Peri-lunate dislocations are relatively rare injuries which are often missed on clinical and radiological diagnosis. Timely identification and early intervention are of utmost importance in improving prognosis.
Dr. Ishaan Siwach, Central Institute of Orthopaedics, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. E-mail: drishaansiwach@gmail.com
Introduction: Perilunate dislocations are rare high-energy injuries which may often have the potential to cause lifelong disability of the wrist if not addressed optimally. Hence, early recognition, diagnosis, and intervention are of paramount importance in the restoring function and prevention of morbidity. Lunate dislocations are the fourth and last stage of perilunate dislocations being extremely rare, with volar dislocations representing <3% of perilunate dislocations.
Case Report: A 24-year-old man suffered from an alleged history of fall from a bike on an outstretched hand following which he developed complaints of pain and swelling in the right wrist. On examination, the patient has relative sensory loss over the lateral half of the palm with no vascular deficit. An accurate range of motion could not be documented due to severe pain. Standard digital X-rays revealed lunate displaced and angulated volarly with a typical “spilled teacup” appearance along with radial and ulnar styloid fractures.
Management: The patient was initially given an attempt of closed reduction which was not successful and was followed with open reduction and internal fixation with both volar and dorsal approach with Kirschner wires. The patient’s wrist was immobilized for 6 weeks with below elbow cast with the removal of k wires at 8 weeks after which wrist ROM exercises were started.
Results: The patient was followed up for 6 months and now has a functional range of motion of the wrist with no sensory deficit and is able to continue with his profession as a car mechanic.
Conclusion: Mayfield progression Stage 4 perilunate dislocations are uncommon with a poor prognosis if not addressed timely. Hence, these injuries need to be identified early and optimally managed with surgical intervention for a favorable outcome.
Keywords: Perilunate dislocation, carpal bones, avascular necrosis of lunate, wrist trauma, carpal instability
Perilunate dislocations are rare high-energy injuries (<10% of all wrist injuries) [1] which may often have the potential to cause lifelong disability of the wrist if not addressed optimally. Perilunate dislocations and fracture dislocations are most often a result of high-energy trauma, exerting an axial load with hyperextension and ulnar deviation of the wrist, along with intercarpal supination [2]. Hence, early recognition, diagnosis, and intervention are of paramount importance in the restoring function and prevention of morbidity such as median nerve injury, carpal instability, avascular necrosis of the lunate, complex regional syndrome, unreliable return of function, and post-traumatic arthritis requiring a secondary salvage surgical procedure [3]. Despite optimal treatment, perilunate dislocations and fracture-dislocations at the wrist cause functional sequelae such as pain, stiffness, strength deficit, and post-traumatic arthritis in nearly 80% of patients. The functional outcomes are determined by the amount of lunate displacement (stage) and the patient’s age [4]. Lunate dislocations are the fourth and last stage of Mayfield staging [5] of perilunate dislocations being extremely rare, with volar dislocations representing <3% of perilunate dislocations [6].
A 24-year-old gentleman suffered from an alleged history of falling from a bike on an outstretched hand following which he developed complaints of pain and swelling in the right wrist and presented to us 1 day after his injury having received splintage elsewhere. On examination, the patient had swelling and tenderness on this wrist joint with relative sensory loss over the lateral half of the palm with no vascular deficit. An accurate range of motion could not be documented due to severe pain. Standard digital radiographs with a postero-anterior view revealed disruption of the Giliua’s 2nd arch with overlapping lunate and capitate along with radial and ulnar styloid fractures (Fig. 1 and 2). A lateral radiograph (Fig. 3) showed lunate displaced and angulated volarly with a typical “spilled teacup” appearance along with the scapholunate angle being greater than 85°.
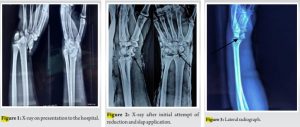
The patient was administered IV analgesics and fluids following which an attempt of closed reduction was given using Tavernier’s method which was unsuccessful (Fig. 4). The patient was then taken up under anesthesia and underwent open reduction using combined volar and dorsal approach and lunate was fixed using scapholunate, triquetro-lunate, and capito-lunate Kirschner wires followed by fixation of radial styloid using 4 mm Cannulated cancellous screw, scapholunate ligament repair was also done (Fig. 5). Patient’s wrist was immobilized with above elbow slab for 2 weeks followed by application of below elbow cast after suture removal for 6 weeks (Fig. 6).

The patient underwent K wire removal at 8 weeks (Fig. 7) and started gentle physiotherapy and wrist range of motion exercises. The patient was followed up for 6 months and now has a functional range of motion of the wrist (flexion 80° and dorsiflexion 85°) with full supination and mildly restricted pronation (60°) as seen in Fig. 8-11.

The patient has no sensory deficit with adequate wrist grip strength is able to continue with his profession as a car mechanic and has a Mayo wrist score of 80% (Fig. 8-11).

Perilunate dislocations are the results of high-energy trauma to the wrist. Green and O’Brien [7] described Volar Perilunate dislocations to take place due to a fall onto the hyperextended wrist with the forearm supinated resulting in a pure dislocation whereas a fall onto hyperextended wrist without forearm supination results in a fracture dislocation.
Mayfield et al. [5] classified carpal instability into four stages:
Stage 1: Scapholunate dislocation
Stage 2: Perilunate dislocation
Stage 3: Midcarpal dislocation
Stage 4: Lunate dislocation
Four ligaments, namely, palmar and dorsal radio-carpal ligaments, and ulnar and radial collateral ligaments, are primarily responsible for maintaining the stability of the wrist joint. Palmar ligaments have high tensile strength and may remain intact even after perilunate dislocation, but there exists an interval of weakness between the capitate and lunate called “Space of Poirier” [8] through which the lunate may dislocate volarly. For a Perilunate dislocation, bony stabilization, as well as repair of the injured ligament and joint capsule are equally important to prevent joint instability. Volar perilunate dislocations may frequently be associated with median nerve compression for which carpal tunnel decompression using the volar approach is required [9]. Volar/dorsal approach or dual approach may be used for open reduction and fixation of perilunate dislocations, Yadav et al. [10] have used a single volar approach for surgical management of this injury whereas Thomas et al. [8] have used dual incision which is similar to our case. Yadav et al. [10] opine that despite operative treatment, return to full function is highly unlikely, however, we are reporting a near total range of motion with a good functional outcome in our case as described above. Thomas et al. [8] have also reported a full range of movement with no carpal instability in their study, which is comparable to our case. Anatomical reduction with stable fixation followed by ligamentous repair plays a major role in providing the best outcomes to the patient.
Mayfield progression Stage 4 perilunate dislocations are uncommon with a poor prognosis if not addressed timely. Favorable outcomes may be achieved following early recognition of these injuries followed by restoration of carpal alignment by open reduction and ligamentous repair if required.
Perilunate dislocations – often missed on initial presentations by inexperienced practitioners require timely identification and intervention which is crucial to a good prognosis following surgery. Successful open reduction of these injuries involves ligamentous repair of at least the scapholunate ligament which prevents morbidity associated with carpal instability.
References
- 1.Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J. Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-79. [Google Scholar]
- 2.Najarian R, Nourbakhsh A, Capo J, Tan V. Perilunate injuries. Hand (N Y) 2011;6:1-7. [Google Scholar]
- 3.Kastanis G, Velivasakis G, Pantouvaki A, Spyrantis M. An unusual localization of lunate in a transcaphoid volar lunate dislocation: Current concepts. Case Rep Orthop 2019;2019:7207856. [Google Scholar]
- 4.Garçon C, Degeorge B, Coulet B, Lazerges C, Chammas M. Perilunate dislocation and fracture dislocation of the wrist: Outcomes and long-term prognostic factors. Orthop Traumatol Surg Res 2022;108:103332. [Google Scholar]
- 5.Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-41. [Google Scholar]
- 6.Youssef B, Deshmukh SC. Volar perilunate dislocation: A case report and review of the literature. Open Orthop J 2008;11:57-8. [Google Scholar]
- 7.Green DP, O’Brien ET. Classification and management of carpal dislocations. Clin Orthop Relat Res 1980;149:55-72. [Google Scholar]
- 8.Thomas J, Makki D. Palmar lunate dislocation with Tran scaphoid fracture dislocation and trapezium fracture-a case report of rare fracture presentation. Trauma Case Rep 2022;23:100736. [Google Scholar]
- 9.Başar H, Başar B, Erol B, Tetik C. Isolated volar surgical approach for the treatment of perilunate and lunate dislocations. Indian J Orthop 2014;48:301-5. [Google Scholar]
- 10.Singh S, Yadav S, Arya R, Sharma D. Volar perilunate dislocation with acute median nerve compression: A case study and literature review. J Postgrad Med Educ Res 2018;52:187-9. [Google Scholar]