
Routine biochemical evaluation is essential in all cases of pathological fractures to avoid misdiagnosis of metabolic bone disease as primary bone tumours.
Dr L. Adithya Narayan, Department of Orthopaedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur - 600 116, Chennai, Tamil Nadu, India. E-mail: adiano97@gmail.com
Abstract
Introduction: Brown’s tumour represents a late skeletal manifestation of long-standing hyperparathyroidism and is characterised by focal osteoclastic activity. Although benign, its presentation can resemble aggressive bone lesions and may lead to diagnostic confusion, particularly when associated with pathological fractures.
Case Report:: A 31-year-old male presented with right arm pain and deformity following trivial trauma. Imaging revealed an expansile osteolytic lesion in the humeral shaft with an associated fracture. Biochemical evaluation revealed marked hypercalcaemia and significantly elevated parathyroid hormone levels. Functional imaging localised a hyperfunctioning parathyroid lesion. Following metabolic correction, the patient underwent parathyroidectomy and intramedullary fixation of the humerus. Histological findings confirmed parathyroid adenoma and reactive osteoclastic bone changes consistent with Brown’s tumour.
Conclusion: Metabolic bone disorders such as Brown’s tumour should be considered when evaluating lytic lesions with fractures. Early biochemical evaluation is essential to avoid misdiagnosis and unnecessary aggressive surgical intervention.
Keywords: Brown’s tumour, hyperparathyroidism, pathological fracture, humerus, osteitis fibrosa cystica.
Parathyroid hormone plays a critical role in calcium homeostasis by regulating bone turnover, renal calcium reabsorption, and intestinal absorption. Persistent elevation of parathyroid hormone results in increased osteoclastic activity, leading to bone resorption and skeletal demineralisation. Brown’s tumour is a non-neoplastic, reactive osseous lesion that develops in the setting of prolonged hyperparathyroidism. It represents localised areas of bone resorption, haemorrhage, and reparative fibrous tissue formation. Radiologically, these lesions may closely mimic other destructive bone conditions such as giant cell tumour, aneurysmal bone cyst, and metastatic disease, making diagnosis challenging. Pathological fractures may be the initial presentation, particularly in long bones. Due to its rarity and non-specific presentation, Brown’s tumour is frequently misdiagnosed. Accurate diagnosis requires careful correlation of clinical, radiological, and biochemical findings. This report highlights an uncommon presentation involving the humeral shaft with a pathological fracture, emphasising the importance of considering metabolic causes in similar clinical scenarios.
A 31-year-old male presented with pain, deformity, and functional limitation of the right arm following a low-velocity road traffic accident. Initial management elsewhere included immobilisation with a U-slab, after which he presented to our institution for further evaluation. There was no significant medical history; however, the patient had undergone right hemimandibulectomy in 2014 for a cystic odontogenic lesion. On examination, there was swelling, tenderness, and abnormal mobility at the mid-arm. Distal neurovascular status was intact. Plain radiographs of the right humerus (anteroposterior and lateral views) demonstrated a well-defined expansile osteolytic lesion involving the mid-shaft, associated with cortical thinning and a comminuted pathological fracture with lateral angulation. No periosteal reaction or matrix mineralisation was noted, and generalised osteopenia was evident (Fig. 1). Further imaging revealed additional lytic lesions in the distal femur along with diffuse skeletal demineralisation. Cervical spine and knee radiographs confirmed previous hemimandibulectomy with generalised osteopenia and osteolytic lesions, respectively (Fig. 2).
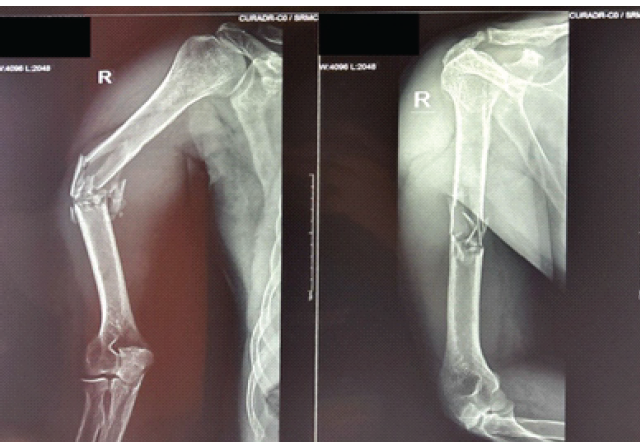
Figure 1: Pre-operative anteroposterior and lateral radiographs of the right humerus showing an expansile osteolytic lesion involving the mid-shaft with cortical thinning and associated pathological fracture.

Figure 2: Cervical spine and knee radiographs confirmed previous hemimandibulectomy with generalized osteopenia and osteolytic lesions, respectively.
Biochemical and functional imaging:
Laboratory investigations showed:
- Serum calcium: 14 mg/dL
- Parathyroid hormone: 2705 pg/mL
- Alkaline phosphatase: Elevated
- Inflammatory markers: Within normal limits
- Vitamin: D: 44 ng/mL.
Ultrasonography and a sestamibi scan localised a hyperfunctioning lesion in the left inferior parathyroid gland. Positron emission tomography-computed tomography demonstrated left parathyroid adenoma and mild lytic lesions in the skull and symmetrical uptake in multiple bones, suggestive of metabolic skeletal involvement (Fig. 3). Based on clinical, radiological, and biochemical findings, a diagnosis of Brown’s tumour of the right humerus presenting with a pathological fracture with a right distal femur osteolytic lesion secondary to primary hyperparathyroidism was established.
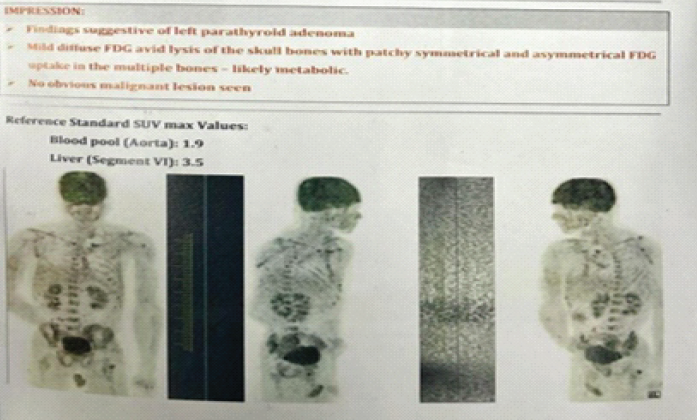
Figure 3: Positron emission tomography-computed tomography image confirming hyperfunctioning left inferior parathyroid adenoma with additional lytic lesions in the skull.
Management:
Initial management included immobilisation of the affected limb and administration of analgesics. Definitive treatment was planned through a multidisciplinary approach, prioritising correction of the underlying metabolic abnormality in coordination with the endocrinology and general surgery teams. Following adequate metabolic stabilisation, surgical fixation of the humeral fracture was undertaken. The patient was positioned in the beach-chair position. A small incision was made over the anterolateral aspect of the acromion, and the deltoid fibres were gently split to gain access. The entry point was established just medial to the greater tuberosity in alignment with the medullary canal using an entry awl. Fracture reduction was achieved under direct visualisation with the assistance of reduction clamps. A guidewire was then advanced across the fracture site, followed by sequential canal preparation by serial reaming. An intramedullary interlocking nail was inserted and secured with proximal and distal locking screws, achieving stable fixation. The wound was closed in layers. Subsequently, the patient underwent bilateral inferior parathyroidectomy for definitive management of hyperparathyroidism. Tissue samples from the excised parathyroid glands and the fracture site were sent for histopathological analysis. Sections from the parathyroid gland show proliferation of chief cells arranged in sheets with reduced stromal fat, consistent with parathyroid adenoma/hyperplasia. Sections from the fracture site show fibrovascular stroma with numerous multinucleated osteoclast-type giant cells, areas of haemorrhage, and haemosiderin-laden macrophages (Fig. 4).
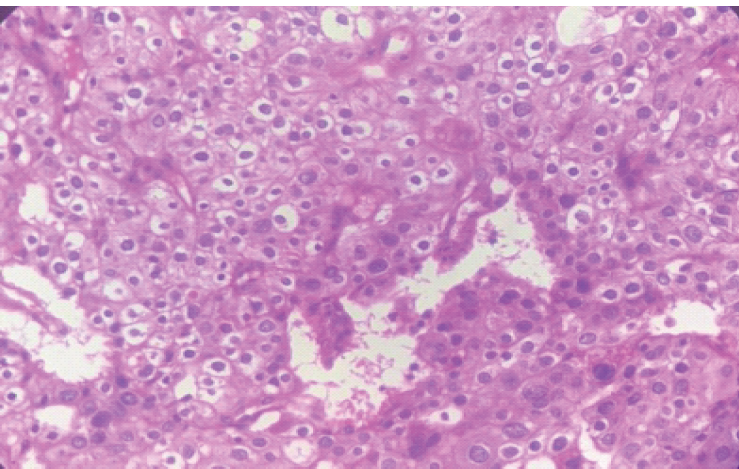
Figure 4: Sections from the parathyroid gland show proliferation of chief cells arranged in sheets with reduced stromal fat, consistent with parathyroid adenoma/hyperplasia. Sections from the fracture site show fibrovascular stroma with numerous multinucleated osteoclast-type giant cells, areas of hemorrhage, and hemosiderin-laden macrophages.
Features are suggestive of a brown tumour in the setting of hyperparathyroidism. The post-operative course was uneventful. Serial monitoring of serum calcium levels demonstrated normalisation. The patient was discharged on calcium and vitamin D supplementation, with advice for regular follow-up. Immediate post-operative anteroposterior and lateral radiographs of the right humerus demonstrate stable fixation of the pathological fracture using an intramedullary interlocking humeral nail with satisfactory alignment (Fig. 5). One-year post-operative radiographic follow-up of the right humerus and femur. Anteroposterior and lateral views showing stable intramedullary fixation with satisfactory alignment and consolidation at the fracture site. There is radiological evidence of healing without implant-related complications or progression of underlying osteolytic pathology (Fig. 6).
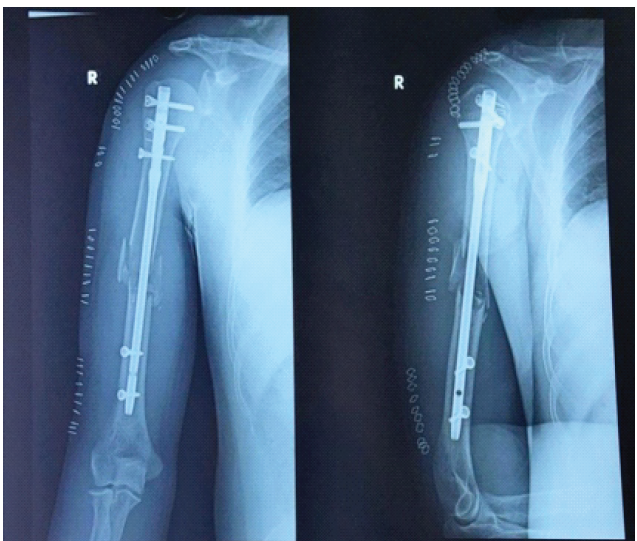
Figure 5: Immediate post-operative radiographs (anteroposterior and lateral views) showing intramedullary interlocking nail fixation of the humeral shaft with satisfactory alignment.

Figure 6: One-year post-operative radiographic follow-up of the right humerus and femur. Anteroposterior and lateral views showing stable intramedullary fixation with satisfactory alignment and consolidation at the fracture site. There is radiological evidence of healing without implant-related complications or progression of underlying osteolytic pathology.
Brown’s tumour represents a severe skeletal consequence of prolonged hyperparathyroidism and corresponds to the advanced stage of osteitis fibrosa cystica. Although historically more common, its incidence has significantly declined in modern clinical practice due to early biochemical screening, and it is now reported in less than 5% of patients with primary hyperparathyroidism [1,2,3]. However, recent literature – including case reports and retrospective series – suggests that it continues to be encountered in developing regions where delayed diagnosis, poor access to healthcare, and vitamin D deficiency are prevalent [2,4]. In comparison to available literature, the present case demonstrates several clinically significant features. First, involvement of the humeral shaft is relatively uncommon. Most reported cases in the literature describe lesions in the mandible, ribs, pelvis, and long bones such as the femur [5,6]. Upper limb involvement, particularly presenting as a pathological fracture, is less frequently reported, thereby increasing the risk of misdiagnosis. Similar cases described in orthopaedic and endocrine literature highlight that atypical locations often lead clinicians toward an initial diagnosis of primary bone tumours or metastatic lesions [7,8]. Radiologically, Brown’s tumours typically demonstrate well-defined expansile osteolytic lesions with cortical thinning and absence of periosteal reaction. These features overlap significantly with giant cell tumour, aneurysmal bone cyst, and metastatic bone disease. Hong et al. [5] emphasised that imaging findings alone are insufficient for differentiation, as magnetic resonance imaging and computed tomography characteristics are non-specific. This diagnostic overlap was evident in the present case, where the solitary humeral lesion with fracture could have been easily misdiagnosed as a primary neoplasm based on imaging alone. Histopathological findings also lack specificity. The presence of multinucleated osteoclast-type giant cells within a fibrovascular stroma, along with areas of haemorrhage and hemosiderin deposition, is characteristic but not pathognomonic. Similar features are observed in giant cell tumours and other giant cell–rich lesions. As highlighted by De Crea et al. [7], reliance on histology without biochemical correlation may result in misdiagnosis and inappropriate treatment. In the present case, definitive diagnosis was achieved only after correlating histopathological findings with markedly elevated serum calcium and parathyroid hormone levels. A key distinguishing aspect of this case, when compared with previously published JOCR and indexed reports, is the presence of multifocal skeletal involvement combined with prior mandibular pathology, suggesting a long-standing, undiagnosed metabolic disorder. Similar patterns have been described in case reports by Vanitcharoenkul et al. [6], where pathological fractures were the initial presenting feature of hyperparathyroidism. Such presentations underscore the importance of considering metabolic aetiologies in patients with multiple lytic lesions. Another critical point of comparison relates to management strategies. Current literature consistently identifies correction of the underlying hyperparathyroidism as the cornerstone of treatment. Studies have demonstrated that following parathyroidectomy, many Brown’s tumours regress spontaneously due to normalisation of bone turnover [2,5]. However, orthopaedic intervention becomes necessary in cases of pathological fracture, impending fracture, or significant functional limitation. The timing of surgical fixation relative to endocrine correction remains a subject of discussion. Several authors advocate initial metabolic stabilisation before orthopaedic intervention to minimise complications such as hypercalcaemic crisis and postoperative hungry bone syndrome [6,9]. In contrast, some reports suggest simultaneous or early fixation in unstable fractures. In our case, a staged approach was adopted, with metabolic stabilisation followed by intramedullary fixation, resulting in favourable functional and radiological outcomes. This approach aligns with the majority of contemporary recommendations and supports the importance of individualised, multidisciplinary planning. Importantly, failure to recognise Brown’s tumour as a metabolic condition has been associated with unnecessary aggressive surgical procedures, including wide excision and even amputation, as reported in earlier literature [7,8,10]. This highlights a major clinical implication – orthopaedic surgeons must maintain a high index of suspicion, particularly in young patients with atypical lytic lesions and pathological fractures. From a broader perspective, this case reinforces three critical learning points in comparison with existing literature:
- Biochemical evaluation is indispensable in all cases of lytic bone lesions
- Histopathology alone is insufficient for definitive diagnosis
- Multidisciplinary management significantly improves outcomes.
Brown’s tumour should be considered in the differential diagnosis of expansile lytic bone lesions, particularly in young patients presenting with pathological fractures. Routine biochemical evaluation is essential before labelling such lesions as primary bone tumours. Management of the underlying hyperparathyroidism combined with appropriate orthopaedic stabilisation results in favourable outcomes.
Biochemical evaluation is mandatory in all pathological fractures to identify underlying metabolic bone disorders and prevent misdiagnosis.
References
- 1. Karaca MO, Özyıldıran M, Savran MD, Başarır K, Yıldız HY. Brown tumours: Retrospective analysis of 26 cases. Arch Orthop Trauma Surg 2024;144:2927-34. [Google Scholar] [PubMed]
- 2. Minisola S, Gianotti L, Bhadada S, Silverberg SJ. Classical complications of primary hyperparathyroidism. Best Pract Res Clin Endocrinol Metab 2018;32:791-803. [Google Scholar] [PubMed]
- 3. Walker MD, Bilezikian JP. Primary hyperparathyroidism: Recent advances. Curr Opin Rheumatol 2018;30:427-39. [Google Scholar] [PubMed]
- 4. Misiorowski W, Czajka-Oraniec I, Kochman M, Zgliczyński W, Bilezikian JP. Osteitis fibrosa cystica – a forgotten radiological feature of primary hyperparathyroidism. Endocrine 2017;58:380-5. [Google Scholar] [PubMed]
- 5. Hong WS, Sung MS, Chun KA, Kim JY, Park SW, Lee KH, et al. Emphasis on the MR imaging findings of brown tumours: A report of five cases. Skeletal Radiol 2011;40:205-13. [Google Scholar] [PubMed]
- 6. Vanitcharoenkul E, Singsampun N, Unnanuntana A, Sirinvaravong S. Osteitis fibrosa cystica and pathological fractures – the classic but neglected skeletal manifestation of primary hyperparathyroidism: A case report. BMC Musculoskelet Disord 2021;22:443. [Google Scholar] [PubMed]
- 7. De Crea C, Traini E, Oragano L, Bellantone C, Raffaelli M, Lombardi CP. Are brown tumours a forgotten disease in developed countries? Acta Otorhinolaryngol Ital 2012;32:410-15. [Google Scholar] [PubMed]
- 8. Guliaeva SS, Voloshchuk IN, Mokrysheva NG. Misdiagnosis of a giant cell tumour of the bone in a patient with hyperparathyroid osteodystrophy. Arkh Patol 2009;71:53-5. [Google Scholar] [PubMed]
- 9. Witteveen JE, Van Thiel S, Romijn JA, Hamdy NA. Hungry bone syndrome: Still a challenge in the post-operative management of primary hyperparathyroidism: A systematic review of the literature. Eur J Endocrinol 2013;168:R45-53. [Google Scholar] [PubMed]
- 10. Wang X, Wang C, Gao Y. Humeral brown tumour as first presentation of primary hyperparathyroidism caused by ectopic parathyroid adenoma. BMJ Case Rep. 2014;2014:bcr2014205754. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Incidental Found Fungal Growth in a Suspected Case of Fibrous Dysplasia of Left Shoulder: Case Report
June 1, 2025 Incidental Found Fungal Growth in a Suspected Case of Fibrous Dysplasia of Left Shoulder: Case Report January 10, 2024 Primary Hyperparathyroidism Mimicking Skeletal Metastasis – A Diagnostic Dilemma
January 10, 2024 Primary Hyperparathyroidism Mimicking Skeletal Metastasis – A Diagnostic Dilemma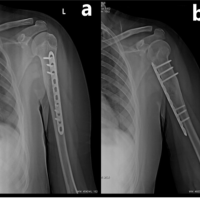 August 10, 2022 Management of a Displaced Pathological Fracture in the Proximal Humerus of a Patient with Autism Spectrum Disorder: A Rare Case Report
August 10, 2022 Management of a Displaced Pathological Fracture in the Proximal Humerus of a Patient with Autism Spectrum Disorder: A Rare Case Report June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes
June 1, 2026 Intralesional Triamcinolone versus Oral Bisphosphonate for Benign Cystic Bone Lesions: A Prospective Comparative Study of Radiological and Pain Outcomes