suspensory fixation (endobutton) whereas fixed at the tibial end with the help of a 9 × 25 mm interference screw (Fig. 5). The ACL ligament tensioning was performed at full extension position.
Post-operative rehabilitation
A post-operative patellar stabilizing knee brace was applied. Radiographs depicted the appropriate position of tunnels and well-aligned patella (Fig. 6). Both patients experienced moderate pain (VAS 5–7) for the next 3 days. Partial weight mobilization was started from post-operative day 1. Whereas knee bending was allowed after post-operative day 3 considering the intensity of the pain. A patellar stabilizing brace was used during the rehabilitation in both patients for the next 6 weeks. Full weight-bearing mobilization and 0–90 degrees knee bending was achieved in 4 weeks. At the follow-up of 3 months, all the patients had stable and pain-free knees with nearly full range of motion. At the follow-up of 1 year, all patients performed all the activities with no symptoms of instability or pain. The Kujala score at the end of the 1-year follow-up was 89, 91, and 91 respectively.

The occurrence of concomitant ACL with patellofemoral instability is an uncommon phenomenon. There are few articles describing the injury pattern and surgical management. There is even less literature describing the concurrent surgical reconstruction of ACL and MPFL [1-3]. Our case series reported three patients suffering from this injury pattern and treated with simultaneous ACL and MPFL reconstruction with good results. The mechanism of injury is yet not fully understood but includes valgus and external rotation injury [4]. Similar to previously published articles, the patients in our series suffered road traffic accidents with similar injury forces. Such injuries were suffered by young patients similar to the previous published literature. The MPFL is the main structure stabilizing the patella against lateral dislocation. Its function is most important in 0° to 30° of flexion [5,6]. The study by Shankar et al. [1] reported three patients with concurrent MPFL and ACL reconstruction. Two patients in that series had MRI evidence of ACL and MPFL ligament whereas one patient had ACL injury with CT and clinical suspicion of patellar instability. All the patients were managed with concurrent MPFL and ACL reconstruction. They utilized hamstring tendons for the reconstruction. An unstable patella is almost invariably a consequence of dislocation and laxity of the MPFL [7-9]. In the previous study by Macura and Veselko [2], two patients were operated on for simultaneous ACL and MPFL reconstruction using the quadriceps tendon. The deeper portion of the quadriceps tendon was used for MPFL reconstruction whereas the superficial portion was utilized for ACL reconstruction. Schöttle et al. [10] and Deie et al. [11] introduced reconstruction of MPFL with hamstring grafts. In this series, ACL reconstruction was performed followed by MPFL reconstruction. Modified MPFL reconstruction with a quadriceps tendon graft described by Steensen et al. [12]. In our case series, we utilized the semitendinosus tendon for ACL reconstruction and the gracilis tendon for MPFL reconstruction. However, the site for the peroneus longus tendon was all prepared for harvesting in case of inappropriate harvesting of semitendinosus or gracilis tendon. In their study, Hiemstra et al. [3] documented the outcomes of ACL reconstruction combined with MPFL imbrication in a group of five patients, and reconstruction in 13 patients utilizing allograft and hamstring autografts. Sillanpaa et al. [4] emphasized the importance of MPFL in preventing ACL reconstruction failures by reporting two cases where a second surgery was needed due to ongoing instability. These findings were consistent with the Hiemstra et al. [3] study, which showed that patellar stabilization was necessary alongside ACL revision in three cases. Considering positive patellar apprehension and a history of patellar dislocation, one patient in a study by Shankar et al. [1] underwent MPFL reconstruction even without the MRI evidence of an MPFL tear. All the previous studies described favorable results with no patellar or knee instability. Although there were problems with knee stiffness considering the different rehabilitation protocols. This was further emphasized by Shankar et al. [1], to perform aggressive rehabilitation from postoperative day 1 as two out of three patients experienced knee stiffness. Even in our series, aggressive exercises were performed as soon as the patient was comfortable. MPFL reconstruction does not alter the biomechanics of cruciate ligaments of the knee, thus warranting no delay in rehabilitation. None of the patients suffered knee stiffness in our study.
This article contributes to the evolving knowledge regarding the management of simultaneous ACL and patellofemoral instability, shedding light on diagnostic considerations, surgical techniques, and post-operative care. Orthopedicians should be aware of the potential for both injuries to coexist and should be managed simultaneously with aggressive physiotherapy.
The simultaneous ACL and MPFL injuries are a rare combination of injuries. The orthopedic surgeons should be aware of this morphology of injury. Oversighting the MPFL injury can lead to suboptimal results, another surgery for patellar dislocation/instability, delayed rehabilitation, and failures. The simultaneous surgical management of ACL and MPFL leads to more stable knee biomechanics, faster rehabilitation, and avoiding further surgeries.
References
- 1.Shankar V, Hussain SN, Sahanand S, Rajan D. Concurrent anterior cruciate ligament and medial patellofemoral ligament reconstruction: A case report and literature review. Cureus 2020;12:e7717. [Google Scholar | PubMed]
- 2.Macura M, Veselko M. Simultaneous reconstruction of ruptured anterior cruciate ligament and medial patellofemoral ligament with ipsilateral quadriceps grafts. Arthroscopy 2010;26:1258-62. [Google Scholar | PubMed]
- 3.Hiemstra LA, Kerslake S, Heard M, Buchko G, Lafave M. Outcomes of surgical stabilization in patients with combined ACL deficiency and patellofemoral instability-a case series. Knee 2016;23:1106-11. [Google Scholar | PubMed]
- 4.Sillanpaa PJ, Elo J, Mattila VM, Pihlajamaki H. Incidence and nature of simultaneous anterior cruciate ligament injury and patellar dislocation-analysis of 130 708 young adults. Arthrosc J Arthrosc Relat Surg 2012;28:???. [Google Scholar | PubMed]
- 5.Victor J, Wong P, Witvrouw E, Sloten JV, Bellemans J. How isometric are the medial patellofemoral, superficial medial collateral, and lateral collateral ligaments of the knee? Am J Sports Med 2009;37:2028-36. [Google Scholar | PubMed]
- 6.Dirim B, Haghighi P, Trudell D, Portes G, Resnick D. Medial patellofemoral ligament: Cadaveric investigation of anatomy with MRI, MR arthrography, and histologic correlation. Am J Roentgenol 2008;191:490-8. [Google Scholar | PubMed]
- 7.Sillanpää PJ, Peltola E, Mattila VM, Kiuru M, Visuri T, Pihlajamäki H. Femoral avulsion of the medial patellofemoral ligament after primary traumatic patellar dislocation predicts subsequent instability in men: A mean 7-year nonoperative follow-up study. Am J Sports Med 2009;37:1513-21. [Google Scholar | PubMed]
- 8.Camanho GL, de Christo Viegas A, Bitar AC, Demange MK, Hernandez AJ. Conservative versus surgical treatment for repair of the medial patellofemoral ligament in acute dislocations of the patella. Arthroscopy 2009;25:620- 5. [Google Scholar | PubMed]
- 9.Christiansen SE, Jakobsen BW, Lund B, Lind M. Isolated repair of the medial patellofemoral ligament in primary dislocation of the patella: A prospective randomized study. Arthroscopy 2008;24:881-7. [Google Scholar | PubMed]
- 10.Schöttle PB, Fucentese SF, Romero J. Clinical and radiological outcome of medial patellofemoral ligament reconstruction with a semitendinosus autograft for patella instability. Knee Surg Sports Traumatol Arthrosc 2005;13:516-21. [Google Scholar | PubMed]
- 11.Deie M, Ochi M, Sumen Y, Adachi N, Kobayashi K, Yasumoto M. A long-term follow-up study after medial patellofemoral ligament reconstruction using the transferred semitendinosus tendon for patellar dislocation. Knee Surg Sports Traumatol Arthrosc 2005;13:522-8. [Google Scholar | PubMed]
- 12.Steensen RN, Dopirak RM, Maurus PB. A simple technique for reconstruction of the medial patellofemoral ligament using a quadriceps tendon graft. Arthroscopy 2005;21:365-70. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Evaluating Surgical Strategies and Functional Outcomes in Multi-Ligamentous Knee Injuries: A Prospective Study in Indian Patients
January 1, 2026 Evaluating Surgical Strategies and Functional Outcomes in Multi-Ligamentous Knee Injuries: A Prospective Study in Indian Patients August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report
August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study