
For treating a gap nonunion of the humerus with failed osteosynthesis, using a locking compression plate (LCP) combined with a fibula strut graft and an iliac crest bone graft is considered a highly effective method. This approach is often regarded as a gold standard due to its ability to provide both structural support and biological enhancement for bone healing.
Dr. Rohan Raj Baruah, Department of Orthopaedics, D.Y. Patil Hospital, Navi Mumbai, Maharashtra, India. E-mail: drrohanrajbaruah@gmail.com
Abstract
Introduction: The humeral shaft gap non-union treatment surgically after unsuccessful fixation is difficult. In this study, the functional outcome of unsuccessful fixation of humeral shaft gap non-unions using a locking compression plate (LCP), fibular strut graft, and iliac bone graft was evaluated.
Case Report: we studied 10 patients with humeral shaft gap non-unions with unsuccessful surgical fixation treated with open reduction and internal fixation using LCP with fibular strut graft and iliac cancellous bone graft. The study duration was from January 2022–January 2024. The mean time from non-union was 7 months. Disabilities of the arm, shoulder, and hand (DASH) scores improved significantly from a pre-operative average of 59.2 ± 7.3 to a mean final score of 24.6 ± 4.8 reflecting a mean improvement of 34.6 with no complications.
Conclusion: This study shows that LCP with fibular strut graft and iliac bone grafts is a good alternative for diaphyseal humerus gap non-union along with statistically significant improvement in functional outcome, with union seen in all cases. This construct augments biomechanical stability and good biological healing in these gap non-unions.
Keywords: Humeral fracture, non-union, locking compression plating, humerus, fibular strut graft.
Gap non-union of the shaft of the humerus fractures can be difficult to treat, particularly when standard bone healing techniques fail. Complicating variables such as implant loosening caused by disuse osteoporosis, osteolysis, comminution, or severe bone depletion make therapy even more challenging [1]. Several treatment options have been documented, including open reduction and internal fixation using dynamic compression plate, locking compression plate (LCP), intramedullary interlocking nail, and external fixation. However, getting successful results remains difficult, especially when stability is impaired due to implant loosening or bone quality concerns [1]. Fibular strut grafting, when paired with plating, appears to be a promising treatment for humerus gap non-union. This treatment improves stability and biological support for gap non-unions in long bone fractures when compared to traditional procedures [2, 3]. Furthermore, autologous bone grafts remain the “gold standard,” with the iliac crest being the most often harvested region [4]. Our study aims to investigate the efficacy of using a non-vascularized fibular strut graft in conjunction with autologous iliac crest bone graft and locking compression plating to treat humerus shaft gap non-unions caused by failed previous fixations.
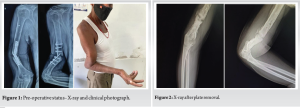
Approval from the ethics committee was taken from D.Y. Patil Hospital (Number-265), Nerul, Navi Mumbai for our study. Informed consent was taken from all patients. Data were collected retrospectively from the institute for a period of 2 years from January 2022 to January 2024 for operated cases of gap non-union of humerus fracture with failed primary osteosynthesis. Inclusion criteria were non-union humerus with a significant gap (>4 mm), age >18 years, and non-union duration of >1 year (Fig. 1). Exclusion criteria were cases with infection, congenital abnormalities, compound fractures, and patients with neuropathic diseases. As there was a gap non-union and instability at the fracture site, intramedullary stability was given by autologous fibular strut graft along with iliac crest cancellous graft in addition to LCP. We selected the same side fibula for cortical strut graft to provide added stability and iliac crest graft for osteo-induction at the site of fracture with LCP. Clinical and radiological follow-up was done for all 10 patients regularly with no loss of follow-up.
Surgical techniques
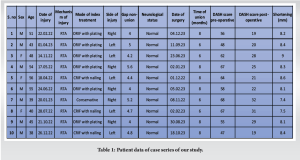
All cases were operated on under supra-clavicular block and general anesthesia. Regional anesthesia was given for post-operative pain analgesia. There were two teams operating simultaneously to save time. One team harvested the ipsilateral fibula as the patient was in a lateral position and the other team was operating on the humerus non-union site. The standard procedure for ipsilateral fibula removal was done under a tourniquet. The graft taken was from the central 1/3rd of the fibula making sure to preserve knee and ankle instability and avoiding peroneal nerve injury. The graft harvested was approximately 8–14 cm (Figs. 2 and 3). We did multiple drill holes proximally and distally before doing an osteotomy.
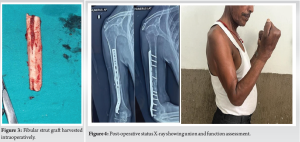
The incision of the humerus was taken over the old healed surgical scar. Old implants were removed from the fracture site and an X-ray was taken to assess the non-union (Fig. 2). The scarred and fibrous tissue were removed along with bone debridement till bleeding bone edges were seen. Mobilization of the radial nerve was performed. Shingling was done at the fracture ends. Sequential reaming with rigid reamers was done in the proximal and distal fragment to recanalize the medullary canal so that the fibular strut graft snuggly fits. The fibular strut graft was placed at the fracture site making sure that the center of the graft is at the fracture site. Cancellous bone grafting taken from the iliac crest was put at the graft-humerus interface in all patients to improve the chances for the bony union. Fixation was done with a 12–15 holed 4.5 mm LCP. In all patients, both the proximal and distal humerus fragments had four screws each.
Post-operative follow-up
Postoperatively, the patients were given a universal shoulder immobilizer for 4 weeks and active shoulder and elbow range of motion exercises were done. Follow-up of patients was done every 2 weeks till 1 month. Then, monthly follow-up was done till union was seen radiologically. Later, follow-up was done every 2 months. All 10 patients were followed up for a minimum of 2 years, that is, 24 months. Functional assessment was examined by disabilities of the arm, shoulder, and hand (DASH) score both before and after the operation.
Ten patients were screened with humeral non-union following failed primary osteosynthesis with male:female ratio of 7:3. The average age of the patients was 46.9 years (±6.52). The average duration of non-union since the initial surgery was around 1.2 years, with average bone gaps of 4.59 mm (±0.53). Five patients on the left and right side each were studied. Each patient had undergone 1–2 previous procedures. The sites were predominantly in the middle third of the humerus. Patients with signs of infection were excluded, and erythrocyte sedimentation rate and C-reactive protein values were checked to rule out infections. Follow-up was for a minimum of 24 months, during which all cases achieved union at an average time of 7.2 months (±0.97), seen by the union in at least three of the four cortices on X-rays (Fig. 4). No pain was reported at the site, with the average time to the radiological union being 7 months (Table 1).
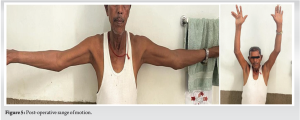
Clinically, the mean shortening of the arm was around 8.2 mm (±0.47) compared to the other side. Post-operative abduction and flexion of the shoulder were seen to be reduced by a mean of 15° each, though pre-operative elbow flexion stiffness resolved partially in all patients. Patients’ activity levels returned to near pre-injury status, with the DASH scores improving significantly from a pre-operative average of 59.2 ± 7.3 to a mean final score of 24.6 ± 4.8 reflecting a mean improvement of 34.6. Results of the paired t-test indicated that there is a significant large difference between before (M = 59.2, SD = 7.7) and after (M = 24.6, SD = 5.1), t (9) = 19, P < 0.001. Satisfaction with the treatment was high among all patients, and no graft site complications is seen (Fig. 5).
Non-union of the shaft of the humerus, particularly in complex cases, is an issue influenced by many factors such as pattern of fracture, interposition of soft tissue, quality of primary fixation [4], and factors such as smoking, obesity, alcoholism, and diabetes [5]. After failed treatment, complications such as poor fracture end contact, inadequate stabilisation, bone devitalization, osteopenia, and bone defects are seen. These patients generally present with gap non-union, local osteoporosis due to disuse, and various implant-related issues such as breakage and metallosis, making surgical reconstruction tough. Several options are there for fixing gap non-union of the humerus with bone defects, including plating, nailing, and external fixators. Our preferred method is LCP due to its rigidity and suitability for osteopenic bones [6, 7, 8]. LCP offers stable fracture stability and solves issues related to poor bone quality and screw purchase [9, 10].
In our approach, we used fibular strut grafts for their structural integrity and minimal harvest site morbidity, along with iliac crest grafts for added strength at the site. This method avoids shortening and provides immediate stability post-surgery. Despite concerns about graft resorption due to inadequate vascularity, our results did not show any failures. Compared to other options such as bone transport or the use of bone morphogenetic proteins, autologous fibular grafts are cost-effective and suitable in settings with limited resources. While fibular strut grafts may theoretically disrupt blood supply, immediate fixation mitigates this risk, ensuring graft survival [11]. Wright et al. [12] used an intramedullary fibular bone graft and a compression plate in nine humeral non-unions. Morsi (union in 6 out of 7, 86%), Steinlechner and Mkandawire (union in 7 out of 8, 88%), and Lawal et al. (union in 8 out of 10, 80%) all reported excellent results in their respective studies on non-vascularized fibular grafting concluding separately that it is a comparatively simple procedure with excellent results [13, 14]. Lawal et al. succeeded in achieving graft incorporation in eight out of the ten patients they included in three series. The average defect was 6.5 cm. They concluded that free fibular grafting is a good option for bone defects in developing countries [15]. Our series, though limited to 10 patients, demonstrated less complication and supports the reliability and cost-effectiveness of using fibular strut grafts for complex humerus gap non-unions. Complications were negligible, showing the viability of this technique in limited resource settings.
We conclude that the combination of iliac crest graft with fibular strut graft and fixation using LCP is a good option for complex humerus non-union in the diaphysis where bone loss and osteopenia are seen. Using a fibular strut graft added biomechanical stability in osteoporosis, while an iliac crest bone graft enhanced the biological environment of the site of fixation. This approach showed an average improvement of the DASH score by 34.6 points, with all cases returning to their previous activity levels with achieving full union radiologically even when there were multiple failed surgeries previously The procedure can be performed with less complications and serves as a feasible option in less resourceful settings where bone banks, allografts, or bone morphogenetic proteins are not available.
For treating a gap non-union of the humerus with failed osteosynthesis, using a LCP combined with a fibular strut graft and an iliac crest bone graft is considered a highly effective method. This approach is often regarded as a gold standard due to its ability to provide both structural support and biological enhancement for bone healing.
References
- 1.Peters RM, Claessen FM, Doornberg JN, Kolovich GP, Diercks RL, van den Bekerom MP. Union rate after operative treatment of humeral shaft nonunion--A systematic review. Injury 2015;46:2314-24. [Google Scholar | PubMed]
- 2.Gopisankar G, Justin AS, Nithyananth M, Cherian VM, Lee VN. Non-vascularised fibular graft as an intramedullary strut for infected non-union of the humerus. J Orthop Surg (Hong Kong) 2011;19:341-5. [Google Scholar | PubMed]
- 3.Padhye KP, Kulkarni VS, Kulkarni GS, Kulkarni MG, Kulkarni S, Kulkarni R, et al. Plating, nailing, external fixation, and fibular strut grafting for non-union of humeral shaft fractures. J Orthop Surg (Hong Kong) 2013;21:327-31. [Google Scholar | PubMed]
- 4.Dimitriou R, Mataliotakis GI, Angoules AG, Kanakaris NK, Giannoudis PV. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: A systematic review. Injury 2011;42:S3-15. [Google Scholar | PubMed]
- 5.Pascarella R, Ponziani L, Ferri M, Ercolani C, Zinghi GF. Aseptic nonunion of the humeral shaft. Chir Organi Mov 2000;85:29-34. [Google Scholar | PubMed]
- 6.Dimitriou R, Dahabreh Z, Katsoulis E, Matthews SJ, Branfoot T, Giannoudis PV. Application of recombinant BMP-7 on persistent upper and lower limb non-unions. Injury 2005;36:S51-9. [Google Scholar | PubMed]
- 7.Patel VR, Menon DK, Pool RD, Simonis RB. Nonunion of the humerus after failure of surgical treatment. Management using the Ilizarov circular fixator. J Bone Joint Surg Br 2000;82:977-83. [Google Scholar | PubMed]
- 8.Barquet A, Fernandez A, Luvizio J, Masliah R. A combined therapeutic protocol for aseptic nonunion of the humeral shaft: A report of 25 cases. J Trauma 1989;29:95-8. [Google Scholar | PubMed]
- 9.Hierholzer C, Sama D, Toro JB, Peterson M, Helfet DL. Plate fixation of ununited humeral shaft fractures: Effect of type of bone graft on healing. J Bone Joint Surg Am 2006;88:1442-7. [Google Scholar | PubMed]
- 10.Babhulkar S, Babhulkar S, Vasudev A. Recalcitrant aseptic atrophic non-union of the shaft of the humerus after failure of surgical treatment: Management by excision of non-union, bone grafting and stabilization by LCP in different modes. Injury 2017;48:S33-43. [Google Scholar | PubMed]
- 11.Roberts TT, Rosenbaum AJ. Bone grafts, bone substitutes and orthobiologics: The bridge between basic science and clinical advancements in fracture healing. Organogenesis 2012;8:114-24. [Google Scholar | PubMed]
- 12.Wright TW, Miller GJ, Vander Griend RA, Wheeler D, Dell PC. Reconstruction of the humerus with an intramedullary fibular graft. A clinical and biomechanical study. J Bone Joint Surg Br 1993;75:804-7. [Google Scholar | PubMed]
- 13.Morsi E. Tibial reconstruction using a non-vascularised fibular transfer. Int Orthop 2002;26:377-80. [Google Scholar | PubMed]
- 14.Steinlechner CW, Mkandawire NC. Non-vascularised fibular transfer in the management of defects of long bones after sequestrectomy in children. J Bone Joint Surg Br 2005;87:1259-63. [Google Scholar | PubMed]
- 15.Lawal YZ, Garba ES, Ogirima MO, Dahiru IL, Maitama MI, Abubakar K, et al. Use of non-vascularized autologous fibula strut graft in the treatment of segmental bone loss. Ann Afr Med 2011;10:25-8. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report
April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report
January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report August 1, 2026 Functional Outcomes of Valgus Osteotomy in Young Patients of Intracapsular Neck of Femur Fracture: A Case Series
August 1, 2026 Functional Outcomes of Valgus Osteotomy in Young Patients of Intracapsular Neck of Femur Fracture: A Case Series July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall
July 1, 2026 Brown’s Tumor Presenting as a Pathological Humerus Fracture: A Rare Diagnostic Pitfall