
This case series provides clinical and radiographic findings used to identify Brodie’s abscess of the distal tibia, which is a rare pathology that is commonly mistaken as a tumor upon initial presentation.
Dr. Christopher Warburton, Medical Student, University of Miami Miller School of Medicine, BS, 1400 NW 12th Avenue, Suite 3046 Miami, Florida, United States. E-mail: cswarburton@med.miami.edu
Abstract
Introduction: A Brodie’s abscess is a form of subacute osteomyelitis that is often considered in the differential diagnosis of other benign and malignant bone lesions. The authors summarize the findings of five cases of Brodie’s abscesses in the distal tibia initially thought to be tumors by the referring physicians.
Case Report: All five cases were presented to the referring physicians with a chief complaint of ankle pain. All patients complained of chronic ankle pain and swelling that was aggravated by activity without constitutional symptoms. On physical examination, all patients presented with point tenderness over the distal tibia/malleolar regions. Three out of the five cases had a full range of ankle motion; the other two had limited dorsiflexion secondary to pain. All inflammatory laboratory values were within normal limits or only slightly elevated. All initial radiographs of the cases described demonstrated a well-defined radiolucent lesion within the distal tibia. In all cases, patients were treated with curetting, with or without bone graft. Bacterial and fungal cultures were negative in all five patients and no long-term post-operative antibiotics were administered.
Conclusion: In this report, we discuss the clinical, radiographic, and pathologic features of this relatively rare condition in the distal tibia. The distinct clinicopathologic features of the disease process are presented to distinguish Brodie’s abscess from a bone tumor.
Keywords: Subacute osteomyelitis, Brodie’s abscess, osteomyelitis, tibia, Staphylococcus infections, abscess, bone diseases.
In 1832, Sir Benjamin Brodie described the first reported case of a special form of osteomyelitis with an indolent course and no prior history of an acute infection. He described these observations and the characteristic pathology after a lower extremity amputation for a suspected tumor [1]. A Brodie’s abscess is thought to be a form of subacute hematogenous osteomyelitis. The diagnosis can be difficult in some cases and treatment is still controversial. We present and summarize the clinical and radiographic features as well as the treatment of five patients with a Brodie’s abscess of the distal tibia thought to be a tumor by referring orthopedic foot and ankle surgeons. The distinct clinicopathologic features of the disease process are presented to distinguish Brodie’s abscess from a bone tumor.
All cases of Brodie’s abscess were reviewed from the orthopedic oncology database at our institution to identify only those cases in the distal tibia. Patient demographics, clinical, radiographic, and microscopic features of these subjects were recorded and analyzed. Institutional review board approval was obtained. We identified five patients with Brodie’s abscess of the distal tibia. There were three women and two men with a mean age of 22.4 years (8–52). The mean duration of symptoms before diagnosis was 5.2 months (3–8 months) and all patients had pain and swelling as the presenting symptoms; three of five had nocturnal pain and none had constitutional symptoms. The mean follow-up was 3.6 years (2–6 years).
Case 1
A 52-year-old female presented with an 8-month history of right ankle pain. The pain was present both at night and rest and was aggravated with ambulation. There was no history of fever or other constitutional symptoms. Her past medical history was significant for colorectal carcinoma and cervical cancer diagnosed and treated 10 and 14 years earlier, respectively. She had sustained an ankle sprain 2 years before the presentation. On physical examination, there was a full range of motion of the ankle without edema, swelling, or erythema. She had localized tenderness to palpation along the medial malleolus. Her white blood cell count was within normal limits with a differential of 57% neutrophils. Radiographs demonstrated a small geographic subchondral radiolucency on the posteromedial aspect of the distal tibial epiphysis (Fig. 1a). The lesion had well-defined margins, without bone production, cortical destruction, periosteal reaction, or soft tissue shadows. A Technetium-99 (Tc-99) pyrophosphate bone scan demonstrated increased radiotracer uptake around the posteromedial aspect of the distal tibia (Fig. 1b). A subsequent magnetic resonance imaging (MRI) showed a well-defined lesion with a characteristic central area of homogenous, hypointensity on T1-weighted images (Fig. 1c), and hyperintense signal on T2-weighted images, with no associated soft-tissue mass. Based on the clinical and radiographic features of the lesion, subacute osteomyelitis was considered and a tumor was thought to be unlikely. The patient underwent open biopsy and curetting without bone grafting. Histology confirmed the diagnosis to be a Brodie’s abscess. The Gram stain and cultures were negative and no antibiotics were given postoperatively. At the final follow-up 2 years and 10 months after surgery, the patient remained asymptomatic.
The lesion had well-defined margins, without bone production, cortical destruction, periosteal reaction, or soft tissue shadows. A Technetium-99 (Tc-99) pyrophosphate bone scan demonstrated increased radiotracer uptake around the posteromedial aspect of the distal tibia (Fig. 1b). A subsequent magnetic resonance imaging (MRI) showed a well-defined lesion with a characteristic central area of homogenous, hypointensity on T1-weighted images (Fig. 1c), and hyperintense signal on T2-weighted images, with no associated soft-tissue mass. Based on the clinical and radiographic features of the lesion, subacute osteomyelitis was considered and a tumor was thought to be unlikely. The patient underwent open biopsy and curetting without bone grafting. Histology confirmed the diagnosis to be a Brodie’s abscess. The Gram stain and cultures were negative and no antibiotics were given postoperatively. At the final follow-up 2 years and 10 months after surgery, the patient remained asymptomatic.
Case 2
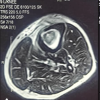
An 18-year-old male presented with a 6-month history of pain in his right ankle. The pain was intermittent, aggravated by weight-bearing activity, and present at night as well. The swelling was noted to occur periodically. No constitutional symptoms were present. On physical examination, there was no significant edema, discoloration, or joint effusion. There was a full active and passive range of motion of the ankle. He had mild tenderness to palpation over the anterior aspect of the distal tibia. The white blood cell count was 7000 cells/µL with a differential of 67.9% neutrophils. Radiographs revealed a serpiginous, radiolucent abnormality in the distal tibial metadiaphysis with well-defined, sclerotic margins (Fig. 2a and b).

No bone production, cortical disruption, periosteal reaction, or soft-tissue shadows were noted. The bone scan showed intense and homogeneous uptake in the right distal tibia. MRI showed a characteristic fluid signal within the lesion (Fig. 2c) and rim enhancement on T1-weighted post-gadolinium images (Fig. 2d). Again, based on the clinical and radiographic features of the lesion, a probable diagnosis of Brodie’s abscess was made. The patient underwent an open biopsy and thorough curetting without a bone graft. A biopsy confirmed the diagnosis of a Brodie’s abscess. Intraoperative cultures were negative and no antibiotics were administered. Three years later the patient remained asymptomatic.
Case 3
A 22-year-old male presented with a 3-month history of progressive left ankle pain occurring with activity and at rest. In addition, the patient complained of pain at night that occasionally awoke him from sleep. The patient denied any other constitutional symptoms. On physical examination, there was mild swelling and tenderness to palpation around the distal tibia, but no warmth or erythema. There was a full range of motion at the ankle joint. The patient’s white blood cell count and differential were normal. Radiographs of the ankle demonstrated a radiolucent lesion in the distal tibial epiphysis with well-defined sclerotic margins (Fig. 3a). There was no bone production, cortical destruction, periosteal reaction, or soft-tissue shadows. The computed tomography scan showed a low attenuation abnormality that better delineated the serpiginous borders of the lesion, and also confirmed the absence of bone production, periosteal reaction, or soft-tissue masses (Fig. 3b). An open biopsy and thorough curetting without bone graft were performed and histology showed findings similar to those seen in chronic osteomyelitis; specifically, empty lacunae and the presence of chronic inflammatory cells and granulation tissue were seen (Fig. 4). Multiple intraoperative samples sent for culture remained negative and antibiotics were withheld. The patient’s pain resolved after surgery and he remained asymptomatic for 6 years, after which he was lost to follow-up.
Case 4
A 12-year-old female presented with a 3-month history of progressive left ankle pain present with activity and rest. She denied constitutional symptoms but had a remote history of a Staphylococcus infection in her cervical region 11 years prior. On physical examination, there was mild swelling and tenderness over her posterolateral ankle with limited dorsiflexion of her ankle secondary to pain. Laboratory values were all normal. Radiographs demonstrated a geographic, radiolucent abnormality in the posterolateral aspect of the distal tibia, without periosteal reaction or matrix production. An open biopsy with extended curetting and bone grafting using particulate bone was performed. A histologic evaluation confirmed the diagnosis of a Brodie’s abscess and intraoperative cultures remained negative. No intravenous or oral antibiotics were used. On final evaluation 2 years later, she remained asymptomatic.
Case 5
An 8-year-old female presented with 6 weeks of mild episodic right ankle pain after an insignificant fall. She was referred with a radiographic abnormality thought to be an aggressive benign or malignant bone tumor. On physical examination, there was mild tenderness over the anterolateral distal tibia and pain with passive dorsiflexion. Laboratory evaluation revealed a white blood cell count of 12.1 and an erythrocyte sedimentation rate (ESR) of 29 mm/h. Radiographs showed a geographic, radiolucent lesion in the anterolateral distal tibia, without periosteal reaction or matrix production. MRI imaging showed a homogeneous, hypointense signal on T1-weighted images with a surrounding rim of relative hypointensity. On T2-weighted images, a homogeneous hyperintense signal was present consistent with an abscess. There was rim enhancement on T1-weighted images following gadolinium administration. Based on the clinical and radiographic findings, a diagnosis of a Brodie’s abscess was made and the patient underwent an open biopsy and extended curetting. The histologic examination was consistent with Brodie’s abscess, cultures remained negative and no intravenous or oral antibiotics were given. Eighteen months after her procedure she remained asymptomatic with radiographic evidence of consolidation of the lesion.
Summary of five cases
All five cases of Brodie’s abscess at this institution were presented to the orthopedic oncology department by referring physicians due to concerns of a tumor or malignancy. All patients complained of chronic ankle pain and swelling that was aggravated by activity without constitutional symptoms. Two of the cases had a history of mild ankle trauma to the affected ankle. One patient reported a history of a Staphylococcus infection of the cervical region over a decade before presentation. On physical examination, all patients presented with point tenderness over the distal tibia/malleolar regions. Three out of the five cases had a full range of ankle motion; the other two had limited dorsiflexion secondary to pain. On laboratory evaluation only one patient presented with a mild elevation of white blood cell count of 12,100 cells/µL. The rest had white blood cell quantities within normal limits. Only one patient presented with a left shift of neutrophils of 67.9%, although they had a normal white blood cell count value of 7000 cells/µL. Only one patient had an elevated ESR of 29 mm/h. All initial radiographs of the cases described demonstrated a well-defined radiolucent lesion within the distal tibia, as exemplified in Figs. 1a, 2a, and b. The precise location of the lesion was either within the epiphysis or metadiaphysis. All lesions were without bone production, cortical destruction, periosteal reaction, or soft-tissue shadows. Two cases demonstrated serpiginous borders of the lesion (Fig. 2 and 3). Three lesions were further evaluated through MRI and demonstrated similar imaging characteristics. T1-weighted images all showed a well-defined lesion with a characteristic central area of homogenous, hypointensity. Rim enhancement was seen on T1-weighted images following gadolinium administration. T2-weighted imaging showed a homogenous hyperintense signal, which is more consistent with an abscess versus a soft-tissue mass. One case was further evaluated through computed tomography (CT). CT imaging showed a low attenuation abnormality that better delineated the serpiginous borders of the lesion, and also confirmed the absence of bone production, periosteal reaction, or soft-tissue masses, as seen in Fig. 3b. After these initial studies and clinical pictures, Brodie’s abscess was the most likely diagnosis in all the cases. Biopsies were obtained from each case, and histological examination confirmed the diagnosis, which showed findings similar to those seen in chronic osteomyelitis. The evaluation revealed empty lacunae and the presence of chronic inflammatory cells and granulation tissue. An example of the histology can be seen in Fig. 4. Bacterial and fungal cultures were negative in all five patients and no long-term post-operative antibiotics were administered in any case.

Brodie’s abscess is a unique form of hematogenous osteomyelitis with a subacute and indolent course. This presumed blood–borne infection results in a well-contained abscess surrounded by granulation tissue and reactive bone. They primarily occur in the long bones of the appendicular skeleton, but may also be found in the axial skeleton and tarsal bones. Two factors are thought to contribute to the formation of this localized subacute process; (1) an intact host immune system and (2) low bacterial virulence [2]. The most commonly affected areas are the long bones of the lower extremity with the proximal metaphysis of the tibia being the most common site [2-5]. In the largest reported series of subacute osteomyelitis, the distal tibial metaphysis was the third most common location, comprising 22 of 181 cases [3]. Like acute hematogenous osteomyelitis, there is a predilection for the metaphysis which can be attributed to the unique vascularization of the area [6]. Other locations of subacute osteomyelitis have been recognized as well in metaphyseal-equivalent locations. Gledhill classified lesions by location and appearance into four types. Type I or Brodie’s abscess is a solitary, localized radiolucency surrounded by reactive new bone, usually metaphyseal but may extend into the epiphysis. Type II are metaphyseal lesions associated with a loss of cortical bone. Type III lesions are diaphyseal with excessive cortical reaction. Type IV lesions are associated with onion skin layering of subperiosteal bone which may mimic early Ewing sarcoma [7]. Roberts expanded the classification to include lesions in the epiphysis and vertebrae [8]. King and Mayo found that extension of Gledhill type I Brodie’s abscess lesions into the epiphysis was common and helpful diagnostically, but in some cases, only evident on tomography [2]. These infections are more common in males than females. Patients are usually in the second decade of life and the incidence progressively decreases with age. Positive cultures for Staphylococcus were reported in 50–78% of cases and negative cultures were observed in 20% of cases, in two large reviews [3,5]. However, our experience, as well as several recent reviews suggests a lower incidence of positive cultures [9,13]. Clinical features are usually subtle, in contrast to acute osteomyelitis, where an acute history of pain, elevated temperature, and loss of function are apparent. Subacute osteomyelitis typically presents with deep bone pain occurring for a prolonged period (months to years) which is consistent with the duration of symptoms that the patients in this study experienced. Occasional, intermittent soft-tissue swelling is also seen with absent fever and malaise. The common finding of night pain may raise suspicion for a neoplastic disease process. On physical examination, local tenderness is consistently reported and was seen in all of our cases. Soft-tissue swelling may be present. Normal joint function is generally seen. The white blood cell count is usually normal and the ESR is commonly elevated and may correlate with disease severity and likelihood of recurrence [7]. Of interest, only one patient at our institution had an elevated ESR, and the same patient had a slightly elevated white blood cell count. Blood cultures are almost always negative and were negative in the cases presented in this study [2,3,5,7]. Histological evaluation reveals changes typically observed in patients with chronic osteomyelitis. Empty lacunae and the presence of chronic inflammatory cells and granulation tissue are seen [2,3,5,13]. Radiographic evaluation is often the most helpful diagnostic tool in making the correct diagnosis. Radiographs, though non-specific, usually reveal a geographic, radiolucent lesion with moderately well or well-defined edges, without soft-tissue mass, bone production, cortical destruction, or osseous expansion [14]. Three-phase Tc-99 bone scans usually show increased radiotracer uptake on delayed images in the affected area, as seen in the one patient who obtained a bone scan in this series of patients (Fig. 1b). Because of the low specificity of bone scan, its utility may be limited to cases where multiple sites of involvement are suspected. Computerized tomography may be helpful in better delineating the lesion. As seen in two of the cases at our institution, a serpiginous border may be identified, which is a characteristic feature of a Brodie’s abscess, and is exemplified in Fig. 3 [15]. Supplementation with MRI with gadolinium enhancement has been reported to increase the likelihood of accurate diagnosis of subacute osteomyelitis [16]. MRI of a Brodie’s abscess has a characteristic four-layer appearance consisting of an abscess cavity, inner ring of granulation tissue, marrow edema, and surrounding bony sclerosis [17]. The presence of an inner ring or “penumbra” sign on T1 images may be particularly helpful. It is described as a discrete relatively hyper-intense area between the central abscess cavity and surrounding marrow edema and sclerosis (Fig. 2d). This was reported to be 75% sensitive and 99% specific in a review of 32 cases of histologically proven Brodie’s abscesses. However, the “penumbra” sign is not pathognomonic and was present in only of case of a chondrosarcoma in this study [18]. The penumbra sign was present in two of the five cases in our study. Gadolinium enhancement is also useful in diagnosing a Brodie’s abscess. Unlike the central fluid portion, the surrounding highly vascular granulation tissue often enhances after administration as seen in Fig. 4. These sequences may also be helpful in identifying concomitant fistula tracts. Treatment has traditionally been open biopsy, curetting, and 6 weeks of intravenous antibiotics [19]. Cancellous bone packing is also recommenced with lesions >3 cm. Recently, non-operative treatment with only antibiotics has been suggested as an option [20,21]. There are no series that systematically evaluate surgical treatment alone in the presence of culture-negative abscesses. Gledhill reported two of eight cases were treated only surgically with a resolution of the disease without antibiotics [7]. We have observed that this disease is indolent and that intralesional surgery can be performed in a minimally invasive manner with or without a bone graft. Prolonged antibiotic therapy should be withheld in cases of Brodie’s abscesses with negative cultures.
A Brodie’s abscess although relatively rare, has distinct clinical and radiographic features that help differentiate it from other benign and malignant osseous lesions. It should be emphasized that a true Brodie’s abscess, in the absence of prior antibiotic therapy, indicates a favorable host immune response over the offending pathogen. While our experience suggests surgical treatment alone without post-operative antibiotics in cases of culture-negative abscesses is sufficient, we recognize that larger studies may be necessary to make definitive treatment recommendations.
When a patient presents with an unknown cause of subacute to chronic ankle pain with or without subtle clinical findings such as soft-tissue swelling, Brodie’s abscess should be included on the differential diagnosis. Although many referring physicians will associate the initial radiographic and clinical findings with neoplastic disease, further imaging along with histopathological analysis can differentiate the ankle lesion as a Brodie’s abscess, which is a much more benign condition compared to a tumor.
References
- 1.Brodi BC. An account of some cases of chronic abscess of the tibia. Med Chir Trans 1832;17:239-49. [Google Scholar | PubMed]
- 2.King DM, Mayo KM. Subacute hematogenous osteomyelitis. J Bone Joint Surg 1969;51B:458-63. [Google Scholar | PubMed]
- 3.Boriani S. Brodie’s abscess-a study of 181 cases, with special reference to radiographic diagnostic criteria. Ital J Orthop Trauma 1980;6:373-83. [Google Scholar | PubMed]
- 4.Harris NH, Kirmaldy-Willis WH. Primary subacute pyogenic osteomyelitis. J Bone Joint Surg 1965;47B:526-32. [Google Scholar | PubMed]
- 5.Stephans MM, MacAuley P. Brodie’s abscess-a long term review. Clin Orthop Relat Res 1987;234:211-6. [Google Scholar | PubMed]
- 6.Schenk RK, Wiener JS, Spiro D. Fine structural aspects of vascular invasion of the tibial epiphyseal plate of growing rats. Acta Anat 1968;69:1-17. [Google Scholar | PubMed]
- 7.Gledhill RB. Subacute osteomyelitis in children. Clin Orthop 1976;96:57-69. [Google Scholar | PubMed]
- 8.Roberts JM, Drummond DS, Breed AL, Chesney J. Subacute hematogenous osteomyelitis in children: A retrospective study. J Pediatr Orthop 1982;2:249-54. [Google Scholar | PubMed]
- 9.Cole WG. The management of chronic osteomyelitis. Clin Orthop 1991;264:84-9. [Google Scholar | PubMed]
- 10.Gamble JG, Rinsky LA. Chronic recurrent multifocal osteomyelitis: A distinct clinical entity. J Pediatr Orthop 1986;6:579-84. [Google Scholar | PubMed]
- 11.Green NE, Beauchamp RD, Griffin PP. Primary subacute epiphyseal osteomyelitis. J Bone Joint Surg 1981;63A:107-14. [Google Scholar | PubMed]
- 12.Hoffman EB, de Beer JD, Keys G, Anderson P. Diaphyseal primary subacute osteomyelitis in children. J Pediatr Orthop 1990;10:250-4. [Google Scholar | PubMed]
- 13.Rasool MN. Primary subacute hematogenous osteomyelitis in children. J Bone Joint surg 2001;83B:93-8. [Google Scholar | PubMed]
- 14.Lopez TD, Reinus WR, Wilson AJ. Quantitative analysis of the plain radiographic appearance of Brodie’s abscess. Invest Radiol 1997;32:51-8. [Google Scholar | PubMed]
- 15.Letts RM. Subacute osteomyelitis in children. In: Current Concepts of Infections on Orthopaedic Surgery. Germany: Springer-Verlag; 1985. p. 141-9. [Google Scholar | PubMed]
- 16.Boutin RD, Brossmann J, Sartoris DJ, Reilly D, Resnick D. Musculoskeletal imaging update, part II-update on imaging of orthopedic infection. Orthop Clin North Am 1998;29:41-66. [Google Scholar | PubMed]
- 17.Marti-Bonmati L, Aparisi F, Poyatos C, Vilar J. Brodie abscess: MR imaging appearance in 10 patients. J Magn Reson Imaging 1993;3:543-6. [Google Scholar | PubMed]
- 18.Grey AC, Davies AM, Mangham DC, Grimer RJ, Ritchie DA. The “penumbra sign” on T1-weighted MR imaging in subacute osteomyelitis: Frequency, cause and significance. Clin Radiol 1998;53:587-692. [Google Scholar | PubMed]
- 19.Alter SA, Sprinkle RW. Brodie’s abscess: A case report. J Foot Ankle Surg 1995;34:208-14. [Google Scholar | PubMed]
- 20.Ezra E, Cohen N, Segec E, Hayek S, Lokiec F, Keret D, et al. Primary subacute epiphyseal osteomyelitis: Role of conservative treatment. J Pediatr Orthop 2002;22:333-7. [Google Scholar | PubMed]
- 21.Hamdy RC, Lawton L, Carey T, Wiley J, Marton D. Subacute hematogenous osteomyelitis: Are biopsy and surgery always indicated? J Pediatr Orthop 1996;16:220-3. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Primary Tuberculous Osteomyelitis of the Proximal Tibia Presenting as Chronic Osteomyelitis: A Diagnostic Challenge in Musculoskeletal Tuberculosis
August 1, 2026 Primary Tuberculous Osteomyelitis of the Proximal Tibia Presenting as Chronic Osteomyelitis: A Diagnostic Challenge in Musculoskeletal Tuberculosis September 10, 2021 Brodie’s Abscess of the Proximal Humerus Metaphysis: A Case Report
September 10, 2021 Brodie’s Abscess of the Proximal Humerus Metaphysis: A Case Report August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report
August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report August 1, 2026 Oblique Plane Deformity Correction with Ilizarov Fixator in Ipsilateral Proximal Tibia Growth Arrest and Malunited Tibia: A Case Report
August 1, 2026 Oblique Plane Deformity Correction with Ilizarov Fixator in Ipsilateral Proximal Tibia Growth Arrest and Malunited Tibia: A Case Report