
Early diagnosis, appropriate surgical intervention, and prompt rehabilitation are crucial for managing complex wrist injuries like the “floating wrist” to achieve satisfactory functional outcomes.
Dr. Abaydi Anass, Department A of Traumatology and Orthopedic Surgery, Hassan 2 University Hospital Center, Sidi Mohamed Ben Abdellah University, Fez, Morocco. E-mail: anass.abaydi@usmba.ac.ma
Introduction: Joint injuries in the upper limb are uncommon and have received limited attention in the literature. This case report presents the first described case in the literature of a “floating wrist” and aims to highlight the diagnostic, anatomical, and therapeutic aspects of this injury.
Case Report: A 27-year-old male was involved in a severe car accident, resulting in a closed deformity of the right wrist. The patient suffered fractures of the forearm bones and dislocation fracture of all five wrist rays. Surgical intervention was performed to repair the fractures and stabilize the wrist. Despite post-operative complications, the patient demonstrated positive functional outcomes after a 12-month follow-up.
Discussion: The term “floating wrist” refers to a rare condition characterized by fractures and/or dislocations of all five wrist rays, accompanied by fractures of the forearm bones. Diagnosis can be complicated due to polytrauma and wrist edema. Early surgical management and rehabilitation are essential for achieving favorable outcomes. Further research is necessary to improve our understanding of this uncommon injury.
Conclusion: This case report highlights a unique instance of a “floating wrist” and emphasizes the significance of early diagnosis, appropriate surgical intervention, and prompt rehabilitation in a comprehensive management of these complex injuries. Enhanced comprehension of this rare condition is crucial for improving patient outcomes in similar traumatic scenarios.
Keywords: Floating wrist, fractures of the forearm bones, distal radius and ulna fractures, dislocation fracture of the five metacarpal bones, dislocation fracture of the five wrist rays, carpometacarpal dislocation, radio-clinical diagnosis, surgical intervention, rehabilitation, functional outcomes.
The term “floating” in medical terminology refers to a body part that is not in continuity with its adjacent structures [1]. This phenomenon can occur due to various reasons, including trauma, surgical interventions, or congenital anomalies. Floating injuries represent a significant challenge in clinical practice due to their complexity and the potential for severe functional impairment [2]. Fractures and dislocations involving the wrist and forearm are among the most complex orthopedic injuries. The wrist is a highly intricate joint, composed of multiple bones, ligaments, and tendons, all working together to facilitate a wide range of motion and dexterity. Injuries to this area can have profound implications on hand function and overall quality of life. In this article, we present a unique case of a “floating wrist” in a patient, which, to the best of our knowledge, has not been reported before in the existing medical literature in both French and English publications. This study aims to discuss the diagnostic challenges, anatomical considerations, and therapeutic strategies associated with this rare and complex injury. By sharing this case, we hope to contribute to the body of knowledge and improve the management and outcomes for similar cases in the future.
We report the case of a right-handed 27-year-old male, working as a bus driver, with no significant medical history, who was admitted to the emergency department following a severe polytrauma resulting from a motor vehicle collision involving two cars, with three fatalities on the scene. On admission, the patient presented with an altered Glasgow Coma Scale score and hemodynamic instability, necessitating stabilization and intubation based on neurological criteria. Initial clinical examination revealed a closed deformity of the right wrist associated with significant swelling and absence of palpable radial and ulnar pulses. After the patient was hemodynamically stabilized, a total body computed tomography (CT) scan and CT angiography were performed, revealing multiple contusions in the brain, chest, and abdomen. Radiological evaluation of the right upper limb showed fractures involving both bones of the forearm, affecting the distal quarter of the radius and ulna with posterior and lateral displacement. In addition, there was a comminuted fracture of the neck of the second metacarpal bone with dislocation of the first, third, and fourth rays of the hand with dorsal radial translation and fifth metacarpal bones volair and radial displacement (Fig. 1). Angiography of the right upper limb revealed a dissection of the radial artery adjacent to the fracture.
The patient was taken to the operating room for surgical intervention 5 h following the accident, after stabilization. The first step involved repairing the forearm bone fractures. We opted for an anterior approach using the Henry technique to reduce and stabilize the radius fracture with a 7-hole DCP plate. A double K-wire of the radial styloid under fluoroscopic control was also performed through the same approach, as well as a preventive neurolysis of the median nerve. The second step involved a posterior approach centered on the ulnar crest to reduce and stabilize the ulna fracture using a 7-hole neutralization plate. The third step focused on vascular repair of the radial artery by vascular surgeons; exploration of the ulnar artery revealed no anomalies.
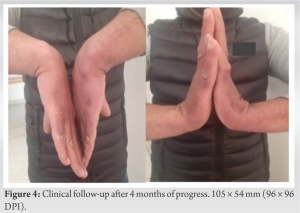
Finally, the fourth step involved closed reduction of the trapeziometacarpal dislocation of the thumb, which was stable after reduction. An open longitudinal dorsal approach on the ulnar border of the second metacarpal bone and on the radial border of the fifth metacarpal bone allowed for an open reduction of the carpometacarpal dislocation, which was stabilized with three Kirschner wires passing through the base of the fifth, fourth, and third metacarpals and pressing against the carpal bones. An axial pinning of the second metacarpal bone was also performed, and given the severity of the injuries, a lateral-medial transverse pinning of the second, third, and fourth metacarpals was carried out. Immobilization through a plaster cast using a brachial antebrachial palmar immobilizing the thumb with a free interphalangeal joint (Fig. 2) after surgery, the patient was admitted into the intensive care unit for close monitoring. Within 24 h, he developed severe respiratory distress, requiring a thoracic CT angiography. Results revealed an aneurysm of the aortic isthmus, for which a vascular endoprosthesis was successfully implanted. The patient remained hospitalized for 24 days until his condition improved and he could be discharged. Three weeks after surgery, an elbow release was performed, followed by rehabilitation sessions for the elbow. At the 4th week, the cast was removed and rehabilitation of the wrist and fingers began, with the patient wearing a splint between sessions for 2 weeks. At the 6th week, the patient returned to our service for the removal of the wires from the metacarpal and carpometacarpal bones (Fig. 3). Rehabilitation protocols were continued. After a follow-up period of 12 months, the functional outcome of the surgery was satisfactory. The patient had no pain, and the fractural healing was observed. Muscle strength was good (90% compared to the unaffected side), and the patient regained complete mobility of the wrist, with flexion at 80°, extension at 80°, ulnar deviation at 25°, and radial deviation at 10°. Finger flexion was almost normal, with no neurological sequelae affecting the median ulnar nerves. A shortening of the length of the second finger was observed during the “Indian salute” test (Fig. 4). The patient was able to return to work 4 months later.
In medical terminology, the term “floating” refers to a body part that is not in continuity with its adjacent structures, which can occur due to various reasons such as trauma, surgical interventions, or even congenital anomalies. The term was first used by Baudens to describe a fracture of the distal end of the ulna, which became detached from the rest of the forearm [1]. Sappey also used this term to describe the clavicle, which is connected only by the surrounding muscles and ligaments and not firmly attached to the sternum, and can occur due to a fracture or congenital malformation [2]. This study focuses on the term “floating wrist” to describe a specific fracture entity in the patient, which combines fractures and/or carpometacarpal dislocations of all 5 rays with diaphyseal fractures of both forearm bones. This entity has never been described in the literature according to our finding. The carpometacarpal joint is a highly stable joint, which is ensured by the bony architecture and the capsuloligamentous system. The system consists of dorsal and palmar carpometacarpal ligaments, transverse intermetacarpal ligament that provides static stability, and the extensor and flexor tendons of the wrist and the interosseous muscles that contribute to dynamic stability [3]. Dorsal ligaments are usually stronger than their palmar counterparts [3,4], but dorsal dislocations are more frequent than palmar dislocations because trauma tends to force the metacarpal bone into flexion [5]. There are two main mechanisms of carpometacarpal dislocation, which include direct and indirect mechanisms. The direct mechanism occurs when force is applied directly to the base of the metacarpals, resulting in dorsal or palmar dislocation depending on the vector direction. The indirect mechanism occurs when force is applied anteriorly to the metacarpal heads, resulting in dislocation at the base. Less commonly, a blow to the ulnar border of the hand can cause a dorsal displacement of the metacarpal bases. High-speed injury is the most common mechanism for carpometacarpal dislocation [6]. In our descripted case, the displacement was posterior and radial due to the direct palmar impact of the car steering wheel against the hand in a motor vehicle accident. The diagnosis of this condition “floating wrist” can be difficult due to its occurrence often associated with polytrauma and severe injuries that have a more critical impact on the patient’s survival. In addition, the presence of wrist edema makes the bony structures non-palpable, making visualization on hand-wrist radiography more challenging. In more than half of cases, injuries to this area can go unnoticed during the initial medical visit [5]. A study by Henderson et al. found that the diagnosis was missed in 15 out of 21 patients [7]. These diagnostic difficulties highlight the importance of a thorough evaluation in cases of polytrauma and keeping in mind the possibility of wrist injury. Specific attention should be paid to wrist radiography, looking for signs of fractures and dislocations of the metacarpal bones. Wrist profile incidence allows diagnosis. Such as CT may be necessary to confirm the diagnosis in uncertain cases. It is essential to improve awareness and knowledge of this condition to avoid diagnostic errors and ensure proper management of patients with a “floating wrist.” Treatment options for a dislocated carpometacarpal joint fracture include closed reduction immobilization, closed reduction with internal fixation, or open reduction with internal fixation using Kirschner wires [8]. When using Kirschner wires, it is optimal to place them on the radial and ulnar borders of the metacarpals, angling them approximately 20° proximally in the coronal plane and 20° dorsally in the sagittal plane to avoid damaging neurological and tendinous structures. This allows for early mobilization and a quicker return to the full range of motion in flexion and extension [9]. Stability of the thumb carpometacarpal joint after reduction is a crucial factor in deciding whether non-operative or operative management is necessary. If the joint remains stable after reduction, immobilization in a thumb-spica cast for 4 to 6 weeks may be sufficient [10]. Pansard et al. first performed open reduction and internal fixation of the radial fracture, followed by a second step of reduction of the carpometacarpal dislocation and internal fixation using Kirschner wires [11]. In a complex case like ours, where there is a comminuted fracture of the second metacarpal neck and a radial artery section, the approach may involve performing open reduction and internal fixation of the radial fracture first, followed by reduction of the carpometacarpal dislocation and internal fixation with Kirschner wires. Longitudinal incisions on the ulnar border of the second metacarpal bone and the radial border of the fifth metacarpal are preferred, as this provides access to the necessary areas for repair and allows for osteosynthesis of the second metacarpal using a centromedullary Kirschner wire. The reduction of the first ray can be done through closed reduction. If the reduction remains stable, the hand can be immobilized with plaster cast using a brachial antebrachial palmar and immobilizing the thumb with free interphalangeal joint for 4 weeks, with elbow mobilization allowed at 3 weeks. The patient should be advised to elevate their hand and apply ice as soon as possible. Finger movements should be encouraged once the pain allows to reduce swelling and promote long-term joint recovery and to avoid most importantly post-operative stiffness. The removal of Kirschner wires should take place 6 weeks after the surgery. Then, an intense rehabilitation in a specialized rehabilitation center is required 9. As the range of motion improves, the patient must progressively hold objects starting from lightweight ones to progressively increase the grip strength. We started rehabilitation early at 4 weeks after plaster removal, with three sessions per week for 4 weeks, followed by two sessions per week for 3 weeks, in a specialized center with protection by a splint between sessions until the removal of the Kirschner wires, which was done 2 weeks after the start of rehabilitation. Complications are related to the severity of the initial trauma or the delay in treatment due to delayed consultation or initial diagnostic failure. Concomitant injuries, such as ulnar nerve damage and ischemia of the interosseous muscles due to edema and hematoma, can also contribute to poor outcomes. Inadequate fixation can result in loss of reduction and the need for further surgical intervention. Therapeutic failure can lead to post-traumatic arthritis. Delaying the initiation of movements can lead to joint stiffness. To avoid such complications, once the diagnosis of a radial fracture or carpometacarpal dislocation is made, it is important to proceed with early reduction, adequate stabilization, and rehabilitation as soon as possible.
This case report presents the first reported case of occurrence of a “floating wrist” in a 27-year-old male following a motor vehicle accident. This rare injury resulted in fractures of both forearm bones, along with dislocation and/or fracture of all five rays in the hand. The diagnostic challenges associated with this complex injury were highlighted, particularly in the context of polytrauma and wrist edema. Surgical intervention involved repairing the fractures and stabilizing the wrist using various techniques. Despite post-operative complications, including respiratory distress and an aortic aneurysm, successful management was achieved. The patient demonstrated satisfactory functional outcomes and regained complete wrist mobility after a 12-month follow-up period. This case emphasizes the importance of early diagnosis, appropriate surgical intervention, and prompt rehabilitation in the comprehensive management of complex wrist injuries. Further research and reporting of such rare cases are essential to enhance our understanding and improve patient outcomes in similar traumatic scenarios.
In managing complex wrist injuries like the “floating wrist,” it is crucial to maintain a high index of suspicion for such injuries in polytrauma cases. Early recognition and accurate diagnosis through thorough clinical and radiological evaluation are essential, especially given the difficulty in detecting these injuries amidst severe trauma and edema. Timely and precise surgical intervention to repair fractures and stabilize dislocations, coupled with early and intensive rehabilitation, are key to ensuring satisfactory functional recovery, minimizing complications, and enhancing overall patient outcomes. The importance of this article also lies in the fact that it describes a rare entity not documented in the medical literature. This case contributes to enriching knowledge on the management of complex wrist injuries and calls for further research and documentation to improve patient care and outcomes in similar scenarios.
References
- 1.Baudens A. Des fractures des os de l’avant-bras. Gaz Hôp 1847;1:117-9. [Google Scholar]
- 2.Sappey M. Le Traité D’anatomie Descriptive. Paris: V. Masson; 1878. [Google Scholar]
- 3.Gangloff D, Mansat P, Gaston A, Apredoaei C, Rongières M. Carpometacarpal dislocation of the fifth finger: Descriptive study of 31 cases. Chir Main 2007;26:206-13. [Google Scholar]
- 4.Yoshida R, Shah MA, Patterson RM, Buford WL Jr., Knighten J, Viegas SF. Anatomy and pathomechanics of ring and small finger carpometacarpal joint injuries. J Hand Surg Am 2003;28:1035-43. [Google Scholar]
- 5.Novak EM, Giostri GS. Reconhecimento precoce e tratamento das fraturas e luxações carpometacarpais. Rev Bras Ortop 2021;56:537-42. [Google Scholar]
- 6.Gülabi D, Uysal MA, Çevik B, Kılıç B, Karadeniz E. Carpometacarpal fracture dislocation of the fourth and fifth finger: Mid-term results of 15 patients. Eklem Hastalik Cerrahisi 2017;28:164-70. [Google Scholar]
- 7.Henderson J, Arafa MA. Carpometacarpal dislocation. An easily missed diagnosis. J Bone Joint Surg Br 1987;69:212-4. [Google Scholar]
- 8.Pundkare GT, Patil AM. Carpometacarpal joint fracture dislocation of second to fifth finger. Clin Orthop Surg 2015;7:430-5. [Google Scholar]
- 9.Bhardwaj P, Sivakumar BS, Vallurupalli A, Pai M, Sabapathy SR. Fracture dislocations of the carpometacarpal joints of the fingers. J Clin Orthop Trauma 2020;11:562-9. [Google Scholar]
- 10.Kim JS, Hussain K, Higginbotham DO, Tsai AG. Management of thumb carpometacarpal joint dislocations: A systematic review. J Orthop 2021;25:59-63. [Google Scholar]
- 11.Pansard E, Kaba A, Peyroux LM, Dereudre G, Koussougbo F, Mathevon H. Luxations spatulaires et lésions associées de la main et des deux os de l’avant-bras. À propos de deux cas. Chir Main 2009;28:250-4. [Google Scholar]








