
Medial clavicle physeal injuries are rare and may present as a dislocation of the sternoclavicular joint which may lead to a diagnostic dilemma for the orthopedic surgeon.
Dr. Dhruva Angachekar, Department of Orthopedics, Dr. N.Y. Tasgaonkar Medical College, Karjat, Maharashtra, India. E-mail: drdhruva55@gmail.com
Abstract
Introduction: Sternoclavicular injuries are rare and account for 1% of all dislocations. Medial clavicular physeal separation is another rare entity and may sometimes mimic a sternoclavicular dislocation. Diagnosis is usually missed in young adults due to a lack of clinical suspicion.
Case Report: A 22-year-old male patient sustained a right shoulder girdle injury due to a motorcycle accident. He was clinically diagnosed with a posterior sternoclavicular dislocation. On further imaging, a medial clavicular physeal injury was suspected. An attempt of closed reduction was attempted but not successful so it was converted to an open reduction. Physeal injury was confirmed and reduction was fixed with transosseous sutures using low-cost polyglactin suture material. The patient had a good clinical recovery.
Conclusion: Medial clavicle physeal injury may mimic sternoclavicular dislocations and should be clinically suspected in young adult patients.
Keywords: Posterior clavicle dislocation×physeal injury, transosseous fixation, medial clavicle epiphysis ossification.
Roughly 1% of all dislocations and 1–3% of all shoulder girdle injuries are caused by sternoclavicular joint injuries, which are uncommon clinical entities [1]. Another rare lesion is the medial physeal fracture separation of the clavicle which usually occurs in young adults and adolescents. There is a partial or complete separation between the clavicle and its epiphysis and mimics a sternoclavicular separation. Fifty percent of pediatric patients undergoing open reduction and internal fixation for posteriorly displaced sternoclavicular joint injuries had a fracture through the medial clavicle physis, according to research [2]. Medial clavicular physeal separation can occur till the fusion of the medial clavicular physis takes place which is usually between 22 and 25 years of age because of its late appearance and subsequently late fusion [3]. Epiphyseal injury is usually not suspected in young adults and so the diagnosis between a sternoclavicular dislocation and a medial clavicle physeal injury becomes a clinical dilemma. We present a case of a 22-year-old male who sustained a bike accident and presented to us with right-side sternoclavicular pain. He was suspected of having a posterior dislocation of the medial clavicle. Computed tomography (CT) images raised suspicions of a physeal injury which was confirmed intraoperatively.
A 22-year-old male patient presented in our outpatient department with pain in the right sternoclavicular region which aggravated on overhead activities. He sustained a fall on the right outstretched hand during a bike accident 8 h before presenting to us. On clinical examination, there was tenderness over the medial sternoclavicular joint as well as posterior dip in the medial clavicle (Fig. 1). This led us to clinically suspect a posterior sternoclavicular dislocation. The radiographs appeared normal (Fig. 2) so we advised a 3D reconstruction CT imaging of the right clavicle and sternum. CT images were suggestive of a posterior dislocation of the medial end of the clavicle (Fig. 3). However, one section of the CT appeared to show a flake of bone attached to the sternum. Medial clavicular physeal injury was a secondary diagnosis which was kept in consideration. We decided to take the patient up for closed reduction under anesthesia and covert to open reduction if closed attempts failed.
Once the patient was sedated, we tried a closed reduction of the medial end of the clavicle; however, it failed. Hence, we decided to go ahead with an open reduction of the medial end of the clavicle over the sternum. An incision was taken over the medial aspect of the clavicle and the sternoclavicular joint (Fig. 4).
 Once we reached the sternoclavicular joint capsule, we realized that the medial clavicular physis was still attached to the capsule (Fig. 5) and that there had been a physeal separation injury and the clavicle went posteriorly and got locked thus mimicking a posterior sternoclavicular dislocation. The reduction was done by giving lateral traction to the distal fragment using a towel clip (Fig. 6).
Once we reached the sternoclavicular joint capsule, we realized that the medial clavicular physis was still attached to the capsule (Fig. 5) and that there had been a physeal separation injury and the clavicle went posteriorly and got locked thus mimicking a posterior sternoclavicular dislocation. The reduction was done by giving lateral traction to the distal fragment using a towel clip (Fig. 6).
Once reduction was confirmed, we proceeded with fixing both fragments using polyglactin No 1 braided absorbable suture material. Two transosseous sutures were taken through the distal clavicle and the medial clavicular epiphysis, once each at the inferior and the superior end (Fig. 7). 
The fixation was stable and the distal fragment was no longer dislocating posteriorly (Fig. 8). The sternoclavicular joint capsule was repaired (Fig. 9) and after thoroughly giving a normal saline wound wash, the incision was closed in layers. The patient was put in an arm sling for 4 weeks and was advised strict immobilization on the shoulder girdle. At 4 weeks, passive range of motion exercises was initiated along with shoulder girdle stabilization exercises and at 6 weeks, active range of motion exercises. The patient regained full active range of motion by 12 weeks and was then started on girdle strengthening exercises. At 6-month post-surgery, the patient had regained pre-injury levels of strength.
Falling or engaging in sports-related activities can result in a direct hit to the shoulder, which is the most common cause of sternoclavicular joint injuries. They are common in the 4th decade and have a slight male predilection [1]. Epidemiological studies have shown that medial clavicular injuries are the least frequent (2% of all clavicular injuries) while road traffic accidents remain the most common cause of these injury patterns [4]. Medial clavicular physis takes place which is usually between 22 and 25 years of age because of its late appearance and subsequently late fusion [3]. As the sternoclavicular joint and the medial clavicular physis are close to each other, it becomes difficult to clinically distinguish a true posterior sternoclavicular dislocation from a medial clavicular physeal injury in such cases [5]. A high index of clinical suspicion should be kept after a high-energy traumatic injury to the shoulder girdle in adolescents and young adults [6]. Since our patient was a young adult with a shoulder girdle high-impact injury, we had a high level of suspicion for this injury presentation intraoperatively. Standard radiographs usually appear normal and may be misleading. Therefore, it is imperative that we perform a CT scan on such patients [7]. To determine the precise location of the fragment and plan reduction as well as osteosynthesis, a CT scan can be used to evaluate the relationship between the clavicular shaft and physis and the major vessels that are just posterior to it [8]. In our case, the radiographs essentially appeared normal. It was only on CT images that we could identify a posteriorly displaced clavicular shaft with a small medial epiphyseal bone. El Mekkaoui et al. in their case report described a similar injury in a 16-year-old boy due to a motorcycle accident. They also suspected a posterior sternoclavicular dislocation which eventually turned out to be a medial clavicle physeal injury. They were treated with opened reduction and fixation with a Kirschner wire (K wire). The K wire was removed at 6 weeks and a similar rehab protocol as ours was followed. The patient had excellent clinical recovery [6]. Beckmann and Crawford in their report of an adolescent female basketball player described a similar injury. They were unable to diagnose the case on radiographs as well as a CT scan. They additionally concluded that magnetic resonance imaging is a good imaging option if such injuries cannot be detected on radiographs and CT. Similar to our case, a closed reduction trial was given and it failed so the reduction was done under vision and fixed with a transosseous fiber wire sutures in a figure of eight pattern which was similar to our case [9]. In our case, we used a polyglactin suture instead of a fiber wire and still achieved a good functional outcome. The advantage of a polyglactin suture is that it is cost-effective as well as absorbable in nature, unlike fiber wires. It retains its strength for 4 weeks and is completely absorbed by 12 weeks which is enough for clinical recovery in such cases [10]. More sternoclavicular dislocations occur anteriorly than posteriorly, with posterior dislocations accounting for as much as 25–33% of all sternoclavicular dislocations [1]. Posterior dislocations have been reported to injure mediastinal tissues such as the trachea, brachial plexus, and major vessels. It has been found that 25–50% of patients with sternoclavicular joint posterior dislocations also present with clinical evidence of mediastinal compression [11]. The majority of posterior sternoclavicular injuries will require open reduction and fixation, despite certain studies recommending attempted close reduction for all of them as it may reduce up to 40–50% of these injuries [1,11,12]. It is possible for sternoclavicular injuries to manifest as a physeal fracture or as a capsular injury until the physis fuses. Physeal fracture dislocations of the sternoclavicular joint, as opposed to a pure posterior dislocation of the joint, were seen in 50% of the 40 skeletally immature patients with posterior sternoclavicular injuries who had open reduction and internal fixation, according to research by Lee et al. [2].
Medial clavicle physeal injury is a rarely documented injury pattern, especially in young adults. However, it should be kept in mind as a clinical diagnosis for young adults presenting with medial clavicular injuries as this physis fuses by 25 years of age. Most of these cases get misdiagnosed as sternoclavicular dislocations as clinical suspicion of a physeal injury is very limited among orthopedic surgeons in these age groups. Additional investigations such as a CT are essential in these cases and minimum attempts at closed reduction should be attempted due to the proximity of mediastinal structures. Transosseous fixation with low-cost absorbable sutures has good functional outcomes postoperatively.
Medial clavicular physeal may be misdiagnosed as a sternoclavicular dislocation in the adolescent or young adult age group due to low clinical suspicion. Open reduction and transosseous fixation give excellent results in such cases.





Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2023 Periosteal Osteosarcoma of the Distal Shaft of Fibula: Case Report on Rare Entity
June 10, 2023 Periosteal Osteosarcoma of the Distal Shaft of Fibula: Case Report on Rare Entity June 10, 2024 OrthoAI: A Surgical Copilot. There will be a Personalised Surgical Copilot for every Orthopaedic Surgeon!
June 10, 2024 OrthoAI: A Surgical Copilot. There will be a Personalised Surgical Copilot for every Orthopaedic Surgeon! April 1, 2026 Understanding Synovial Chondromatosis: A Rare Cause of Shoulder Impingement
April 1, 2026 Understanding Synovial Chondromatosis: A Rare Cause of Shoulder Impingement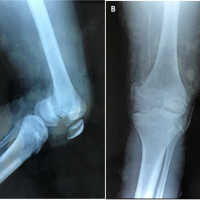 May 10, 2024 The Challenging Diagnosis and Management of a Pediatric Bicondylar Hoffa Fracture: A Case Report
May 10, 2024 The Challenging Diagnosis and Management of a Pediatric Bicondylar Hoffa Fracture: A Case Report