
A giant cell tumour of the first metatarsal is an exceptionally rare clinical entity that requires a high index of suspicion and multimodal imaging for diagnosis. For Grade 3 lesions with extensive bone destruction, en bloc resection followed by non-vascularised fibular autograft reconstruction provides an oncologically sound treatment that restores biomechanical stability and yields good functional outcomes.
Dr. Nikhil Agrawal, Department of Orthopaedics, All India Institute of Medical Sciences, New Delhi, India. Email: nikhilagrawalwork1503@gmail.com
Abstract
Introduction: Giant cell tumours (GCTs) of bone are benign but locally aggressive neoplasms that predominantly involve the epiphyseal regions of long bones, with the first metatarsal being an exceptionally rare site of involvement. This case report describes the clinical presentation, diagnostic evaluation, surgical management, and functional outcomes of a rare GCT involving the first metatarsal bone.
Case Report: A 54-year-old female presented with a 5-month history of progressive pain and swelling of the right foot localised over the first metatarsal region. Clinical examination revealed a firm, tender, bony expansion measuring approximately 3 × 5 × 3 cm. Radiological investigations, including plain radiography, multiplanar MRI and CT imaging, confirmed an osteolytic, expansile lesion suggestive of GCT. En bloc resection of the tumour-bearing segment was performed with reconstruction using non-vascularised fibular autograft fixation with K-wires. Histopathological examination confirmed the diagnosis of GCT of bone.
Results: The patient achieved complete surgical resection with excellent functional recovery at 12-month follow-up. The fibular autograft demonstrated satisfactory integration without evidence of recurrence or significant complications. Functional outcome scores improved significantly, and the patient resumed normal weight-bearing activities.
Conclusion: Although rare, GCT of the first metatarsal should be considered in the differential diagnosis of expansile osteolytic lesions in the foot. En bloc resection with non-vascularised fibular autograft reconstruction provides oncologically sound treatment with acceptable functional outcomes and minimal recurrence rates. This case underscores the importance of multimodal imaging, histopathological confirmation, and meticulous surgical planning in managing this challenging presentation.
Keywords: Giant cell tumor, first metatarsal, en bloc resection, bone graft, benign bone neoplasm.
Giant cell tumours (GCTs) of bone represent 3–5% of all primary bone tumours and typically manifest as benign but locally aggressive lesions affecting the epiphyseal and metaphyseal regions of long bones [1]. The tumour predominantly involves the distal femur (30%), proximal tibia (25%), and distal radius (10%), with a strong predilection for the 2nd to 4th decades of life and female predominance (female-to-male ratio approximately 1.3:1) [2]. The characteristic histological feature consists of round-to-oval multinucleated giant cells interspersed with mononuclear stromal cells, haemosiderin-laden macrophages, and focal haemorrhage. Involvement of the first metatarsal bone by GCT represents an exceptionally rare occurrence. The metatarsals are typically spared from GCT involvement, constituting <1% of all documented cases [3]. This unusual anatomical presentation poses significant diagnostic challenges and requires high clinical suspicion, particularly in endemic regions. The diagnosis is frequently delayed due to the atypical location and the rarity of the condition, potentially leading to increased local destruction and functional impairment. The clinical significance of this case lies in its rare anatomical location. The first metatarsal bone is critical for the biomechanical function of the foot, bearing significant weight during ambulation and providing stability during the propulsive phase of gait. Involvement at this location necessitates careful surgical planning to balance oncological principles with functional preservation.
Pathological characteristics:
GCTs are locally aggressive lesions characterised by rapid growth potential and a propensity for recurrence following inadequate treatment. The Campanacci grading system is widely employed to classify these tumours based on radiological criteria: Grade 1 lesions demonstrate well-demarcated margins without cortical breakthrough; Grade 2 lesions show cortical thinning or subtle cortical breakthrough, and grade 3 lesions exhibit extensive cortical destruction with soft tissue extension [1]. The surgical approach is typically guided by this grading system, with Grade 1 and 2 lesions amenable to intralesional curettage, whereas Grade 3 lesions with extensive bone destruction are better treated with wide excision or en bloc resection.
Epidemiology and clinical context:
Although GCT commonly affects the knee region, presentation in the foot bones is exceptionally uncommon. The anatomical rarity of metatarsal involvement, combined with complex biomechanical demands of the first ray, makes surgical decision-making more complex than typical GCT cases. Published literature documenting GCT of the first metatarsal remains sparse, with only a handful of case reports describing this presentation [3,4].
Clinical history:
A 54-year-old female presented to the Department of Orthopaedic Surgery with a 5-month history of progressive pain and swelling of the right foot, localised to the medial midfoot. The patient initially attributed the symptoms to footwear irritation and attempted conservative management with rest and analgesia without symptomatic improvement. Symptoms progressively worsened, with the swelling becoming increasingly firm and the pain becoming more constant, particularly with weight-bearing activities. There was no documented history of antecedent trauma to the foot. The patient specifically denied systemic symptoms, including fever, unintentional weight loss, night sweats, or loss of appetite. Medical history was unremarkable with no significant systemic comorbidities or prior orthopaedic pathology. (Fig. 1).

Figure 1: Pre-operative images of right foot.
Physical examination:
Clinical examination revealed a well-circumscribed, firm, non-mobile bony enlargement measuring approximately 3 × 5 × 3 cm over the medial aspect of the right foot at the level of the first metatarsal base and shaft. The overlying skin was normal without erythema, warmth, or ulceration. Palpation elicited tenderness directly over the lesion. A notable firm, tender mass was detected. Active range of motion of the first metatarsophalangeal joint was maintained but associated with localised discomfort. Weight-bearing on the right foot was tolerated with an antalgic gait pattern. Neurovascular examination revealed intact foot pulses, normal capillary refill, and intact sensory perception in the distribution of the superficial peroneal and sural nerves. No lymphadenopathy was appreciated.
Imaging findings:
Plain radiography:
Anteroposterior, lateral, and oblique radiographs of the right foot revealed a well-defined osteolytic lesion centred within the first metatarsal bone, extending from the base to the distal shaft. The lesion demonstrated cortical breakthrough and marginal scalloping, with internal trabecular destruction. There was evidence of cortical expansion without soft tissue calcification. (Fig. 2).

Figure 2: Pre-operative X-ray images of right foot – AP and oblique view.
Computed tomography:
High-resolution CT imaging with multiplanar reconstruction demonstrated an expansile, well-circumscribed lesion involving the first metatarsal with predominantly lytic characteristics. The lesion measured approximately 3.2 × 4.8 × 3.1 cm in maximum dimensions. There was an evident cortical breakthrough on the medial and plantar aspects of the metatarsal with thin cortical margins elsewhere. The lesion showed inhomogeneous density with areas of low attenuation, suggesting fluid levels. No periosteal new bone formation was appreciated. Soft tissue extension was minimal without involvement of adjacent anatomical structures.
Magnetic resonance imaging:
Multiplanar magnetic resonance imaging (MRI) of the right foot with a high-field 1.5-tesla system and dedicated foot coil demonstrated the lesion to be predominantly hyperintense on T2-weighted sequences with multiple internal areas of T2 hypointensity suggestive of hemosiderin-laden macrophages and previous haemorrhage. T1-weighted post-gadolinium sequences revealed a heterogeneous enhancement pattern. The lesion was well-circumscribed with clear demarcation from adjacent soft tissues. No apparent involvement of the first metatarsocuneiform articulation was noted on coronal imaging. Perilesional oedema within the marrow spaces of adjacent tarsal bones was minimal. (Fig. 3).
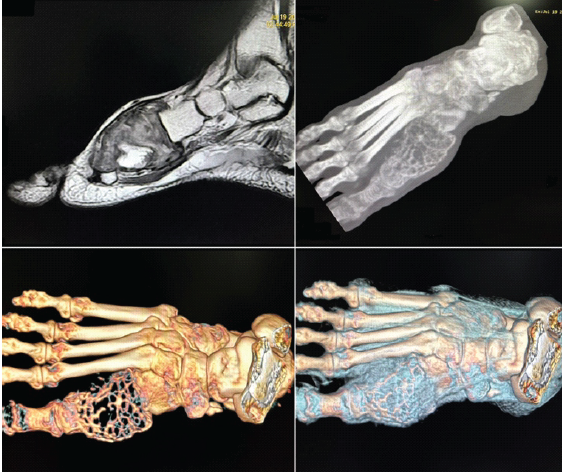
Figure 3: MRI and screening CT scan of the right foot showing a well-defined, osteolytic, expansile and benign lesion, most likely a giant cell tumor.
Differential diagnosis:
The radiological presentation was consistent with several entities: (1) GCT – the primary consideration given the epiphyseal involvement, lytic character, and age demographic; (2) Aneurysmal bone cyst – less likely given the heterogeneous enhancement and lack of rapid growth history; (3) Clear cell sarcoma – histologically distinct and typically demonstrates more aggressive biological behaviour; (4) Chondroblastoma – typically found in younger patients and more commonly involves the distal femoral epiphysis. Histopathological confirmation was deemed essential for definitive diagnosis and to exclude malignant alternatives, particularly given the unusual anatomical location.
Surgical management and intraoperative findings:
Preoperative planning:
Given the extensive radiological destruction (Campanacci Grade 3), intralesional curettage was deemed inadequate, and en bloc resection was planned. The surgical strategy aimed to achieve complete tumour removal while minimising functional compromise. Reconstruction planning included harvesting a non-vascularised fibular autograft from the ipsilateral lower extremity to restore structural continuity and mechanical support.
Surgical technique:
The patient was positioned supine under spinal anaesthesia. A longitudinal medial incision was made over the first metatarsal, approximately 6–7 cm in length, centred over the visible bony prominence. Careful soft tissue dissection revealed the well-circumscribed tumour mass causing cortical expansion. The tumour appeared as a firm, greyish-white tissue with evidence of cystic degeneration and haemorrhagic infiltration. Intraoperative assessment confirmed extensive cortical destruction and expansion without appreciable soft tissue mass beyond the bone. En bloc resection was performed, removing the tumour-bearing segment of the first metatarsal. A 6–7 cm segment of fibular graft was harvested from the ipsilateral fibula from a point approximately 10 cm below the fibular head, and reconstruction was done using a non-vascularised fibular autograft. Fixation of autograft was done using K wires. The vascular integrity of the foot was preserved throughout the dissection, and specific care was taken to protect the dorsalis pedis artery and its branches. Wound closure was performed in layers with careful attention to haemostasis. A sterile compression dressing was applied, and the foot was immobilised in a short-leg posterior slab cast. A histological specimen was submitted for analysis. (Fig. 4).

Figure 4: Intraoperative picture showing reconstruction with fibula autograft.
Operative specimen:
The excised tissue measured 5.8 × 2.1 × 1.9 cm. The specimen demonstrated focal areas of brown discolouration consistent with haemorrhage. The bone was predominantly lytic with cortical breakthrough. On sectioning, the tumour tissue was tan-white with areas of cystic degeneration containing blood-stained fluid. No areas of obvious necrosis were appreciated. (Fig. 5).
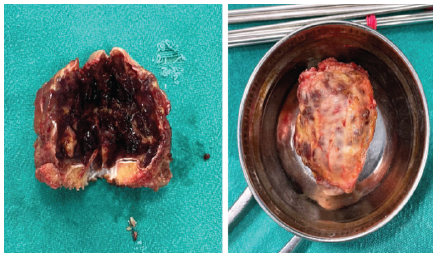
Figure 5: Intraoperative pictures of the resected specimen.
Histopathological findings:
Microscopic examination of the resected specimen revealed a benign lesion consistent with GCT of bone. The tumour was composed of numerous multinucleated giant cells (osteoclast-like) with round-to-oval morphology and abundant cytoplasm containing multiple nuclei. The giant cells were interspersed among mononuclear stromal cells with oval nuclei and amphophilic cytoplasm. Hemosiderin-laden macrophages were numerous throughout. Areas of a haemangiosarcoma-like pattern were present but without cytological atypia or mitotic activity. The lesion lacked the presence of any caseating granulomas, excluding tuberculous or fungal aetiology. Immunohistochemical analysis (not performed in this case but standard confirmation) would demonstrate positive staining for alkaline phosphatase and mild positivity for p63. The diagnosis of GCT of bone was confirmed. (Fig. 6).
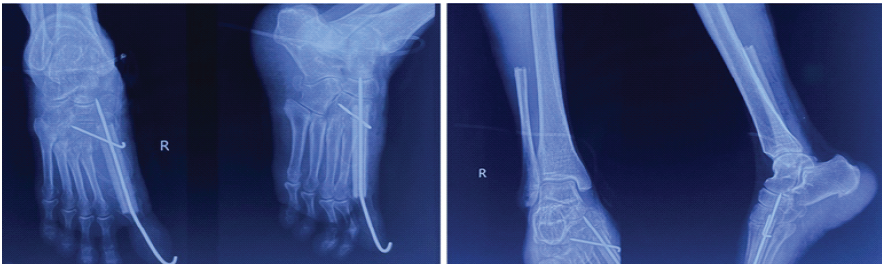
Figure 6: Post-operative X-ray of right foot – anteroposterior (AP) and oblique view and X-ray ankle with leg – AP and lateral view showing reconstruction using fibula autograft and fixation using K wires.
GCTs represent a significant proportion of benign bone tumours, yet their occurrence in metatarsal bones remains exceptionally rare [3,4]. The anatomical distribution of GCT typically follows the pattern of greater propensity for epiphyseal involvement in weight-bearing long bones. The first metatarsal, despite being a critical bone for locomotion and weight-bearing, appears to be remarkably resistant to GCT involvement [5]. This unusual presentation mandates careful consideration in the differential diagnosis of any expansile lytic lesion in the metatarsal bones, as delayed recognition may result in unnecessary diagnostic procedures or inappropriate treatment delays [4]. The diagnosis of GCT relies on integration of clinical presentation, radiological features, and histopathological confirmation [1]. Radiologically, GCT typically presents as a well-demarcated, eccentric, epiphyseal or metaphyseal osteolytic lesion with cortical expansion or breakthrough. The presence of internal trabeculation may impart a “soap bubble” or “honey comb” appearance on radiographs [6]. In this case, the radiological findings were entirely consistent with GCT, though the metatarsal location represented a diagnostic rarity that required correlation with clinical context and histology for confident diagnosis. MRI plays an increasingly important role in the pre-operative assessment of GCT [7]. The characteristic MRI appearance includes hyperintensity on T2-weighted sequences with areas of hypointensity reflecting haemosiderin deposition from previous haemorrhagic episodes. The pattern of enhancement following gadolinium administration is typically heterogeneous, reflecting the stromal cellular component and areas of cystic change. These imaging features were all evident in this case and proved invaluable for surgical planning. The management of GCT remains controversial, with ongoing debate regarding the optimal balance between recurrence prevention and functional preservation [8]. Intralesional curettage preserves articular anatomy and offers superior functional outcomes but carries recurrence rates ranging from 11% to 65% depending on surgical technique, use of adjuvants, and extent of bone destruction [1]. In contrast, wide excision or en bloc resection sacrifices articular anatomy but provides recurrence rates typically below 10% [3]. In this patient, the extensive cortical destruction (Campanacci Grade 3) made intralesional curettage inappropriate. En bloc resection was justified despite the functional concerns about metatarsal reconstruction. The first metatarsal’s critical role in weight-bearing and push-off during ambulation necessitated reconstruction to maintain foot biomechanics and prevent post-operative disabilities [9]. Following metatarsal reconstruction, patients typically demonstrate gradual functional recovery over 6–12 months [4]. Early weight-bearing protocols with appropriate orthotic support facilitate graft incorporation while minimising stress shielding. Given these complex biomechanical demands, a vigilant and structured postoperative rehabilitation protocol is essential to ensure long-term stability. Although this patient demonstrated excellent functional recovery at 12-month follow-up with return to normal weight-bearing activities, longer-term surveillance is required to assess for graft incorporation and detect any signs of recurrence. Functional scores, such as the American Orthopaedic Foot and Ankle Society score and the Musculoskeletal Tumour Society score, can be used in future studies to objectively quantify long-term mechanical and functional recovery.
Recurrence and surveillance:
Recurrence rates following en bloc resection are significantly lower than intralesional approaches, typically ranging from 0% to 10% [1]. However, vigilant long-term surveillance remains essential, particularly given the rarity of this tumour type at this location. Clinical examination for local swelling and serial radiological imaging at 6-month to annual intervals for the first 5 years post-treatment is recommended [10]. Any recurrent symptoms warrant urgent imaging and clinical reassessment.
Although exceptionally rare, GCT of the first metatarsal should be included in the differential diagnosis of expansile osteolytic foot lesions. A definitive diagnosis requires the integration of multimodal imaging (X-ray, CT, and MRI) and mandatory histopathological confirmation to exclude malignancy. For Campanacci grade 3 lesions, en bloc resection with non-vascularised fibular autograft reconstruction provides an oncologically sound treatment strategy. This approach effectively restores biomechanical stability, resulting in excellent functional recovery and minimal recurrence.
GCT of the first metatarsal is highly atypical; however, for aggressive Campanacci grade 3 lesions, complete en bloc resection paired with an autologous fibular graft offers an optimal balance between oncological clearance and anatomical reconstruction.
References
- 1. Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am 1987;69:106-14. [Google Scholar] [PubMed]
- 2. Szendröi M. Giant-cell tumour of bone. J Bone Joint Surg Br 2004;86:5-12. [Google Scholar] [PubMed]
- 3. Prashant K, Bhattacharyya TD, Frank H, Ram P. An unusual case of giant cell tumor of first metatarsal: A rare case report and review of literature. J Orthop Case Rep 2016;6:3-6. [Google Scholar] [PubMed]
- 4. Florio M, Careri S, Zoccali C, Aulisa AG, Falciglia F, Toniolo RM, et al. Reconstruction of metatarsal bone after giant cell tumor resection with no vascularized fibular graft in a pediatric patient: Case report and review of literature. Front Pediatr 2022;10:970309. [Google Scholar] [PubMed]
- 5. Wold LE, Doyle JR. Giant cell tumor of the bones of the hand. Am J Surg Pathol 1994;18:1081-92. [Google Scholar] [PubMed]
- 6. Kumta SM, Chow TC, Lee KM, Chiu KH, Ho EY, Capanna R, et al. Imaging of giant cell tumor of bone: Experience with 21 cases. Skeletal Radiol 2003;32:255-63. [Google Scholar] [PubMed]
- 7. Balke M, Ahrens H, Streitbürger A, Koehler G, Wegner D, Gosheger G, et al. Treatment options for giant cell tumor of bone. Curr Treat Options Oncol 2012;13:1-14. [Google Scholar] [PubMed]
- 8. Rock MG. Curettage and reconstruction for giant cell tumor of the distal radius. Hand Clin 2010;26:225-33. [Google Scholar] [PubMed]
- 9. Getty E, Mirra JM. Osteoclastoma (giant cell tumor) of bone. Orthop Clin North Am 2010;41:45-53. [Google Scholar] [PubMed]
- 10. Lewinstein I, Georghiu A, Frim D, Lewis V. Giant cell tumor-a benign lesion with aggressive biological behavior. Case report and review. N Engl J Med 1994;330:1275-9. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Reconstruction of Recurrent First Metatarsal Giant Cell Tumor with Vascularized Metatarsal Transfer: Long-Term Functional Outcomes
January 1, 2026 Reconstruction of Recurrent First Metatarsal Giant Cell Tumor with Vascularized Metatarsal Transfer: Long-Term Functional Outcomes December 1, 2025 Recurrent Giant Cell Tumor of the Carpal Bones in an Adult Male Managed by En-bloc Excision, Extended Curettage, Bone Grafting, and all-Kirschner Wire Fixation: A Rare Case Report and Literature Review
December 1, 2025 Recurrent Giant Cell Tumor of the Carpal Bones in an Adult Male Managed by En-bloc Excision, Extended Curettage, Bone Grafting, and all-Kirschner Wire Fixation: A Rare Case Report and Literature Review September 1, 2024 Giant Cell Tumor of First Metatarsal: A Rare Case Report with Literature Review
September 1, 2024 Giant Cell Tumor of First Metatarsal: A Rare Case Report with Literature Review August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization
August 1, 2026 Extensive Giant Cell Tumor Involving Entire Tibia with Talar Extension and Pulmonary Metastases: Successful Limb Preservation with Denosumab and Angioembolization