
How to manage a burnt leg stump to preserve the length necessary for prostesization.
Dr. Tito Brambullo, Department of Neurosciences, Clinic of Plastic Surgery, University of Padua, Padua, Italy. E-mail: tito.brambullo@unipd.it
Abstract
Introduction: Negative pressure wound therapy (NPWT) is a beneficial tool for enhancing the local conditions of complex wounds. Clinical evidence supports its application in the management of burn injuries; however, limited data are available concerning the effectiveness of NPWT on dermal substitutes and skin grafts.
Case Report: A 29-year-old female patient was referred to our clinic after sustaining severe burns in a road accident. The patient’s right lower limb was affected, necessitating an amputation below the knee. To preserve an adequate stump length, multiple procedures were performed, including the application of NPWT to optimize the uptake of the graft into the wound bed. The rehabilitation program for the amputated leg was aided by maintaining a suitable stump length, which can be challenging to achieve when burn damage is present.
Conclusion: The use of skin substitutes and grafts can benefit from the application of mild negative pressure, which can improve adherence to the wound bed. The clinical case presented highlights the benefits of NPWT in managing complex lower-limb trauma, thereby expanding the scope of this technique.
Keywords: Amputation stump, burns, negative pressure wound therapy, road injury, skin graft.
Negative pressure wound therapy (NPWT) is a specialized treatment method that involves the use of a sterile foam dressing and a suction device to create negative pressure on the wound site. This technique has been shown to have several benefits, including the promotion of granulation tissue development and re-epithelialization, as well as faster healing of burn wounds [1]. In fact, NPWT has become the standard of care for the treatment of acute and chronic wounds in many countries. The therapy works by inducing capillary growth and removing excess fluids from the wound site, which helps to reduce the risk of bacterial colonization and promote faster healing. While more research is needed to fully understand the cost-effectiveness of NPWT, there is evidence to support its use in the management of burn injuries [2]. One promising application of NPWT is in improving skin graft uptake, which is particularly important in patients with lower-limb trauma associated with burn damage. Although there are various methods for covering complex skin lesions, split-thickness skin grafts are the most common approach. While there is some literature available on how to secure grafts [3,4], there are lack of data on the impact of NPWT on the success of skin grafts [5]. We present our experience with using NPWT to enhance skin grafts in a patient who lost her right leg due to a road accident.
A 29-year-old female patient was admitted to our clinic for treatment in October 2023, following a severe road accident that left her with multiple injuries. She sustained several fractures, along with 3rd° burns that covered her entire right lower limb and right flank, which represented 20% of her total body surface area. Despite the surgical debridement and escharotomies, the right leg’s soft tissues became full-thickness necrotic, necessitating the decision to amputate the inferior limb (Fig. 1).
The stump was kept long enough to allow for the use of a prosthetic, but definitive coverage was not possible due to the burn extension. As a result, wounds were temporarily covered with dermal substitutes, such as Integra® and Pelnac™. Only the tip of the stump was repaired with a meshed skin graft (Fig. 2). Antibiotic therapy was deemed necessary based on the findings of the swab test; however, blood cultures and bacteriuria screening remained negative throughout the entire hospitalization period. The wounds were then covered with homologous skin grafts from a cadaver bank (Fig. 3) and NPWT was initiated by applying Suprasorb® R CNP EasyDress® by Lohmann and Rauscher on the grafts at −80 mmHg.
The NPWT dressing comprised of an absorbent sponge molded to fit the wound size, in direct contact with the skin grafts, and a plastic casing that was subsequently positioned and connected to a vacuuming system, resulting in negative pressure being applied throughout the lower limb (Fig. 4). In general, NPWT is kept in place for 3–4 weeks and the dressing is renewed weekly.

The system applies the chosen negative pressure continuously. After a week, the bank grafts were replaced by autologous skin grafts, harvested from the patient’s left thigh and meshed with 1:6 and 1:3 ratios (Fig. 5), then EasyDress® was applied with a negative pressure of −100 mmHg considering the higher serum drainage from the graft holes. After 12 days, the NPWT was stopped since the skin grafts showed successful taking and no significant drainage was evident (Fig. 6).
The NPWT was used for a total time of 19 days. A month after the traumatic event, the injured areas were almost fully repaired (Fig. 7). The patient was then transferred to a rehabilitation service to prepare for the prosthetization of the right leg. At the time of writing this article, the patient is actively engaging in the rehabilitation program, and the lower limb stump is free of complications.
The use of NPWT in an emergency setting for damage control of injured and fractured lower limbs is well known [6-8]. NPWT presents several advantages. First, it allows for wound exudate control, so the absorbent sponge can be left untouched for 5-7 days in contact with the wound bed. Despite the extensive area of injury, the patient did not develop an infection during the month we used NPWT, proving its efficacy in superinfection prevention. Second, unlike traditional dressings that need to be renewed every day, NPWT reduces patient discomfort by tailoring the negative pressure adjustment and also decreases the nursing staff workload [3]. Although tie-over dressing is the most used and successful method in securing skin grafts in most patients, when there is a need to cover complex surfaces (joint or circumferential areas) or subcutaneous tissue with abundant production of fluids, as in our case, skin grafts would hardly take well. The NPWT allows for the immobilization of grafts to the wound bed, even in difficult locations, which facilitates graft taking. The disadvantages of NPWT include the cost, lengthening the dressing procedure, and the need for additional surgery in the operating room with anesthesia to remove the dressing in the event of a large wound. Training the nursing staff is necessary to monitor and manage the functioning of NPWT [3]. The use of NPWT as a bolster dressing for autografts is supported by literature data. Scherer et al. [7] conducted a retrospective study in which they compared traditional skin graft securing methods with NPWT in skin lesions of various natures, 50% of which were burn wounds. The NPWT group had a lower rate of graft failure, according to a subgroup analysis of burn wounds (0% vs. 19%). A prospective randomized trial by Petkar et al. [8] compared skin grafts taken in 21 patients with burn lesions treated with NPWT applied on split-thickness skin grafts and 19 patients with burn wounds receiving a traditional compressive dressing on the same kind of grafts. The average graft take was higher in the NPWT group than in the control group (96.7% vs. 87.5%; P < 0.001). In a double-blind randomized trial, a comparison was made between the total area of skin graft loss for skin wounds, with over half of them being burns, in grafts secured using conventional methods and NPWT [9]. The authors reported a median failure of skin grafts of 0.0 cm2 for the NPWT group and of 4.5 cm2 for the control group (respectively, range 0.0–11.8 cm2 and range 0.0–5.2 cm2; P = 0.001) and the median percentage of graft loss in the negative pressure group was 0.0% (range, 0.0–62.0%) versus 12.8% (0–75.9%) in the control group (P < 0.001). Patients treated with NPWT also had significantly reduced length of hospital stays. Although burn patients are not the sole focus of most studies on the use of NPWT on grafts, the studies we examined demonstrate that NPWT improves graft healing. According to the literature, using NPWT as a dressing can help integrate bilaminate dermal substitutes. Jeschke et al. [10] compared the use of traditional compression dressing versus NPWT used together with fibrin glue to secure a bilaminate dermal substitute. A split-thickness skin graft was placed after the dermal substitute was fully vascularized and the take rate was measured as a percentage of the total area of dermal substitute placement. The rate of graft take was found to be significantly higher in cases where NPWT plus fibrin glue was used compared with patients treated with conventional dressings (98% vs. 78%; P < 0.003). In addition, patients treated with NPWT had a shorter time to definitive coverage (10 days vs. 24 days; P < 0.002). However, it is hard to tell the difference between the benefits of NPWT and the fibrin glue used in conjunction with it in this study. A retrospective study conducted by Molnar et al. [11] examined the integration of bilaminate dermal substitutes and the rate of skin graft take, both managed with NPWT coverage. The patients examined had lesions of different extents, with exposed bone, tendon, or joint that would otherwise require more complex reconstructive procedures. The dermal substitute revascularization rate was 96%, the skin graft take rate was 93%, and the average time between dermal substitute placement and skin grafting was 7.25 days, as revealed in the study. Both studies seem to agree that NPWT can enhance the rate of vascularization of bilaminate dermal substitutes, leading to a shorter delay before skin grafting and better overall skin graft outcomes.
According to our observations, NPWT has proven to be a useful and effective approach for managing complex cases of burns and amputated lower limbs. The primary advantages of NPWT include effective exudate management, protection against superinfections, and promotion of wound bed granulation, all of which contribute to improving the local conditions and facilitating early grafting. The literature also supports the specific application of NPWT on dermal substitutes and skin grafts on burn surfaces, thereby expanding the scope of this technology in the field.
The objective of preserving an optimal amputation stump length to aid prosthesis use can be realized even in the presence of extensive burn damage by utilizing reconstructive approaches and wound-healing methodologies.
References
- 1.Deva AK, Buckland GH, Fisher E, Liew SC, Merten S, McGlynn M, et al. Topical negative pressure in wound management. Med J Aust 2000;173:128-31. [Google Scholar | PubMed]
- 2.Elwood ET, Bolitho DG. Negative-pressure dressings in the treatment of hidradenitis suppurativa. Ann Plast Surg 2001;46:49-51. [Google Scholar | PubMed]
- 3.Kantak NA, Mistry R, Varon DE, Halvorson EG. Negative pressure wound therapy for burns. Clin Plast Surg 2017;44:671-7. [Google Scholar | PubMed]
- 4.Hansbrough W, Doré C, Hansbrough JF. Management of skin-grafted burn wounds with xeroform and layers of dry coarse-mesh gauze dressing results in excellent graft take and minimal nursing time. J Burn Care Rehabil 1995;16:531-4. [Google Scholar | PubMed]
- 5.Sposato G, Molea G, Di Caprio G, Scioli M, La Rusca I, Ziccardi P. Ambulant vacuum-assisted closure of skin-graft dressing in the lower limbs using a portable mini-VAC device. Br J Plast Surg 2001;54:235-7. [Google Scholar | PubMed]
- 6.Matsumine H, Giatsidis G, Fujimaki H, Yoshimoto N, Makino Y, Hosoi S, et al. NPWTi allows safe delayed free flap repair of Gustilo IIIb injuries: A prospective case series. Regen Ther 2021;18:82-7. [Google Scholar | PubMed]
- 7.Scherer LA, Shiver S, Chang M, Meredith JW, Owings JT. The vacuum assisted closure device: A method of securing skin grafts and improving graft survival. Arch Surg 2002;137:930-3; discussion 933-4. [Google Scholar | PubMed]
- 8.Petkar KS, Dhanraj P, Kingsly PM, Sreekar H, Lakshmanarao A, Lamba S, et al. A prospective randomized controlled trial comparing negative pressure dressing and conventional dressing methods on split-thickness skin grafts in burned patients. Burns 2011;37:925-9. [Google Scholar | PubMed]
- 9.Llanos S, Danilla S, Barraza C, Armijo E, Piñeros JL, Quintas M, et al. Effectiveness of negative pressure closure in the integration of split thickness skin grafts: A randomized, double-masked, controlled trial. Ann Surg 2006;244:700-5. [Google Scholar | PubMed]
- 10.Jeschke MG, Rose C, Angele P, Füchtmeier B, Nerlich MN, Bolder U. Development of new reconstructive techniques: Use of Integra in combination with fibrin glue and negative-pressure therapy for reconstruction of acute and chronic wounds. Plast Reconstr Surg 2004;113:525-30. [Google Scholar | PubMed]
- 11.Molnar JA, DeFranzo AJ, Hadaegh A, Morykwas MJ, Shen P, Argenta LC. Acceleration of integra incorporation in complex tissue defects with subatmospheric pressure. Plast Reconstr Surg 2004;113:1339-46. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Segmental Achilles Tendon Loss With Skin Defect in an Open Calcaneal Fracture Managed Without Tendon Reconstruction: A Case Report
May 1, 2026 Segmental Achilles Tendon Loss With Skin Defect in an Open Calcaneal Fracture Managed Without Tendon Reconstruction: A Case Report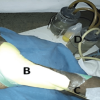 January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial
January 1, 2026 Comparison of Indigenous Low Cost Vacuum-Assisted Closure Therapy and Standard Wound Therapy in Open Fractures: A Randomized Controlled Trial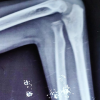 October 1, 2025 Neglected Monteggia Fracture-Dislocation in an 8-Year-Old Child with Posterior Interosseous Nerve Palsy: A Case Report
October 1, 2025 Neglected Monteggia Fracture-Dislocation in an 8-Year-Old Child with Posterior Interosseous Nerve Palsy: A Case Report June 10, 2024 Lambrinudi Triple Arthrodesis with Posterior Tibial Tendon Transfer in Adult Fixed Equinus Deformity: Case Report
June 10, 2024 Lambrinudi Triple Arthrodesis with Posterior Tibial Tendon Transfer in Adult Fixed Equinus Deformity: Case Report