
In extremely rare cases, post acute COVID-19 syndrome may manifest as osteonecrosis of the femoral head with concomitant septic arthritis with an unusual organism
Dr. Apurve Parameswaran, Department of Orthopaedics, Medicover Hospitals, Opposite Cyber Towers, Ibis Hotel Lane, HITEC City, Hyderabad - 500 081, Telangana, India. E-mail: doctorapurve@gmail.com
Abstract
Introduction: Among the various musculoskeletal manifestations of post-acute Coronavirus disease 2019 (COVID-19) syndrome, osteonecrosis and pyogenic infections are of serious concern due to their potential for joint destruction and the need for major surgery, even among young patients. Spontaneous septic arthritis is rare among healthy adults. Very few cases of osteonecrosis of the femoral heads (ONFH) with concomitant septic arthritis of the hip following a COVID-19 infection are reported in the literature.
Case Report: We report the case of a 43-year-old male patient, who presented with bilateral ONFHs and concomitant septic arthritis of the hips (caused by Pseudomonas aeruginosa), 8 weeks following a severe COVID-19 infection. His serum inflammatory markers were elevated. Radiologic findings were equivocal, and suggestive of osteonecrosis, with possible septic arthritis of the hip. In view of disabling end-stage arthritis, he was advised bilateral total hip arthroplasty (THA), in one or two stages, depending on the intraoperative findings. The diagnosis of infection was confirmed through intraoperative frozen section analysis. Bilateral two-staged THA was performed. At 3 years’ follow-up, the patient had no recurrence of symptoms, and was found to be doing well, with a Harris Hip Score of 93 points, and no limb length discrepancy.
Conclusion: COVID-19 infection predisposes patients to the development of ONFH. Concomitant septic arthritis of the hip, however, is scarcely reported, and needs to be ruled out in cases with rapid progression of symptoms.
Keywords: Severe acute respiratory syndrome, Coronavirus disease 2019, osteonecrosis, septic arthritis, post-acute Coronavirus disease 2019 syndrome.
Coronavirus disease 2019 (COVID-19) patients usually return to a seronegative state within 3–5 weeks following the onset of infection. Some patients, however, develop “post-acute COVID-19 syndrome” (PACS), a condition manifested through systemic pathology for several months following recovery [1]. Among the various musculoskeletal manifestations of PACS, osteonecrosis and pyogenic infections are of serious concern, due to their potential for rapid joint destruction [2]. COVID-19 predisposes patients to the development of osteonecrosis of the femoral head (ONFH) [3]. Reports of ONFH with concomitant septic arthritis of the hip, however, are rare [4,5], and involve infections with unusual and opportunistic organisms. We hereby report a case of bilateral ONFH with concomitant septic arthritis (caused by Pseudomonas aeruginosa) of hips following a severe COVID-19 infection, in an adult with no prior medical comorbidities. He underwent bilateral staged total hip arthroplasty (THA), and was found to be doing well at 2 years’ follow-up. The patient has given his informed consent for publication of the case report.
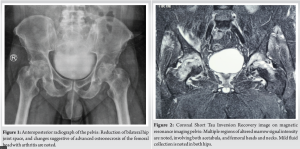
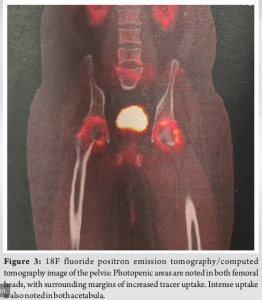
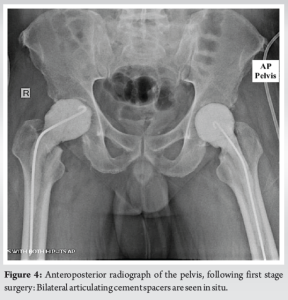
A 43-year-old male, teacher by profession, with no medical comorbidities, presented with complaints of bilateral groin pain for 2 months. The pain was progressive, and aggravated by hip movement and weight bearing. The patient used over-the-counter analgesics advised by a local physician initially, but presented to us since the pain continued to deteriorate till he was unable to bear weight. He had a history of hospitalization for a severe COVID-19 infection in 2020, 4 months before his presentation at our out-patient clinic. He required intensive care unit admission, oxygen support, and intra-venous corticosteroid medications at the time. He was discharged after 2 weeks in a stable condition. He was advised oral steroid at discharge, which was tapered over the following 4 weeks. Two weeks following discontinuation of the medication, he started developing bilateral groin pain. On examination, the patient was mildly febrile. Tenderness was elicited over the anterior and posterior hip joint lines, and hip movement was painful and restricted bilaterally. No clinical abnormality was noted over any other joints. Radiographs revealed symmetric reduction of the hip joint space bilaterally, with cystic changes in the femoral heads (Fig. 1). On investigation, his erythrocytic sedimentation rate (ESR) (80 mm/1st h; normal range: 0–10 mm/1st h) and C-reactive protein (CRP) (42.71 mg/L; normal range: 0.0–5.0 mg/L) levels were elevated; however, rheumatoid factor, anti-nuclear antibody profile, serum uric acid, and total leukocytic count were normal. Magnetic resonance imaging revealed changes suggestive of avascular necrosis (Fig. 2). Multiple subchondral serpiginous lines and geographic areas of altered marrow signal intensity were noted, involving both acetabula, and femoral heads and necks. Trace fluid was noted in the joint space bilaterally. Edema was noted within the glutei and the iliacus tendons. The patient was advised 18F-fluoride positron emission tomography/computed tomography (PET/CT), which showed photopenic areas in both femoral heads with surrounding margins of increased tracer uptake. Intense 18F fluoride uptake was also noted in both acetabular margins, suggesting the possibility of septic arthritis (Fig. 3).
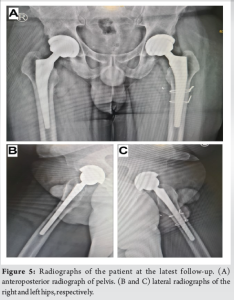
Considering the end-stage, disabling arthritis of the hips, it was concluded that the patient required bilateral THA. In the absence of a confirmed diagnosis, with the possibility of septic arthritis as indicated by the PET/CT scan, ultrasound-guided hip aspiration was attempted, but only resulted in a dry tap on both sides. The patient was counseled about the need for bilateral THA, in one or two stages depending on the intraoperative findings. The more painful left hip was operated first, using the posterior approach. Arthrotomy revealed minimal fluid, but extensive thickened synovium. The femoral head was deformed with areas of necrosis, and covered with granulation tissue. The suspicious tissue was sent for frozen section, which revealed the presence of over 20 cells per high power field, confirming the diagnosis of infection. Two-staged THA was planned. The femoral head was excised, and a thorough synovectomy, debridement and wash were performed. Tissue was sent for culture and sensitivity. An articulating vancomycin-impregnated cement spacer was placed in situ. The joint was closed over an indwelling pig-tail catheter for local antibiotic delivery [6]. Similar intraoperative findings were noted in the right hip, and a similar procedure was performed over the right side (Fig. 4). The patient was empirically started on intra-venous cefipime and ciprofloxacin, along with vancomycin injections through the pig-tail catheter following surgery. Culture and sensitivity revealed the growth of P. aeruginosa sensitive to colistin, imipenem, meropenem, amikacin, and ciprofloxacin. Accordingly, the patient was advised colistin injections through the pig-tail catheter for 2 weeks, along with intravenous meropenem and oral ciprofloxacin for 6 weeks.
ESR and CRP were monitored biweekly. Their decreasing trend stabilized at 8 weeks following surgery. Second stage surgery (bilateral spacer removal and uncemented THA) was planned after an additional 8 weeks, to permit general recovery of the patient. During revision surgery, a crack occurred at the calcar while broaching on the left side. Hence, additional cerclage wiring was performed. Intraoperative tissue samples were sent for culture and sensitivity, and revealed no microbial growth. The patient was advised intravenous meropenem and oral ciprofloxacin for 2 weeks following surgery. He did not have subsequent recurrence of symptoms. At 3 years’ follow-up, the patient was found to be doing well, with a Harris Hip Score of 93 points, and no limb length discrepancy (Fig. 5).
The outbreak of severe acute respiratory syndrome (SARS) early in 2003 led to a considerable proportion of patients developing musculoskeletal sequelae, including arthralgia and osteonecrosis [7]. Likewise, the recent COVID-19 pandemic resulted in a large proportion of recovered patients manifesting multi-system pathologies, up to several months following resumption of seronegativity for SARS-CoV2. This phenomenon, originally termed “Long COVID,” is now recognized as PACS [1]. Over 50 long-term effects of COVID-19 have been reported, of which fatigue, headache, attention disorder, hair loss and dyspnea are the most common [8]. Musculoskeletal manifestations of PACS range from self-limiting myalgia and arthralgia, to more serious pathology such as osteonecrosis or pyogenic infections [2]. Given the large number of COVID-19 cases the world has seen in recent times, PACS is likely to be encountered for some time to come, despite the decreased incidence of acute infection. An understandable limitation of most literature from the time of the pandemic is that case reports and series did not present follow-up data of clinical outcomes, since the focus was on creating awareness regarding the possibility of various COVID-19 sequelae. Our case report presents the findings and management in a rare presentation of PACS, along with the clinical outcome following 3 years of treatment. Osteonecrosis (or “avascular necrosis”) refers to in situ death of a bone segment due to interruption of blood supply to the bone [9]. Among multiple reported contributory factors, the cumulative dose of steroid is considered the most important risk factor for predicting development of osteonecrosis [7]. Though a cumulative dose of 2000 mg of prednisolone (or its equivalent) is generally considered the safe ceiling to prevent development of osteonecrosis [10], post-COVID-19 ONFH has been reported to occur despite corticosteroid doses as low as 400 mg of prednisolone equivalent [11]. COVID-19 results in a hypercoagulable state and endothelial dysfunction leading to thrombotic microangiopathy, which could lead to early onset osteonecrosis despite lower doses of corticosteroids [3,9]. Although symptoms of ONFH usually develop 6 months to a year following the start of corticosteroid medications [9], our patient developed bilateral symptoms 2 months after the diagnosis of COVID-19. Infectious arthritis is the most destructive form of arthritis. Spontaneous septic arthritis however, is rarely seen in healthy adults. Jain and Sawant [9] reported a case of bilateral ONFHs, with concomitant Escherichia coli infection in both hips, in a 42-year-old man. Ardakani et al. [4], Salehi et al. [5] reported five cases of femoral head osteonecrosis with septic arthritis of the hip (caused by non-tyhoid group D Salmonella, Serratia marcescens, and coagulase positive staphylococci). To the best of our knowledge, there are no other similar reports in the literature. Our patient presented with bilateral septic arthritis due to P. aeruginosa, which is both virulent and uncommon. The course of COVID-19 infection and the use of corticosteroid medications in its management, lead to the occurrence of osteonecrosis in a set of patients, which could create a favorable environment for infection with unusual and opportunistic pathogens. We believe that the possibility of bacterial infection must be considered and investigated for all patients presenting with symptoms of femoral head osteonecrosis, before planning primary arthroplasty. There were multiple challenges pertaining to the diagnosis of septic arthritis in our case. At the onset of symptoms, the patient was advised analgesics and rest by a local physician, probably in view of the possibility of reactive arthritis following COVID-19 infection. The patient subsequently presented to us, with a prolonged and progressive course of symptoms, which would indicate the probability of osteonecrosis. Radiographs showed symmetric reduction of the hip joint space bilaterally, which was consistent with this initial diagnosis. However, due to the mildly febrile status of the patient at the time of presentation, he was investigated for the possibility of septic arthritis. Although his ESR and CRP values were elevated, they were not adequate to confirm or rule out infection, as these inflammatory markers have been found to remain considerably elevated even 3 months following recovery from COVID-19 infection [12]. MRI findings were equivocal, with no frank collection in the joint. PET/CT findings were suggestive of septic arthritis. Ultrasound guided hip aspiration was attempted, but resulted in a dry tap bilaterally. Surgery was planned, and a frozen section eventually confirmed the diagnosis, following which bilateral staged THA was executed. The patient had no complaints and was found to be doing well at his 3 years’ follow-up.
Septic arthritis can result in rapid irreversible joint destruction, especially in deep-seated joints like the hips, considering the lower probability of appreciating subtle clinical findings such as warmth and swelling. Despite the high likelihood of persistent hip-related symptoms following COVID-19 infection resulting from reactive arthritis, triggering of rheumatoid diseases, or ONFH, an awareness of the possibility of pyogenic infections is necessary. When pre-operative investigations results are equivocal, surgeons must rely on intraoperative findings and frozen sections to appropriately manage these patients.
Among the various manifestations of PACS, osteonecrosis and pyogenic infections are of particular concern. In rare cases, ONFH resulting from COVID-19 infection and the corticosteroids used in its management may create a favorable environment for the development of concomitant septic arthritis, thereby presenting a diagnostic challenge with equivocal investigation reports. Appropriate pre-operative counseling and frozen section analysis can help confirm or rule out pyogenic infections in these cases.
References
- 1.Chiappelli F, Fotovat L. Post acute CoViD-19 syndrome (PACS)-long CoViD. Bioinformation 2022;18:908-11. [Google Scholar | PubMed]
- 2.Pires RE, Reis IG, Waldolato GS, Pires DD, Bidolegui F, Giordano V. What do we need to know about musculoskeletal manifestations of COVID-19?: A systematic review. JBJS Rev 2022;10(6):e22.00013. [Google Scholar | PubMed]
- 3.Shetty L, Nahar S, Domah T, Raj AT. COVID-19 patients could be at high risk for dry socket. Med Hypotheses 2021;146:110462. [Google Scholar | PubMed]
- 4.Ardakani MV, Parviz S, Ghadimi E, Zamani Z, Salehi M, Firoozabadi MA, et al. Concomitant septic arthritis of the hip joint and femoral head avascular necrosis in patients with recent COVID-19 infection: A cautionary report. J Orthop Surg Res 2022;17:302. [Google Scholar | PubMed]
- 5.Salehi M, Nourbakhsh SM, Ardakani MV, Abdollahi A, Khaki PA, Aliramezani A. Bilateral hip septic arthritis caused by nontyphoidal Salmonella group D in a 16-year-old girl with COVID-19: A case report. Int J Surg Case Rep 2022;95:107202. [Google Scholar | PubMed]
- 6.Whiteside LA, Roy ME. One-stage Revision with catheter infusion of intraarticular antibiotics successfully treats infected THA. Clin Orthop Relat Res 2017;475:419-29. [Google Scholar | PubMed]
- 7.Griffith JF. Musculoskeletal complications of severe acute respiratory syndrome. Semin Musculoskelet Radiol 2011;15:554-60. [Google Scholar | PubMed]
- 8.Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, et al. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci Rep 2021;11:16144. [Google Scholar | PubMed]
- 9.Jain S, Sawant T. Osteonecrosis with concomitant bacterial osteomyelitis of both hips and a knee in a post-COVID-19 patient: A case report. JBJS Case Connect 2022;12(1):e21.00629. [Google Scholar | PubMed]
- 10.Banerjee I, Robinson J, Sathian B. Corticosteroid induced avascular necrosis and COVID-19: The drug dilemma. Nepal J Epidemiol 2021;11:1049-52. [Google Scholar | PubMed]
- 11.Agarwala SR, Vijayvargiya M, Pandey P. Avascular necrosis as a part of ‘long COVID-19’. BMJ Case Rep 2021;14:e242101. [Google Scholar | PubMed]
- 12.Gameil MA, Marzouk RE, Elsebaie AH, Rozaik SE. Long-term clinical and biochemical residue after COVID-19 recovery. Egypt Liver J 2021;11:74. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Case Report on Steroid-induced Bilateral Femoral Head Osteonecrosis with Concomitant Hip Septic Arthritis in Primary Membranous Nephropathy
February 1, 2026 Case Report on Steroid-induced Bilateral Femoral Head Osteonecrosis with Concomitant Hip Septic Arthritis in Primary Membranous Nephropathy July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report
July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult
July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult May 1, 2026 Traumatic Obturator Variant of Anterior Hip Dislocation – A Case Series
May 1, 2026 Traumatic Obturator Variant of Anterior Hip Dislocation – A Case Series