
Tumor may presents as acute fracture in uncommon sites.
Dr. Rohit Karthik, Department of Orthopaedics, Sree Balaji medical college and hospital, CLC works road, Shankar Nagar, Chromepet, Chennai-600044, Tamil Nadu, India. E-mail: rohotron@gmail.com
Abstract
Introduction: Giantcell tumour of ulna is a rare and benign neoplasm but is locally invasive tumour. Distal ulna Giant cell tumors have a reported incidence of 0.45 to 0.6%.
Case report: 43 years old female came with alleged History of slip and fall at her residence sustaining injury to right wrist and suspected to be a Giant cell tumor. The Giant cell tumour was treated with en bloc resection and curettage [Darrach’s procedure]. Patient was followed up for 6 months during which she regained full range of motion.
Conclusion: Giantcell tumor can masquerade as pathological fracture with En bloc Resection dramatically reducing the risk of recurrence.
Keywords: Giant cell tumor, Distal Ulna, Excision Biopsy
Giant cell tumor is the most common locally aggressive bone tumor that occurs mostly at the distal femur or proximal tibia, typically involving the epiphysis of the bone [1-3]. Clinically, it presents as insidious pain at the affected site that worsens with activity. Swelling and joint stiffness may also be present [2,4]. Radiologically, the tumor typically shows a characteristic “soap bubble” appearance [3,5], and diagnosis is confirmed with biopsy postoperatively [5]. Intraoperatively, after excision of the bony lesion, adjuvants are used to reduce recurrence [6,7]. Bone grafting or bone cementation is performed when there is a large defect post-excision [6]. Postoperatively, patients are immobilized with a splint for 2–3 weeks, followed by physiotherapy. By six months, patients typically show clinical and functional improvement with full range of motion and no pain at the operated site [6-10].
A 43-year-old female presented with complaints of pain and swelling in her right wrist for 15 days following a slip and fall inside a moving bus. She initially self-medicated with NSAIDs, but the pain persisted. On examination, a solitary, tender, bony-hard swelling measuring 4×2×1 cm was noted over the ulnar aspect of the right wrist without secondary skin changes [Fig. 1]. Wrist movements were preserved except for terminal pain in ulnar deviation and dorsiflexion [Table 1]. Radiographs revealed an epiphyseal lesion with metaphyseal extension at the distal ulna, displaying a geographic lytic pattern with a narrow zone of transition, soap bubble appearance, internal trabeculations, and a possible cortical breach [Fig. 2], consistent with findings reported by Goldenberg et al. [3] and Schajowicz [8]. CT confirmed focal cortical discontinuity [Fig. 3,4], while T2-weighted MRI demonstrated fluid-fluid levels, a feature noted in prior studies by Masui et al. [5] and Turcotte et al. [6] [Fig. 3]. Based on Enneking’s staging system, the lesion was classified as Stage 2 [active], and according to Campanacci grading, it was a Grade II lesion, indicating locally aggressive behavior with cortical thinning but without soft tissue extension [2].




Surgical management involved wide resection using the Darrach procedure [14] [Fig.s 5 and 6], followed by dynamic stabilization with extensor carpi ulnaris [ECU] tenodesis to the distal ulnar stump [Fig. 7], as described by Singh et al. [9] and Novel and Arafa [15]. A frozen section was performed intraoperatively to confirm negative margins before proceeding with definitive reconstruction, ensuring complete tumor clearance [10]. Following excision, hydrogen peroxide was used as a local chemical adjuvant within the cavity to reduce the risk of local recurrence, consistent with methods reported in prior studies [7]. Postoperatively, the patient was immobilized with an above-elbow splint for 4–5 weeks, followed by progressive wrist mobilization and strengthening through physiotherapy.



Follow-up was structured in accordance with established GCT surveillance guidelines [10,11]. Clinical evaluation and local radiographs were performed every 3 months for the first two years, then every 6 months for up to 5 years to monitor for local recurrence. Chest imaging [X-ray or CT] was conducted biannually during the first two years and annually thereafter to screen for pulmonary metastasis. Functional outcomes were assessed during each visit, with focus on wrist range of motion, grip strength, and any signs of recurrence. Patients were educated about early symptoms such as return of pain, swelling, or limited joint function.
At one-year follow-up, the patient had full, pain-free wrist motion [Fig. 8-12] without any clinical or radiological evidence of recurrence [Fig. 10], consistent with outcomes reported by Ward and Li [10].



Giant cell tumor [GCT] of bone is a benign yet locally aggressive tumor, constituting 4–5% of all primary bone tumors, with a predilection for young adults, especially females [1,4]. The distal radius and ulna are common sites, accounting for 10–12% of cases [11]. These tumors originate from mesenchymal stromal cells and exhibit osteolytic destruction, cortical breach, and soft tissue extension in aggressive cases [7,12]. Radiologically, GCTs show a characteristic soap bubble appearance with a narrow zone of transition, internal trabeculations, and an expansile nature, as described by Goldenberg et al. [3] [Fig. 2]. MRI findings, including fluid-fluid levels, are useful in differentiating GCTs from aneurysmal bone cysts [5,6] [Fig. 3]. Enneking’s staging classifies GCTs into Stage 1 [latent], Stage 2 [active], and Stage 3 [aggressive], which influences surgical management decisions [2]. Similarly, Campanacci grading divides them into Grade I [latent], Grade II [active but contained within bone], and Grade III [aggressive with soft tissue extension] [2]. The lesion in this case was classified as Stage 2 [active] and Grade II, indicating a high risk of recurrence but without extraosseous invasion. Treatment strategies for GCTs range from intralesional curettage with adjuvant therapy to en bloc resection, depending on lesion grade and anatomical location [7,13]. Wide resection is preferred in cases involving extensive cortical breach or high recurrence risk [10] [Fig. 4]. The Darrach procedure, originally described for post-traumatic conditions, has been successfully adapted for tumors of the distal ulna [14] [Fig. 5, Fig. 6]. However, resection of the distal ulna can result in instability, necessitating reconstructive stabilization techniques. Extensor carpi ulnaris tenodesis is a well-established method to restore wrist stability post-resection, as highlighted by Singh et al. [9] and Novel and Arafa [15] [Fig. 7]. This approach allows preservation of wrist function while minimizing postoperative complications. Postoperative radiographs at two weeks [Fig. 8], six months [Fig. 9], and one year [Fig. 10] demonstrated no radioulnar convergence, confirming the efficacy of the stabilization procedure. Improvement in wrist mobility was noted at six months [Fig. 11, Table 2] and further optimized at one year [Fig. 12, Table 3].
Early recognition of GCT, particularly in patients with persistent pain and swelling post-trauma, is crucial to prevent misdiagnosis and delays in treatment. Radiological evaluation, including CT and MRI, plays a critical role in diagnosis and surgical planning. The Enneking and Campanacci grading systems provide a structured approach to assessing tumor behavior and determining appropriate treatment strategies. Surgical excision with proper stabilization, such as the Darrach procedure with ulnar tenodesis, ensures optimal functional recovery while minimizing complications. This case reinforces the importance of a tailored surgical approach in achieving successful long-term outcomes in patients with GCT of the distal ulna.
Giant cell tumors should be considered in patients with persistent wrist pain and swelling post-trauma, even in the absence of severe movement restriction. Radiological assessment, along with Enneking staging and Campanacci grading, aids in early diagnosis and treatment planning. Surgical excision with stabilization techniques like ulnar tenodesis can restore wrist function while preventing long-term instability.
References
- 1.Beebe-Dimmer JL, Cetin K, Fryzek JP, Schuetze SM, Schwartz K. The epidemiology of malignant Giant cell tumors of bone: an analysis of data from the Surveillance, Epidemiology and End Results Program [1975–2004] Rare Tumors. 2009;1:e52. [Google Scholar | PubMed]
- 2.Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am. 1987;69:106–114. [Google Scholar | PubMed]
- 3.Goldenberg RR, Campbell CJ, Bonfiglio M. Giant-cell tumor of bone. An analysis of two hundred and eighteen cases. J Bone Joint Surg Am. 1970;52:619–664. [Google Scholar | PubMed]
- 4.Sung HW, Kuo DP, Shu WP, Chai YB, Liu CC, Li SM. Giant-cell tumor of bone: analysis of two hundred and eight cases in Chinese patients. J Bone Joint Surg Am. 1982;64:755–761. [Google Scholar | PubMed]
- 5.Masui F, Ushigome S, Fujii K. Giant cell tumor of bone: a clinicopathologic study of prognostic factors. Pathol Int. 1998;48:723–729. [Google Scholar | PubMed]
- 6.Turcotte RE, Wunder JS, Isler MH, Bell RS, Schachar N, Masri BA, Moreau G, Davis AM. Canadian Sarcoma Group. Giant cell tumor of long bone: a Canadian Sarcoma Group study. Clin Orthop Relat Res. 2002;397:248–258 [Google Scholar | PubMed]
- 7.Prosser GH, Baloch KG, Tillman RM, Carter SR, Grimer RJ. Does curettage without adjuvant therapy provide low recurrence rates in Giant-cell tumors of bone? Clin Orthop Relat Res. 2005;435:211–218. [Google Scholar | PubMed]
- 8.Schajowicz F. Tumors and Tumor-like Lesions of Bone: Pathology, Radiology and Treatment. Springer-Verlag, ; 1994 [Google Scholar | PubMed]
- 9.Singh M, Sharma S, Peshin C, Wani IH, Tikoo A, Gupta SK, Singh D. Wide resection and stabilization of ulnar stump by extensor carpi ulnaris for Giant cell tumor of distal ulna: two case reports. Cases J. 2009;2:8617. doi: 10.4076/1757-1626-2-8617. [Google Scholar | PubMed | CrossRef]
- 10.Ward WG, Li G. Customized treatment algorithm for Giant cell tumor of bone: report of a series. Clin Orthop Relat Res. 2002;397:259–270. [Google Scholar | PubMed]
- 11.Akio Minami, Norimasa Iwasaki, Kinya Nishida, Makoto Motomiya, Katsuhisa Yamada, Daisuke Momma, "Giant-Cell Tumor of the Distal Ulna Treated by Wide Resection and Ulnar Support Reconstruction: A Case Report", Case Reports in Medicine, vol. 2010, Article ID 871278, 4 pages, 2010. [Google Scholar | PubMed]
- 12.D. J. McDonald, F. H. Sim, R. A. McLeod, and D. C. Dahlin, “Giant-cell tumor of bone,” Journal of Bone and Joint Surgery. Series A, vol. 68, no. 2, pp. 235–242, 1986. [Google Scholar | PubMed]
- 13.W. P. Cooney, T. A. Damron, F. H. Sim, and R. L. Linscheid, “En bloc resection of tumors of the distal end of the ulna,” Journal of Bone and Joint Surgery. Series A, vol. 79, no. 3, pp. 406–412, 1997. [Google Scholar | PubMed]
- 14.P. V. Dingman, “Resection of the distal end of the ulna [Darrach operation]. An end result study of twenty four cases,” The Journal of Bone and Joint Surgery, vol. 34, no. 4, pp. 893–900, 1952. [Google Scholar | PubMed]
- 15.J. Novel and M. Arafa, “Stabilization of distal ulna after excessive Darrach’s procedure,” The Hand, vol. 15, pp. 70–72, 1983. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Optimizing Functional Recovery in Multi-Site Giant Cell Tumors
September 1, 2025 Optimizing Functional Recovery in Multi-Site Giant Cell Tumors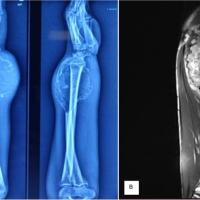 June 10, 2024 Huge Distal Ulna Giant Cell Tumor Treated with Wide Local Excision and Extensor Carpi Ulnaris Tenodesis – A Rare Case Report
June 10, 2024 Huge Distal Ulna Giant Cell Tumor Treated with Wide Local Excision and Extensor Carpi Ulnaris Tenodesis – A Rare Case Report August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization
August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization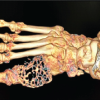 June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction
June 1, 2026 A Rare Case of Giant Cell Tumor of the First Metatarsal: En Bloc Resection and Fibular Autograft Reconstruction