
It is possible to have a mechanical block to motion in a concentrically reduced proximal interphalangeal joint, which necessitates examination under digital block as a diagnostic adjunct for prompt diagnosis and intervention.
Dr. Keith T Aziz, Department of Orthopedic Surgery, Mayo Clinic Florida, Jacksonville, Florida. E-mail: aziz.keith@mayo.edu
Abstract
Introduction: Fracture-dislocations of the proximal interphalangeal joint (PIPJ) can have a significant impact on digital motion and hand function if inappropriately treated. While these injuries are commonly encountered, they can be quite challenging to manage. It is critical to ensure a concentric reduction and early motion when treating these injuries.
Case Report: A 17-year-old woman sustained a fracture-dislocation of the PIPJ of the left small finger. Despite a concentric closed reduction, she had pain and a mechanical block to PIPJ motion. Axial imaging revealed volar entrapment plate in the retrocondylar space. She was treated with open reduction and direct volar plate repair. Postoperatively, the patient had an excellent outcome with no complications.
Conclusion: Our case highlights the importance of both performing an anesthetized examination and investigating the etiology of any limitations to motion even if there is an initial acceptable closed reduction.
Keywords: Proximal interphalangeal joint×PIP, volar plate, interphalangeal dislocation, fracture-dislocation.
The volar plate is a multilayered condensation of fibrocartilaginous tissue that plays a critical role in maintaining the stability and alignment of the proximal interphalangeal joint (PIPJ) of the hand [1-4]. Thus, volar plate injuries might lead to PIPJ instability, and if left untreated, chronic deformities of the PIPJ might result [1,2]. Injuries to the volar plate of the finger are most common in younger individuals, particularly in those participating in sports [5]. Volar plate injuries typically occur due to an axial load placed on the PIPJ. If the force is sufficiently large enough, a dislocation of the middle phalanx can occur, with the directionality of the dislocation dictated by the position of the digit when the load is applied. Dorsal PIPJ dislocations are most common and occur as a result of a hyperextension injury [2-6]. Typically, these injuries are managed with careful closed reduction of the PIPJ dislocation. However, in some cases, the volar plate can become entrapped within the PIPJ, necessitating operative intervention [7]. We report a case of a 17-year-old female athlete who sustained a dorsal PIPJ dislocation that was appropriately reduced in a concentric fashion, who was found to have entrapment of the volar plate within the retrocondylar space causing pain and a mechanical block to motion. She underwent open reduction of the volar plate and direct repair with excellent outcome.
A 17-year-old right hand dominant woman presented to our clinic for follow-up after having previously sustained a dorsal dislocation of the PIPJ of the left small finger as a result of an axial load to the digit while playing basketball 10 days prior. She had multiple reduction attempts performed at an outside facility, but ultimately successful concentric reduction was achieved. After closed reduction, she was placed into a removable Velcro ulnar gutter splint and encouraged to mobilize the joint. She presented to our institution for follow-up with persistent pain and swelling. On our initial examination, she had intact sensation and perfusion distal to the PIPJ. She had tenderness about the PIPJ but was stable to radial and ulnar stress of the joint. The flexor digitorum profundus and flexor digitorum superficialis tendons were intact. Her range of motion (ROM) at the metacarpophalangeal (MCP) and distal interphalangeal (DIP) joints was 0°–90°, and 0°–45°, respectively. With attempted flexion of the PIPJ, she had pain at about 60° of flexion. After a digital block, an examination under anesthesia was performed and there was no improvement in her active flexion. Plain radiographs demonstrated a well-reduced PIPJ, without subluxation or interval dislocation (Fig. 1a, b, c). There was also a fracture of the base of the left small finger middle phalanx, suggestive of a volar plate avulsion fracture (Fig. 1d). Dynamic evaluation of the PIPJ on fluoroscopy evaluation in clinic demonstrated a concentrically reduced joint with stability, but persistent inability to passively or actively flex the PIPJ beyond 60°. The patient was then placed into a left small finger PIP dorsal-blocking splint and a magnetic resonance imaging (MRI) of the left small finger was obtained to evaluate the joint and surrounding soft tissue.

The MRI demonstrated a 5 mm × 3 mm avulsion fracture of the volar aspect of the middle phalanx, with approximately 3 mm of proximal retraction, involving <30% of the articular surface (Fig. 2). The volar plate was attached to the fracture fragment and sat within the retrocondylar space of Drucker (Fig. 2). After reviewing the imaging, the decision was made to proceed with open volar plate repair to remove any interposed soft tissue and ensure PIPJ stability and restore ROM.

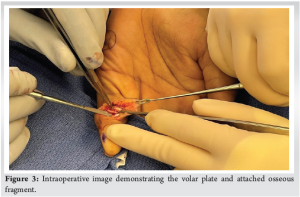
The patient subsequently underwent open volar plate repair, where a trapezoidal incision was made on the ulnar aspect of the left small finger and the A3 pulley was incised (Fig. 3). Intraoperatively, the volar plate and volar articular fragment were found to be rotated approximately 270° and encased in significant scar tissue in the retrocondylar space of Drucker (Fig. 3). The scar tissue was released and mobilized, and the volar plate was unfurled. Proper reduction of the fracture fragment at the base of the middle phalanx was facilitated using bicondylar suture anchors (Fig. 4). Following fixation, the A3 pulley was repaired with sutures into the volar plate over the fiber wire fixation construct and the surgical incision was closed. To protect the volar plate repair, the patient’s left small and ring fingers were immobilized in a dorsal extension-blocking splint in slight flexion at the PIPJ. The patient was then referred to occupational therapy to begin passive ROM exercises within 1 week of the repair to avoid stiffness.
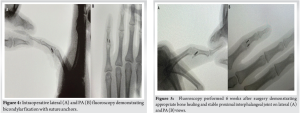
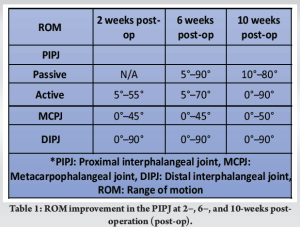
Six weeks after her left small finger surgery, the patient’s surgical incisions were well healed. There was an improvement in passive and active ROM of the PIPJ but she had not regained full ROM (Fig. 5 and Table 1). At her follow-up appointment 10 weeks after her left small finger surgery, she demonstrated excellent motion at the MCP (0–90°), DIP (0–50°), and PIP (10–80°) joints and the ability to make a full composite fist (Fig. 6 and Table 1). She has had no functional obstacles that necessitate a follow-up evaluation since her 10-week post-operative appointment.

PIPJ injuries are some of the most common injuries of the hand, particularly in athletes. These injuries can range from simple sprains to major soft-tissue trauma and fracture-dislocations, with each injury having its own assortment of treatment options [7-10]. Clinically, patients with volar plate or PIPJ injuries often have pain, swelling, and ecchymosis focally about the joint. While the volar plate is comprised fibrocartilage and therefore radiolucent, there are often osseous avulsions that accompany injuries involving the volar plate. Compromise of the volar plate can impact PIPJ stability, and it is critical to scrutinize radiographs for the possibility of a non-concentric reduction. Typically, stable PIPJ injuries with a concentrically reduced joint are conservatively treated with splint and hand therapy with early mobilization. If patients fail conservative measures, serial passive manipulation or operative intervention is considered. Wollstein et al. describe a series of 52 patients with a concentrically reduced stable PIPJ who failed non-operative management and ultimately underwent a direct volar plate repair [11]. All patients who were treated with direct volar plate repair had failed at least 2 months of conservative treatment and had involvement of <40% of the middle phalangeal base [11]. In our case, we utilized an exam under anesthesia and noted persistent mechanical block to both passive and active motion. Due to this, early axial imaging was obtained to evaluate the PIPJ. While our patient underwent surgical intervention at an earlier time, the ROM improvement achieved by our patient is comparable to that reported in Wollstein et al. This highlights the importance of utilizing an examination under digital block as an adjunctive clinical exam maneuver. To the best of our knowledge, this is the first described case report of a retracted volar plate encasing the middle phalangeal base volar lip fragment and causing a mechanical block to motion.
Our findings were confirmed both by MRI and clinically during direct open repair of the volar plate. This case highlights the utility of an anesthetized exam when evaluating patients with PIPJ injuries. In our case, operative exploration with direct repair of the volar plate and suture anchor fixation of the volar lip fracture fragment provided a good outcome without complications.
We believe special consideration should be given in cases where there is a mechanical block to flexion under anesthetized examination to expedite operative intervention and post-operative recovery.
References
- 1.Caviglia D, Ciolli G, Fulchignoni C, Rocchi L. Chronic post-traumatic volar plate avulsions of the finger proximal interphalangeal joint: A literature review of different surgical techniques. Orthop Rev (Pavia) 2021;13:9058. [Google Scholar | PubMed]
- 2.Pattni A, Jones M, Gujral S. Volar plate avulsion injury. Eplasty 2016;16:ic22. [Google Scholar | PubMed]
- 3.Alotaibi AS, AlMarshad FA, Alzahrani AM, Hossein MO, Ijaz A, Ifthikar Z, et al. Simultaneous central slip and volar plate injuries at pip joint: A novel therapeutic approach. Plast Reconstr Surg Glob Open 2021;9:e3923. [Google Scholar | PubMed]
- 4.Pang EQ, Yao J. Anatomy and biomechanics of the finger proximal interphalangeal joint. Hand Clin 2018;34:121-6. [Google Scholar | PubMed]
- 5.Hardy M. Principles of metacarpal and phalangeal fracture management: A review of rehabilitation concepts. J Orthop Sports Phys Ther 2004;34:781-99. [Google Scholar | PubMed]
- 6.Blazar PE, Steinberg DR. Fractures of the proximal interphalangeal joint. J Am Acad Orthop Surg 2000;8:383-90. [Google Scholar | PubMed]
- 7.Aziz KT, London DA, Stern PJ. Adult Phalangeal Base Fractures: Pilons, Avulsions, PIPJ Fracture-Dislocations. Ch. 5. New York City: Springer International Publishing; 2023. [Google Scholar | PubMed]
- 8.Kamnerdnakta S, Huetteman HE, Chung KC. Complications of proximal interphalangeal joint injuries. Prevention and treatment. Hand Clin 2018;34:267-88. [Google Scholar | PubMed]
- 9.Elfar J, Mann T. Fracture-dislocations of the proximal interphalangeal joint. J Am Acad Orthop Surg 2013;21:88-98. [Google Scholar | PubMed]
- 10.Freiberg A. Management of proximal interphalangeal joint injuries. Can J Plast Surg 2007;15:199-203. [Google Scholar | PubMed]
- 11.Wollstein R, Watson HK, Carlson L. A technique for the repair of chronic volar plate avulsion of the proximal interphalangeal joint: A review of 54 cases. Plast Reconstr Surg 2006;117:1239-45, discussion 1246-7. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Pediatric Tibial Plateau Fracture-Dislocation: A Case Report
February 1, 2026 Pediatric Tibial Plateau Fracture-Dislocation: A Case Report November 1, 2025 Bilateral simultaneous distal radius fractures with elbow dislocations following a fall from height: A rare orthopedic quadruple injury with review of the literature
November 1, 2025 Bilateral simultaneous distal radius fractures with elbow dislocations following a fall from height: A rare orthopedic quadruple injury with review of the literature November 1, 2024 Fixation of 3-Part Intra Articular Distal Radius Fracture with Combined Volar Plate and Dorsal Spanning Plate: A Case Report
November 1, 2024 Fixation of 3-Part Intra Articular Distal Radius Fracture with Combined Volar Plate and Dorsal Spanning Plate: A Case Report October 1, 2024 L4-L5 Facet Dislocation Treated in a Delayed Fashion with Excellent Early Clinical Results
October 1, 2024 L4-L5 Facet Dislocation Treated in a Delayed Fashion with Excellent Early Clinical Results