
This case report describes a 45-year-old male with Ehlers–Danlos syndrome who sustained bilateral patellar tendon ruptures and obtained a good functional post-operative outcome following operative management through primary patellar tendon repair.
David Fraser, Department of Orthopaedic Surgery, The Prince Charles Hospital, Brisbane, Queensland, Australia. E-mail: David.Fraser@health.qld.gov.au
Abstract
Introduction: Bilateral spontaneous patellar tendon ruptures are rare, though it is hypothesized to be more common in patients with risk factors such as connective tissue disorders such as Ehlers–Danlos syndrome (EDS), systemic disorders weakening collagen structures, chronic stress around the patellar tendon, medications, and obesity or sedentary lifestyles. Clinicians should maintain a high degree of clinical suspicion for concerning features on clinical examination and radiological investigations to facilitate prompt diagnosis and operative management. This case report describes the first documented case of an adult patient with EDS who sustained bilateral spontaneous patellar tendon ruptures. There is one previously reported acute bilateral patellar tendon rupture occurring in a pediatric patient with EDS. Within the adult literature, two case reports have reported patients with EDS: One acute unilateral patellar tendon rupture who underwent operative management and one chronic patellar tendon tear requiring reconstruction 2.5 years following initial end-to-end repair.
Case Report: A 45-year-old male sustained bilateral patellar tendon ruptures after falling onto his knees while pushing a heavy cart. The patient reported a giving-way sensation and was unable to mobilize independently. On presentation to the emergency department, the patient was noted to have an absent straight-leg raise and a palpable gap between the distal pole of the patella and patellar tendon. Plain radiograph and ultrasound investigations confirmed bilateral complete patellar tendon ruptures. The patient underwent operative management 5 days following injury through bilateral direct patellar tendon repair utilizing the Krackow technique with transosseous fixation. Twelve months post-operatively, the patient had returned to pre-injuries activities of daily living, a full active range of motion without extensor lag, and recorded “fair knee function” on the Lysholm Knee Scoring Scale.
Conclusion: This case report described the first reported bilateral spontaneous patellar tendon rupture in an adult patient with EDS, who underwent operative management and achieved a return to pre-injury function. Furthermore, this case report summarizes the pre-existing literature on spontaneous bilateral patellar tendon ruptures and patellar tendon ruptures in patients with EDS.
Keywords: Spontaneous patellar tendon rupture, bilateral patellar tendon rupture, Ehlers–Danlos syndrome tendon rupture.
Patellar tendon ruptures are the third most common cause of disruption to the knee extensor mechanism [1]. Ruptures may occur through trauma or spontaneously, defined as activities that should not disrupt the musculotendinous unit [2]. Two theories exist on the pathogenesis of spontaneous ruptures: first, a microtrauma mechanical theory with traumatic bleeding into the synovial sheath with an intact fibrous sheath leading to increased intrasynovial pressure and hypoxia [3] and second, a vascular theory based on age-related changes and sedentary lifestyle [4,5]. Patellar tendon ruptures are typically unilateral and traumatic, occurring in younger patients [6]. Bilateral ruptures may be associated with systemic disorders that weaken collagen structures, such as renal failure [7], systemic lupus erythematosus [8], rheumatoid arthritis [9], hyperparathyroidism [10], and diabetes mellitus, connective tissue disorders, and medications including corticosteroids and anabolic hormones [11,12]. Patients may present with weak or absent active knee extension, difficulty weight-bearing, generalized knee pain, significant effusion, palpable infrapatellar soft tissue defect, or high-riding patella [13]. Radiological investigations confirm the diagnosis including ultrasound and plain radiograph demonstrating a patella alta, indicated by the Insall-Salvati ratio more than 1.2 as calculated by the position of the patella relative to the tibial tuberosity [13]. Non-operative management may be considered in cases of partial rupture or low-mobility patients with medical co-morbidities [14]. Surgical management options include primary repair and reconstruction. The location determines the type of primary repair: Ruptures at the origin (type 1) may have transosseous repair, mid-substance tears may have end-to-end repair (type 2), and distal avulsion tears (type 3) may require anchor repair [15]. Reconstruction with autograft or allograft may be required in severe or subacute cases [16]. Ehlers–Danlos syndrome (EDS), a genetic connective tissue disorder leading to altered fibrillar collagen metabolism [17], is diagnosed through examination, family history, and genetic testing. There are six subtypes: Classical, hypermobility, vascular, kyphoscoliosis, arthrochalasia, and dermatosparaxis [18]. EDS is characterized by generalized joint hypermobility, atrophic scarring, excessive bruising, delayed wound healing, and increased skin elasticity [19]. Knee instability is the most commonly involved joint, possibly contributed to by quadriceps and hamstring weakness [20]. Collagen fibers constitute 70–80% of the patellar tendon dry weight [2], with EDS patellar tendons demonstrating lower biomechanical properties compared to controls [21]. Healthy patellar tendons which require a force of 17.5 times the patient’s body weight to rupture [22], though EDS patients may require less force. There have been three cases of spontaneous patellar tendon rupture in patients with EDS reported in the literature. First, Moretti et al. reported a 13-year-old child with EDS who sustained bilateral spontaneous patellar tendon ruptures after a fall while walking and underwent primary tendon repair 72 h following the injury [23]. Takata et al. reported a 27-year-old male with classic EDS who sustained a unilateral spontaneous patellar tendon rupture while walking downstairs and underwent primary repair with semitendinosus and gracilis augmentation 5 days following the injury [24]. Finally, Iacono et al. reported a 23-year-old man with vascular EDS who sustained a chronic patellar tendon tear 2.5 years following primary tendon repair [25]. The reported case describes an adult patient with classical EDS who sustained bilateral spontaneous patellar tendon ruptures while pushing a heavy trolley. The patient underwent direct tendon repair and obtained good post-operative recovery at 12-month follow-up.
A 45-year-old male presented to the Emergency Department after falling while pushing a heavy trolley. The reported mechanism involved the trolley beginning to fall, with the patient attempting to balance the trolley, leading to eccentric contraction of quadriceps muscles. Immediately following the injury, the patient was unable to mobilize. He was diagnosed with classical EDS on genetic testing as a child, presenting with skin hyperextensibility, joint hypermobility, and hypertrophic scars on bony protrusions. He did not have any other medical conditions or take regular medications. He worked as a retail assistant at a variety of department stores and was independent with activities of daily living.

Clinical presentation
On examination of the right and left knee, there were palpable effusions, inability to actively straight leg raise, high riding patellae, and a palpable gap distal to the inferior pole of the patellae. Neurovascular examination was unremarkable. There was a high clinical suspicion of bilateral patellar tendon ruptures given the palpable gaps, though differential diagnoses included patella fractures.
Radiological features
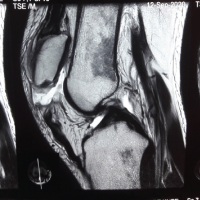
Plain radiographs (Fig. 1) of the knees demonstrated bilateral effusions, patella alta, and no fractures. Diagnosis of proximal patellar tendon tears was confirmed on ultrasound: The right knee ultrasound was reported to have a hematoma within the right patellar tendon, with a near complete loss of normal tendon fibers proximally and the left knee ultrasound was reported to show a complete tear involving the proximal aspect of the patellar tendon.

Management and post-operative recovery
The patient received temporary immobilization with bilateral knee splints in extension and underwent bilateral patellar tendon repairs 5 days following the injury. The patient underwent a general anesthetic and was positioned supine on a standard operating room table with a thigh tourniquet inflated to 300 mmHg. A midline incision was made with an anterior approach to the patella and patellar tendon. Intra-operatively, it was noted that the majority of the right patellar tendon was ruptured at the inferior pole of the patella and remained intact distally, while the left patellar tendon was completely avulsed from the inferior pole of the patella. Both sides were repaired with a braided polyblend suture, size 5 Fibrewire (Arthrex, Florida, USA) utilizing the Krackow technique and reinforced with transosseous fixation. The repair was ranged under direct visualization to ensure no gapping with flexion to 90°. The paratenon and retinaculum were repaired with a dissolvable suture, Vicryl (Ethicon, New Jersey, USA), and the skin was closed with non-absorbable nylon sutures (Ethicon, New Jersey, USA). The patient was immobilized in a DonJoy X-ROM post-operative knee brace (DJO Global, California, USA) locked in full extension for 1 week to protect the patient’s skin. The patient was able to weight bear as tolerated and began supervised rehabilitation with physiotherapists on a graded range of motion program: 0–30° flexion from 1 to 3 weeks post-operatively, 0–60° flexion from 3 to 5 weeks, and 0–90° from 5 to 7 weeks. On review 7 weeks post-operatively, the patient was able to straight leg raise without extensor lag and actively flex both knees to 105°, though was noted to have decreased quadriceps strength. He remained in the brace with unrestricted range and began quadriceps strengthening exercises. At 3 months post-operatively, his wounds were completely healed (Fig. 2), and he could achieve 135° flexion bilaterally. Following the wound healing, he commenced hydrotherapy and continued quadriceps strengthening exercises. At 6 months post-operatively, the patient could walk 100 m without crutches and 30 min with crutches, limited by quadriceps fatigue. On examination of his gait, he was noted to have a slight back knee gait due to quadriceps weakness on the right leg, though a normal left leg gait. Both knees had no palpable defect in the patellar tendon and achieved 140° flexion (Fig. 3a and b). He underwent an ultrasound which demonstrated both patellar tendons were intact. At 12 months, the patient achieved a full active range of motion without extensor lag. He had returned to pre-injury activities of daily living. He scored “fair” knee function on the Lysholm Knee Scoring Scale (score: 74 right; 69 left) [26] and 66.7% (right) and 67.8% (left) on the International knee documentation committee knee Score, with a higher score indicating better overall knee function [27].
This reports the first adult EDS patient who sustained bilateral patellar tendon ruptures and describes the operative management through direct repair. Furthermore, the case expands on the paucity of literature surrounding operative management for EDS patients with patellar tendon ruptures and post-operative outcomes. A literature review of unilateral or bilateral patellar tendon ruptures in pediatric or adult patients with EDS using PubMed, MEDLINE, and Scopus was conducted. The search was limited to full text and English language, which yielded three suitable case reports as summarized in Table 1. All three patients were male, with an average age of 21 years (range, 13–27 years). Two cases were acute patellar tendon ruptures, after a fall while walking (bilateral) and a fall down stairs (unilateral). One case was a unilateral chronic patellar tendon tear diagnosed 2.5 years following initial bilateral patellar tendon ruptures managed with primary end-to-end repairs. All patients underwent surgical management, with the two acute cases undergoing primary repair ± augmentation with autograft and the chronic tear undergoing reconstruction with allograft. The patient in the presented case report was 45 years old at the time of injury, which is higher than the previously reported cases in EDS patients (average: 21 years). However, the patient’s age is similar to the average age of 37.1 years reported by Fernandes et al. in a systematic review of simultaneous bilateral patellar tendon ruptures [28]. Previous literature has hypothesized age-related histological changes that may predispose patellar tendon ruptures, such as decreased elasticity, altered osteotendinous junction blood supply, and collagen degeneration [23]. While the low-energy mechanism of injury reported by the patient was similar to past case reports, age-related changes in conjunction with predisposition secondary to EDS may contribute to bilateral patellar tendons rupturing during eccentric contraction. Acute patellar tendon ruptures often undergo surgical management. Fernandes et al. reviewed 45 cases of spontaneous bilateral patellar tendon ruptures managed surgically, with 88.9% (40/45) patients receiving direct primary repair and 11.1% (5/45) patients undergoing reconstruction [28]. However, there is no consensus in the literature on surgical techniques in patients with connective tissue abnormalities [20], with differences in management noted between the previously reported case studies of EDS patients with acute patellar tendon ruptures. Moretti et al., described primary repair in a pediatric EDS patient 72 h following injury with primary repair utilizing a Vicryl suture (Johnson and Johnson, Bruxelles, Belgium) through a modified Bunnell technique and reinforced with wire cerclage, followed by post-operative immobilization with a brace locked at full extension [23]. Takata et al., described primary repair in an adult patient 5 days following unilateral patellar tendon rupture using FiberWire (Arthrex, Munich, Germany) transosseous sutures through a Krackow’s technique and augmented with semitendinosus and gracilis muscle, followed by post-operative immobilization in a long-leg cylinder cast [24]. At 12 months, the patient was able to walk without crutches and obtained an active range of motion to 145° flexion without extension lag. In comparison, the reported case describes an acute primary patellar tendon repair with utilizing the Krackow technique, reinforced with transosseous tunnels without autograft or allograft augmentation, and post-operative immobilization with a brace locked at full extension. At 12 months, the patient achieved similar clinical outcomes as the two previous case reports. While there is no reported medium or long-term follow-up for bilateral patellar tendon repairs in the literature [28], it is interesting to note Iacono et al., reported an EDS patient diagnosed with a unilateral chronic patellar tendon tear 2.5 years following bilateral primary end-to-end repairs at another institution [25]. Further research is required to explore surgical repair and reconstruction techniques for patients with connective tissue disorders and subsequent post-operative outcomes.
This case reports the first bilateral spontaneous patellar tendon rupture in an adult patient with EDS, who underwent operative management through primary tendon repair and returned to pre-injury function. As there is insufficient evidence for comparison between operative techniques, it is recommended that management should be individualized based on patient factors, concomitant injuries, and pre-injury functional capacity.
Spontaneous patellar tendon ruptures may be rare; however, clinicians should maintain a high degree of clinical suspicion with clinical examination and radiological features, particularly in patients with pertinent risk factors, such as EDS. The case report describes a 45-year-old male who sustained bilateral patellar tendon ruptures following a fall, underwent operative management utilizing the Krackow technique with transosseous fixation and obtained good functional outcome at 12 months.
References
- 1.Enad JG. Patellar tendon ruptures. South Med J 1999;92:563-6. [Google Scholar | PubMed]
- 2.Savarese E, Bisicchia S, Amendola A. Bilateral spontaneous concurrent rupture of the patellar tendon in a healthy man: Case report and review of the literature. Musculoskelet Surg 2010;94:81-8. [Google Scholar | PubMed]
- 3.Knorzer E, Folkhard W, Geercken W, Koch MH, Hilbert B, Krahl H, et al. New aspects of the etiology of tendon rupture. An analysis of time-resolved dynamic-mechanical measurements using synchrotron radiation. Arch Orthop Trauma Surg (1978) 1986;105:113-20. [Google Scholar | PubMed]
- 4.Kannus P, Józsa L. Histopathological changes preceding spontaneous rupture of a tendon. A controlled study of 891 patients. J Bone Joint Surg Am 1991;72:1507-5. [Google Scholar | PubMed]
- 5.Engkvist O, Lundborg G. Rupture of the extensor pollicis longus tendon after fracture of the lower end of the radius--a clinical and microangiographic study. Hand 1979;11:76-86. [Google Scholar | PubMed]
- 6.Tarazi N, O’loughlin P, Amin A, Keogh P. A rare case of bilateral patellar tendon ruptures: A case report and literature review. Case Rep Orthop 2016;2016:6912968. [Google Scholar | PubMed]
- 7.Caldas MT, Barbara GH, Barbara MB. Simultaneous bilateral rupture of the patellar ligament in chronic renal patient. A case report. Rev Bras Ortop 2013;48:455-9. [Google Scholar | PubMed]
- 8.Lu M, Johar S, Veenema K, Goldblatt J. Patellar tendon rupture with underlying systemic lupus erythematosus: A case report. J Emerg Med 2012;43:e35-8. [Google Scholar | PubMed]
- 9.Peiro A, Ferrandis R, Garcia L, Alcazar E. Simultaneous and spontaneous bilateral rupture of the patellar tendon in rheumatoid arthritis. A case report. Acta Orthop Scand 1975;46:700-3. [Google Scholar | PubMed]
- 10.Chen CH, Niu CC, Yang WE, Chen WJ, Shih CH. Spontaneous bilateral patellar tendon rupture in primary hyperparathyroidism. Orthopedics 1999;22:1177-9. [Google Scholar | PubMed]
- 11.Clark SC, Jones MW, Choudhury RR, Smith E. Bilateral patellar tendon rupture secondary to repeated local steroid injections. J Accid Emerg Med 1995;12:300-1. [Google Scholar | PubMed]
- 12.Stinner DJ, Orr JD, Hsu JR. Fluoroquinolone-associated bilateral patellar tendon rupture: A case report and review of the literature. Mil Med 2010;175:457-9. [Google Scholar | PubMed]
- 13.Rose PS, Frassica FJ. Araumatic bilateral patellar tendon rupture, a case report and review of the literaturet. J Bone Joint Surg Am 2001;83:1382-86. [Google Scholar | PubMed]
- 14.Murphy SM, McAleese T, Elghobashy O, Walsh J. Bilateral patellar tendon rupture following low-energy trauma in a young patient without predisposing risk factors. Trauma Case Rep 2022;40:100643. [Google Scholar | PubMed]
- 15.Courtney PM, Edmiston TA, Pflederer CT, Levine BR, Gerlinger TL. Is there any role for direct repair of extensor mechanism disruption following total knee arthroplasty? J Arthroplasty 2018;33:S244-8. [Google Scholar | PubMed]
- 16.Camarda L, D’Arienzo A, Morello S, Guarneri M, Balistreri F, D’Arienzo M. Bilateral ruptures of the extensor mechanism of the knee: A systematic review. J Orthop 2017;14:445-53. [Google Scholar | PubMed]
- 17.Byers PH. Inherited disorders of collagen gene structure and expression. Am J Med Genet 1989;34:72-80. [Google Scholar | PubMed]
- 18.Beighton P, Paepe AD, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: Revised nosology, Villefranche, 1997. Ehlers-danlos national foundation (USA) and ehlers-danlos support group (UK). Am J Med Genet 1998;77:31-7. [Google Scholar | PubMed]
- 19.Jensen JK, Nygaard RH, Svensson RB, Hove HD, Magnusson SP, Kjær M, et al. Biomechanical properties of the patellar tendon in children with heritable connective tissue disorders. Eur J Appl Physiol 2018;118:1301-7. [Google Scholar | PubMed]
- 20.Homere A, Bolia IK, Juhan T, Weber AE, Hatch GF. Surgical management of shoulder and knee instability in patients with ehlers-danlos syndrome: Joint Hypermobility syndrome. Clin Orthop Surg 2020;12:279-85. [Google Scholar | PubMed]
- 21.Nielsen RH, Couppe C, Jensen JK, Olsen MR, Heinemeier KM, Malfait F, et al. Low tendon stiffness and abnormal ultrastructure distinguish classic Ehlers-Danlos syndrome from benign joint hypermobility syndrome in patients. FASEB J 2014;28:4668-76. [Google Scholar | PubMed]
- 22.Zernicke RF, Garhammer J, Jobe FW. Human patellar-tendon rupture. J Bone Joint Surg Am 1977;59:179-83. [Google Scholar | PubMed]
- 23.Moretti B, Notarnicola A, Moretti L, Garofalo R, Patella V. Spontaneous bilateral patellar tendon rupture: A case report and review of the literature. Chir Organi Mov 2008;91:51-5. [Google Scholar | PubMed]
- 24.Takata Y, Nakase J, Numata H, Oshima T, Tsuchiya H. Repair and augmentation of a spontaneous patellar tendon rupture in a patient with Ehlers-Danlos syndrome: A case report. Arch Orthop Trauma Surg 2015;135:639-44. [Google Scholar | PubMed]
- 25.Iacono V, Cigala F, Fazioli F, Rosa D, Maffulli N. Reconstruction of chronic patellar tendon tear with allograft in a patient with Ehlers-Danlos syndrome. Knee Surg Sports Traumatol Arthrosc 2010;18:1116-8. [Google Scholar | PubMed]
- 26.Lysholm J, Gillquist J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med 1982;10:150-4. [Google Scholar | PubMed]
- 27.Irrgang JJ, Anderson AF, Boland AL, Harner CD, Kurosaka M, Neyret P, et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med 2001;29:600-13. [Google Scholar | PubMed]
- 28.Fernandes A, Rufino M, Hamal D, Mousa A, Fossett E, Cheema KS. Simultaneous bilateral patellar tendon rupture: A systematic review. Cureus 2023;15:e41512. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Bilateral Patellar Tendon Avulsion in End-Stage Renal Disease with G6 PD Deficient Patient: Case Report and Review of Literature
March 1, 2025 Bilateral Patellar Tendon Avulsion in End-Stage Renal Disease with G6 PD Deficient Patient: Case Report and Review of Literature February 5, 2012 Metastatic adenocarcinoma of proximal femur treated by custom made hip prosthesis. Case 1 – Jan -Mar 2012. Journal of Orthopaedic Case Reports
February 5, 2012 Metastatic adenocarcinoma of proximal femur treated by custom made hip prosthesis. Case 1 – Jan -Mar 2012. Journal of Orthopaedic Case Reports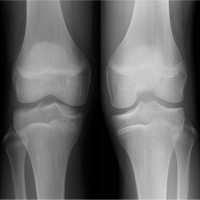 March 10, 2023 Bilateral Medial and Lateral Discoid Menisci: A Case Report
March 10, 2023 Bilateral Medial and Lateral Discoid Menisci: A Case Report July 10, 2023 A Type IV Tibial Tuberosity Avulsion Fracture in an Adolescent – A Case Report
July 10, 2023 A Type IV Tibial Tuberosity Avulsion Fracture in an Adolescent – A Case Report