
The impact of pes planus is a function of its severity, with severe pes planus causing early onset medial compartment OA in younger age group.
Dr. Meet Shah, Department of Orthopedics, Dr. D. Y. Patil Medical College Hospital and Research Institute, Pimpri-Chinchwad, Maharashtra, India. E-mail: mbbs_ms_meetshah@yahoo.com
Abstract
Introduction: Pes planus, commonly known as flat foot, is characterized by the lowering of the medial longitudinal arch of the foot, leading to alterations in lower limb biomechanics and potential pain and injury. This condition can affect the mechanical alignment and dynamic function of the lower limb, potentially contributing to the development and progression of knee osteoarthritis (OA). This study aims to investigate the association between pes planus and medial compartment knee OA as well as its impact on the knee functional score.
Materials and Methods: This cross-sectional study included 165 patients aged 20–72 years. Inclusion criteria were individuals with unilateral or bilateral flat feet, while exclusion criteria were other foot conditions, history of knee or ankle surgeries, rheumatoid arthritis, and limb length discrepancies. Clinical assessments included knee joint tenderness, foot arch measurement using the foot arch index, and radiographic evaluations of Meary’s angle and tibiofemoral (TF) angle. The knee injury and osteoarthritis outcome score (KOOS) was used to assess knee function.
Results: The study population had a mean age of 43.98 ± 13.17 years. Meary’s angle ranged from 5 to 19° (mean 9.46), and the foot arch index ranged from 0.220 to 0.520 (mean 0.33). The TF angle ranged from 1.7 to 7.5° (mean 4.98). KOOS scores varied from 10 to 100 (mean 62.40). Patients with more severe flat feet (higher Meary’s angle and foot arch index) had significantly lower KOOS scores, indicating worse knee function and greater pain. The correlations between foot arch index, Meary’s angle, and KOOS scores were statistically significant (P = 0.001).
Conclusion: This study demonstrates a strong association between flat foot severity and knee OA. Increased Meary’s angle and foot arch index were correlated with worsened knee function and increased pain, as measured by KOOS scores. These findings highlight the importance of assessing foot posture in patients with medial compartment OA and suggest that early intervention and orthotic management could be beneficial in mitigating the progression and severity of knee OA in patients with pes planus.
Keywords: Pes planus, Medial compartment Osteoarthritis, Foot arch index, Meary’s angle
Pes planus, commonly known as flat foot, is characterized by the lowering of the medial longitudinal arch of the foot, resulting in the flattening of the foot arch [1]. While often asymptomatic, this condition alters lower limb biomechanics and muscle activity, potentially leading to pain and injury [2,3]. There are two main types of pes planus: Flexible and rigid. Flexible pes planus shows a normal arch when the foot is not bearing weight but a lowered arch when it is weight-bearing [2]. In contrast, rigid pes planus, also known as structural pes planus, involves a permanently lowered arch. Flexible pes planus can be associated with posterior tibial tendon dysfunction, hindfoot fractures, plantar fascia injuries, spring ligament injuries, and degenerative or inflammatory arthropathies [2-4]. The human foot’s arches – medial longitudinal, lateral longitudinal, anterior transverse, and posterior transverse – are crucial in shaping the foot and are unique to each individual [5]. The foot plays a vital role in absorbing mechanical stresses from ground contact and influences postural alignment and joint motion in the knee and lower extremities [6]. During weight-bearing activities, the interrelationship between knee posture and foot motion can lead to excessive rotation in individuals with flat feet [7]. It has been reported that flat feet often result in knee pain and damage to the medial cartilage [8]. Knee osteoarthritis (OA) is a degenerative, age-related disorder characterized by chronic joint stiffness and pain, which limits daily activities. Although the exact etiology of knee OA is not fully understood [9,10], recent studies have focused on biomechanical factors in the disease’s pathogenesis, especially the knee adduction movement, which has been implicated in the progression of medial compartment knee OA. Globally, symptomatic knee OA affects an estimated 9.6% of men and 18.6% of women over the age of 60. In India, the prevalence ranges from 22% to 39% [11,12]. Foot posture has been suggested to influence the development of lower limb musculoskeletal conditions due to its impact on the mechanical alignment and dynamic function of the lower limb [13,14]. Recent studies have indicated that a more pronated foot posture is common in individuals with OA and is associated with pes planus morphology and medial cartilage damage [15-18]. The relationship between pes planus and knee OA highlights the need to consider the impact of flat feet on the progression and severity of knee OA.
The aim is to study the association between the flat foot and medial compartment OA.
Given the prevalence of OA at 39% in the Indian population, as reported by Pal et al. in “An Epidemiology of Knee OA in India and Related Factors,” a sample size of 163 was determined based on a 95% confidence interval, an acceptable difference of 7.5/100, and an assumed rate of 39%/100. The inclusion criteria for the study were individuals over 20 years of age with unilateral or bilateral flat feet. Exclusion criteria included the presence of any other foot conditions, a history of operative procedures on the knee or ankle joints, the presence of rheumatoid arthritis, and limb length discrepancies. Patients were clinically examined for knee joint tenderness and assessed for foot arch using the foot arch index. Radiographic assessments were conducted, including knee radiographs to determine the Kellgren–Lawrence (KL) grade of knee OA and weight-bearing lateral radiographs to measure Meary’s angle. In addition, the tibiofemoral (TF) angle was calculated to identify varus deviations in the patients. The patients were asked to fill up the knee injury and osteoarthritis outcome score (KOOS) questionnaire to assess their knee functions. After collecting the data, patients were divided into two broad age groups: Those younger than 45 years and those older than 45 years. Each of these groups was further subdivided into patients with knee pain and those without knee pain. The severity of flat foot and its association with knee pain and the development of radiological knee changes were then compared across these subgroups.
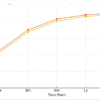
The study included 165 patients ranging from 20 years to a maximum of 72 years, and the mean age in this study was 43.98 ± 13.17 years as shown in Table 1. Age-wise distribution showed that 51.5% of the subjects were >45 years and 48.5% of the patients were under 45 years of age as shown in Table 2. The Meary’s angle measured in the subject ranged from a minimum of 5° to a maximum of 19° with the mean being 9.46°. The foot arch index ranged from 0.220 to 0.520 with a mean of 0.33 as shown in Table 3. The tibiofemoral angle measured in the subject ranged from a minimum of 1.7 to a maximum of 7.5° with the mean being 4.984°. The KOOS score in the patients were recorded between a minimum of 10 and a maximum of 100 and the mean was 62.40 as shown in Table 4. The patients were classified into two groups one with minimal knee pain with KL grade 1 and 2 and the other with severe knee pain and KL grade 3 and 4. 85 patients with minimal knee pain had a mean tibiofemoral angle of 6.20 ± 0.82 and 80 patients with severe knee pain had a mean tibiofemoral angle of 3.68 ± 0.99. The correlation between tibiofemoral angle and knee pain was statistically significant. (P = 0.001), suggesting that the patients with more varus deviated knee are likely to have more severe knee pain. This is shown in Table 5. Out of 83 patients (50.3%) having foot arch index <0.31, 74 (44.8%) had minimal knee pain and 9 (5.5%) had severe knee pain. Out of 82 patients (49.7%) having foot arch index >0.31, 11 (6.7%) had minimal knee pain and 71 (43%) had severe Knee pain. The correlation between foot arch index and KL grade was statistically significant (P = 0.001). Out of 80 patients (48.5%) having Meary’s angle (in degree) <8, 77 (46.7%) had minimal knee pain and 3 (1.8%) had severe knee pain. Out of 85 patients (51.5%) having Meary’s angle (in degree) >8, 8 (4.8%) had minimal knee pain and 77 (46.7%) had severe knee pain. The correlation between Meary’s angle and KL grade was statistically significant. (P = 0.001) this is depicted in Table 6. Fig. 1 shows the calculation of Meary’s angle, and Fig. 2 and 3 show the calculation of the tibiofemoral angle Eighty-three patients (50.3%) had a foot arch index <0.31, of which, 8 patients (4.8%) had a KOOS score <50 and 75 patients (45.5%) had a KOOS score >50. Eighty-two patients (49.7%) had a foot arch index >0.31, of which, 63 patients (38.2%) had a KOOS score <50 and 19 patients (11.5%) had a KOOS score >50. The correlation between the foot arch index and KOOS score was statistically significant (P = 0.001), as the severity of flat foot increases the severity of knee pain in the patients and the function of the knee decreases as shown by deteriorating KOOS score. 80 patients (48.5%) having Meary’s angle <8, of which, 3 patients (1.8%) had a KOOS score <50 and 77 patients (46.7%) had a KOOS score >50. 85 patients (51.5%) having Meary’s angle >8, of which, 68 patients (41.2%) had a KOOS score <50 and 17 patients (10.3%) had a KOOS score >50. The correlation between Meary’s angle and KOOS score was statistically significant. (P = 0.001) shown in Table 7, Graphs 1 and 2. The odds ratio and relative risk were calculated to compare patients with severe flat foot to those with mild to moderate flat foot in relation to the development of significant knee OA, as assessed by radiographic KL grades. Severe flat foot was defined by a foot arch index, while mild to moderate flat foot was classified as the non-exposed group. Out of 82 patients with severe flat foot, 71 had radiographic KL grades 3 or 4, indicating advanced OA. In contrast, among 83 patients with mild to moderate flat foot, only 9 had radiographic KL grades 3 or 4. The results showed an odds ratio of 53.07 and a relative risk of 8.6, indicating that patients with severe flat foot are significantly more likely to develop severe knee OA compared to those with mild to moderate flat foot.










There is a lack of research on the connection between pes planus and knee OA, despite data indicating a biomechanical association. The potential for mechanical stress on the TF and patellofemoral compartments due to an overly planus foot shape has been suggested. This study examines several parameters related to this association. Sharma et al. [11] investigated knee OA in individuals older than 60 years, identifying high body mass index, obesity, a history of knee injuries, female sex, age (50–75 years), and vigorous physical activity as risk factors for OA, as supported by Silverwood et al. [20]. These findings align with our study, where the mean age of patients was 43.98 ± 13.17 years. Among the 165 patients, 80 (48.5%) were younger than 45 years, and 85 (51.5%) were older than 45 years. The talar-first metatarsal angle, calcaneal pitch, and talonavicular coverage angle are crucial metrics for diagnosing and grading flat feet in adults. A larger rotation of up to 7° laterally indicates flat feet, with a Meary’s angle of 15° considered “severe” flat foot [19]. In our study, the mean Meary’s angle was 9.46±3.44°. Radiographs of individuals with clinically confirmed flatfoot and those with normal feet, as investigated by Younger et al. and Coughlin and Kaz, showed substantial correlations between flatfoot and abnormal Meary’s angle, calcaneal pitch angle, and cuneiform-to-fifth metatarsal height. Hakukawa et al. [21] found that severe flatfoot often accompanies the progression of knee OA, particularly as the condition advances from KL-1 to KL-2 and KL-3 stages. The medial longitudinal arch index, specifically the anteroposterior (AP) Meary’s angle, is an important indicator for assessing flatfoot. The AP Meary’s angle defines the arch height and is effective for evaluating planovalgus deformity, which reflects the alignment of the talocrural and subtalar joints. Our study found a statistically significant correlation between Meary’s angle and both KL grade and KOOS score (P = 0.001). An increase in Meary’s angle was associated with significant worsening of knee function, as demonstrated by the KOOS score. Patients with a Meary’s angle <8 degrees had good knee function and minimal knee pain. During activity, the foot absorbs stress and serves as a cushion. A healthy arch helps maintain balance, while flat feet reduce the cushioning effect, causing increased stress on the knees and altering the biomechanical line, making prolonged walking difficult. The arch index, which measures foot features using a static footprint, is a reliable tool that does not depend on the examiner’s clinical judgment. Levinger et al. [17] demonstrated that the arch index shows good reliability and can distinguish medial compartment knee OA based on changes in foot position. In our study, the mean foot arch index was 0.33 ± 0.06. The correlation between foot arch index and KOOS score was statistically significant (P = 0.001), with patients having a foot arch index score <0.31 showing better functional scores compared to those with scores above 0.31. Unusual foot alignment and structure can lead to compensatory mechanisms such as varus knee. In our study, the mean TF angle was 4.984 ± 1.55°. Patients with minimal knee pain had a mean TF angle of 6.20 ± 0.82°, while those with severe knee pain had a mean angle of 3.68 ± 0.99 degrees. The correlation between TF angle and knee pain was statistically significant (P = 0.001). These findings are consistent with Zhang et al. [22], who concluded that flat feet contribute to knee pain, and the severity of flattening determines the severity of knee pain. In our study, the mean KOOS score was 62.4 ± 29.21. Patients with minimal knee pain had a KOOS score of 88.04 ± 9.80, while those with severe knee pain had a mean KOOS score of 35.16 ± 14.55. The correlation between KOOS score and knee pain was statistically significant (P = 0.001). Comparisons of KOOS scores against foot arch index and Meary’s angle showed that patients with less severe flat feet had better knee function and minimal pain, whereas those with a foot arch index >0.31 and a Meary’s angle >8° had worsening knee scores. This trend was observed even in the younger age group, indicating that a more severe flat foot is associated with worse knee scores.
Limitations:
The association between flatfoot and knee OA was examined; however, other significant variables including foot discomfort were not taken into account. We did not rule out the potential that pain in other joints may play a role.
A small sample size
A longitudinal study is required to assess the causal relationship between severe flat foot and early-onset medial compartment OA in the younger age group. A study is required to study the effect of giving foot orthosis to young patients and flat foot progression.
The results of this study demonstrated a strong association between flatfoot and knee OA, and the foot posture is strongly correlated with the internal femorotibial knee OA, as a more pronated foot causes internal rotation at the tibia and worsening of the knee functions and knee pain. The assessment of the foot posture of people with medial compartment OA is necessary to improve our understanding of foot orthoses and footwear modification on lower limb alignment and function. Old age, increased Meary’s angle, foot arch index, reduced TF angle, and KOOS score were significant variables that showed a strong association in demonstrating the relation between pes planus and the development of knee OA in the present study.
Flat foot and is associated with knee OA. The more severe the flat foot the worse are the knee functional scores in the patients. Severe flat foot is also a risk factor for the development of early-onset knee OA in younger individuals.
References
- 1.Franco AH. Pes cavus and pes planus. Analyses and treatment. Phys Ther 1987;67:688-94. [Google Scholar | PubMed]
- 2.Raj MA, Tafti D, Kiel J. Pes planus. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. [Google Scholar | PubMed]
- 3.Murley GS, Menz HB, Landorf KB. Foot posture influences the electromyographic activity of selected lower limb muscles during gait. J Foot Ankle Res 2009;2:35. [Google Scholar | PubMed]
- 4.Erol K, Karahan AY, Kerimoğlu Ü, Ordahan B, Tekin L, Şahin M, et al. An important cause of pes planus: The posterior tibial tendon dysfunction. Clin Pract 2015;5:699. [Google Scholar | PubMed]
- 5.Abourazzak FE, Kadi N, Azzouzi H, Lazrak F, Najdi A, Nejjari C, et al. A positive association between foot posture index and medial compartment knee osteoarthritis in Moroccan people. Open Rheumatol J 2014;8:96-9. [Google Scholar | PubMed]
- 6.Guler H, Karazincir S, Turhanoglu AD, Sahin G, Balci A, Ozer C. Effect of coexisting foot deformity on disability in women with knee osteoarthritis. J Am Podiatr Med Assoc 2009;99:23-7. [Google Scholar | PubMed]
- 7.Souza TR, Pinto RZ, Trede RG, Kirkwood RN, Fonseca ST. Temporal couplings between rearfoot-shank complex and hip joint during walking. Clin Biomech (Bristol, Avon) 2010;25:745-8. [Google Scholar | PubMed]
- 8.Paterson KL, Kasza J, Hunter DJ, Hinman RS, Menz HB, Peat G, et al. The relationship between foot and ankle symptoms and risk of developing knee osteoarthritis: Data from the osteoarthritis initiative. Osteoarthritis Cartilage 2017;25:639-46. [Google Scholar | PubMed]
- 9.Andriacchi TP. Dynamics of knee malalignment. Orthop Clin North Am 1994;25:395-403. [Google Scholar | PubMed]
- 10.Miyazaki T, Wada M, Kawahara H, Sato M, Baba H, Shimada S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum Dis 2002;61:617-22. [Google Scholar | PubMed]
- 11.Sharma L, Hurwitz DE, Thonar EJ, Sum JA, Lenz ME, Dunlop DD, et al. Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum 1998;41:1233-40. [Google Scholar | PubMed]
- 12.Pal CP, Singh P, Chaturvedi S, Pruthi KK, Vij A. Epidemiology of knee osteoarthritis in India and related factors. Indian J Orthop 2016;50:518-22. [Google Scholar | PubMed]
- 13.Donatelli RA. Abnormal biomechanics of the foot and ankle. J Orthop Sports Phys Ther 1987;9:11-6. [Google Scholar | PubMed]
- 14.Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: A theoretical model. J Orthop Sports Phys Ther 1987;9:160-5. [Google Scholar | PubMed]
- 15.Guichet JM, Javed A, Russell J, Saleh M. Effect of the foot on the mechanical alignment of the lower limbs. Clin Orthop Relat Res 2003;415:193-201. [Google Scholar | PubMed]
- 16.Reilly K, Barker K, Shamley D, Newman M, Oskrochi GR, Sandall S. The role of foot and ankle assessment of patients with lower limb osteoarthritis. Physiotherapy 2009;95:164-9. [Google Scholar | PubMed]
- 17.Levinger P, Menz HB, Fotoohabadi MR, Feller JA, Bartlett JR, Bergman NR. Foot posture in people with medial compartment knee osteoarthritis. J Foot Ankle Res 2010;3:29. [Google Scholar | PubMed]
- 18.Gross KD, Felson DT, Niu J, Hunter DJ, Guermazi A, Roemer FW, et al. Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care Res (Hoboken) 2011;63:937-44. [Google Scholar | PubMed]
- 19.Woźniacka R, Bac A, Matusik S, Szczygieł E, Ciszek E. Body weight and the medial longitudinal foot arch: High-arched foot, a hidden problem? Eur J Pediatr 2013;172:683-91. [Google Scholar | PubMed]
- 20.Silverwood V, Blagojevic-Bucknall M, Jinks C, Jordan JL, Protheroe J, Jordan KP. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthritis Cartilage 2015;23:507-15. [Google Scholar | PubMed]
- 21.Hakukawa S, Kaneda K, Oki S, Harato K, Yamada Y, Niki Y, et al. Knee varus alters three-dimensional ankle alignment in standing-a study with upright computed tomography. BMC Musculoskelet Disord 2022;23:321. [Google Scholar | PubMed]
- 22.Zhang M, Nie MD, Qi XZ, Ke S, Li JW, Shui YY, et al. A strong correlation between the severity of flatfoot and symptoms of knee osteoarthritis in 95 patients. Front Surg 2022;9:936720. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Mid-term Functional Outcomes Following One-stage Single-Sitting Bilateral and Unilateral Unicompartmental Knee Arthroplasty: A 5-year Prospective Cohort Study
April 1, 2026 Mid-term Functional Outcomes Following One-stage Single-Sitting Bilateral and Unilateral Unicompartmental Knee Arthroplasty: A 5-year Prospective Cohort Study February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series
February 1, 2026 Outcome of Medial Open Wedge High Tibial Osteotomy for Knee Osteoarthritis: A Case Series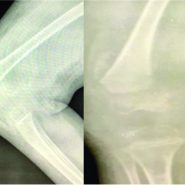 August 10, 2021 Scurvy Masquerading as Septic Arthritis in a Case of Cerebral Palsy
August 10, 2021 Scurvy Masquerading as Septic Arthritis in a Case of Cerebral Palsy May 10, 2020 Conversion Total Hip Arthroplasty Following Failed Hip Fracture Fixation in a Patient with Factor XI Deficiency: A Case Report
May 10, 2020 Conversion Total Hip Arthroplasty Following Failed Hip Fracture Fixation in a Patient with Factor XI Deficiency: A Case Report