
The risk of iatrogenic injury to the popliteal neurovascular bundle during lateral meniscus repair may be lower than previously reported. This is because its distance to the lateral meniscus posterior capsule increases with knee flexion, and lateral meniscus repair is performed with the knee flexed in the “figure-of-four” position.
Dr. Peter D Fabricant, Hospital for Special Surgery, 535 East 70th Street, New York - 10021, USA. E-mail: fabricantp@hss.edu
Abstract
Introduction: The incidence of pediatric meniscal tears and their surgical repair has risen, with complications including iatrogenic injury to the popliteal neurovascular (NV) bundle posing notable risks, particularly during posterior horn lateral meniscus (PHLM) repair. Studies have assessed the PHLM-popliteal NV bundle distance using magnetic resonance imaging (MRI) or cadaveric approaches, but these methods often fail to replicate surgical conditions, such as the knee’s figure-of-four position at 90° flexion.
Case Report: A 17-year-old male presented with a locked knee at 90° of flexion due to a displaced bucket-handle lateral meniscus tear sustained while wrestling, which was managed with arthroscopic meniscus repair. On preoperative MRI in 90° of flexion, the lateral meniscus posterior capsule to popliteal artery distance measured 15.1 mm. Postoperative MRI with knee in relative extension demonstrated a distance of 5.8 mm.
Conclusion: The distance between the lateral meniscus posterior capsule and the popliteal NV bundle appears to increase with increasing knee flexion. Thus, the proximity of the NV bundle to the posterior capsule (and therefore the risk of iatrogenic injury during meniscal repair) may be lower than previously reported.
Keywords: Posterior horn lateral meniscus repair, iatrogenic injury, knee flexion.
Meniscal tears in pediatric populations have been continually rising in incidence, as has the incidence of surgical repair [1,2]. While complications of meniscal repair in children are rare, there is a risk of arthrofibrosis, complex regional pain syndrome, and neurovascular (NV) injury, particularly to the popliteal NV bundle when suturing the posterior horn of the lateral meniscus [1]. To better understand the risk of iatrogenic injury to the popliteal NV bundle during meniscus repair, studies have attempted to measure the distance of the posterior capsule and posterior horn of the lateral meniscus (PHLM) to the popliteal NV bundle [3-7]. In one study, the measured distances between the most anterior edge of the PHLM and the popliteal NV bundle were frequently less than the maximum depth of all-inside meniscal repair devices [8]Due to the proximity of these two structures and the risk of iatrogenic injury as demonstrated in these studies, authors have proposed a need for modification of standard techniques during PHLM all-inside meniscus repair such as the use of accessory portals [3-5]. To date, however, studies measuring the PHLM-popliteal NV bundle distance have differed significantly in their strategies using either magnetic resonance imaging (MRI) or cadaveric approaches. These studies are limited in that they may not be representative of the true anatomical distance during surgery. During standard all-inside meniscus repair of the PHLM, the patient’s knee is positioned in the figure-of-four position, where the knee is in approximately 90° of flexion. When measuring the distance from the NV bundle to the PHLM in living subjects, previous studies have relied on standard MRI with the knee in relative extension. Cadaveric studies have attempted to control for this by measuring the distance between NV structures and the lateral meniscus with the knee in flexion [9,10]. One adult cadaveric study demonstrated that the distance from the NV bundle to the PHLM increases significantly as knee flexion increases. This suggests that MRI studies with the knee in flexion may be underestimating this distance and that the figure-of-four position may minimize the risk of iatrogenic injury to the popliteal NV bundle during all-inside repair of the PHLM [9]. Additionally, another cadaveric study showed the proximity of various NV structures to the lateral meniscus in children 11 years old and younger. However, these cadaveric studies were performed in dry environments without fluid to distend the joint, and without the standard muscle bulk and tone of a living patient [10]. No study, to the authors’ knowledge has measured this distance in a living subject when the knee is in near full extension and in 90° of flexion. By better understanding the safe distance to the popliteal NV bundle, the safety of lateral meniscus repairs may be improved. Therefore, the purpose of this study was to report and compare the distance between the lateral meniscus posterior capsule and the popliteal NV bundle in a 17-year-old male using MRIs taken with the knee in full extension and 90° of flexion.
A 17-year-old male presented to our institution with a chief complaint of right knee pain after several weeks of knee “popping” during wrestling. On examination, his knee was locked at 90° of knee flexion with a range of motion of 80° of extension to 110° of flexion. The patient reported lateral joint line tenderness to palpation. Due to concern of a lateral meniscus tear in this patient with a locked knee, MRI was obtained with the patient’s knee was at 90° of flexion. The MRI confirmed the presence of a bucket-handle lateral meniscus tear, which was displaced into the anterior aspect of the joint, resulting in the inability to fully extend the knee. It was noted that the distance from the lateral meniscus posterior capsule to the popliteal artery was 15.1 mm with the knee in 90° of flexion (Fig. 1). Given the presence of a PHLM tear, the patient was indicated for arthroscopic repair.

During a diagnostic arthroscopy of the lateral compartment of the knee, the lateral meniscus was noted to be torn at the meniscocapsular junction from the anterior horn/body junction to the intact posterior root. Meniscus repair was performed in the figure-of-four position using 4 inside-out sutures and 2 all-inside suture implants. The patient was slow to gain early postoperative range of motion due to apprehension about the knee, however, 3 months postoperatively, the range of motion was 0–90° without any mechanical catching or locking. An MRI with the knee standardly positioned in relative extension was obtained to ensure healing of the meniscus prior to progression to impact resistance training. This MRI demonstrated that the distance from the lateral meniscus posterior capsule to the popliteal artery was 5.8 mm (Fig. 1). Over the following 3 months, the patient steadily improved his range of motion with the assistance of a static progressive flexion splint, and regained strength symmetry, so that he was cleared for return to sports 8 months postoperatively. Knee range of motion was 0–130°, compared to 0–140° on the contralateral side. At the final follow-up 13 months postoperatively, the knee range of motion was 0–140° bilaterally. The patient reported a PROMIS pain interference score improvement from 77 at baseline to 38.7 13 months postoperatively and a PROMIS physical activity score improvement from 49 at baseline to 53.7 13 months postoperatively. The patient also reported normal or high levels of activity and function 13 months postoperatively (Table 1).

It is important for orthopedic surgeons to understand the risk of iatrogenic injury to NV structures during meniscus repair. While all-inside meniscus repair is highly effective and complications are rare, suturing devices are often made with a minimum firing distance, which may still result in injury to the popliteal NV bundle immediately posterior to the lateral meniscus. Therefore, it is critical to ensure that the set penetration distance of the meniscal repair device is sufficiently less than the distance from the lateral meniscus posterior capsule to these NV structures. This is particularly important in pediatric patients for whom these devices were not originally designed. While studies have quantified the distance between the posterior capsule and the NV bundle on MRI, this is the first study to report this distance with the knee in flexion in a living patient in order to more closely replicate the position of the knee at the time of an arthroscopic lateral meniscal repair. The results of this study suggest that the distance between the lateral meniscus posterior capsule and the NV bundle increases with knee flexion (5.8 mm and 15.1 mm in knee extension and flexion, respectively), which is consistent with results from cadaveric studies. For example, when a suturing device was inserted at the lateral edge of the popliteal hiatus in one cadaveric study, the distance between the device and the popliteal nerve decreased from a median of 21.5 mm in 90° of knee flexion to 15.5 mm in 0° of flexion [9]. While the authors used different landmarks for measurement than those of the current study, their results demonstrate that the distance between meniscal structures and popliteal NV structures increases with increasing knee flexion. Ninety degrees of knee flexion is similar to the figure-of-four positioning during lateral meniscus repair. Therefore, studies that measure this distance in full extension may be overestimating the risk to the NV bundle during lateral meniscus repair. For example, one MRI study found that the mean distance between the PHLM and the popliteal NV bundle in adults with the knee in extension was 7.8 mm [4]. Future studies with larger sample sizes that assess the distance between the lateral meniscus posterior capsule and NV bundle with the knee in flexion are therefore warranted to elucidate the true safe distance during surgery. One important limitation of this study should be noted. With a displaced bucket handle lateral meniscus tear, it was impossible to accurately measure the penetration distance of a meniscal implant through the meniscus, posterior capsule, and to the NV bundle. Instead, measuring the distance from the lateral meniscus posterior capsule to the NV bundle allowed for accurate measurement and direct comparison of an identical measurement technique both preoperatively and postoperatively. Furthermore, measuring from the capsule to the NV bundle would, if anything, underestimate the true distance of a meniscal implant needle (safer than overestimation) and not affect the change in distance measured from flexion to extension. Finally, this case report does not account for anatomic variability among pediatric patients.
While the results of the current study suggest that the risk of injury to the NV bundle may be lower than previously described in the literature, it is still important to err on the side of caution and assess the risk of iatrogenic injury on a case-by-case basis.
The distance from the popliteal NV bundle to the posterior to the lateral meniscus is typically measured on MRI with the knee in relative extension, which is the standard position for obtaining MRI. However, during lateral meniscus repair, the knee is routinely placed in a 90° flexed position in “figure-of-four”. This unique case, in which the patient presented with his knee locked in 90° of flexion, required MRI be obtained at a flexion angle comparable to intraoperative positioning during repair. This, therefore, allowed for a more applicable measurement of the distance between the posterior capsule and the NV bundle. We found that the distance between the popliteal NV bundle and lateral meniscus posterior capsule was greater with the knee in flexion than in extension, suggesting that risk of iatrogenic injury to the NV bundle during lateral meniscus repair may be lower than previously reported.
References
- 1.Kramer DE, Micheli LJ. Meniscal tears and discoid meniscus in children: Diagnosis and treatment. J Am Acad Orthop Surg 2009;17:698-707. [Google Scholar | PubMed]
- 2.Werner BC, Yang S, Looney AM, Gwathmey FW Jr. Trends in pediatric and adolescent anterior cruciate ligament injury and reconstruction. J Pediatr Orthop 2016;36:447-52. [Google Scholar | PubMed]
- 3.Massey P, Parker D, Feibel B, Ogden A, Robinson J, Barton RS. Proximity of the neurovascular bundle during posterior-lateral meniscal repair: A comparison of the transpatellar, anteromedial, and anterolateral portals. Arthroscopy 2019;35:1557-64. [Google Scholar | PubMed]
- 4.Gilat R, Agar G, Shohat N, Dahan M, Beer Y, Lindner D. Avoiding injury to the popliteal neurovascular bundle in all-inside suturing of the posterior horn of the lateral meniscus: A magnetic resonance imaging assessment of portal selection and safety. Arthroscopy 2020;36:492-8. [Google Scholar | PubMed]
- 5.Chuaychoosakoon C, Wuttimanop W, Tangjatsakow P, Charoenrattanawat S, Parinyakhup W, Boonriong T, et al. The danger zone for iatrogenic neurovascular injury in all-inside lateral meniscal repair in relation to the popliteal tendon: An MRI study. Orthop J Sports Med 2021;9:23259671211038396. [Google Scholar | PubMed]
- 6.Gupta H, Ghasi RG, Kataria H, Jain V, Shankar V, Daripa RK, et al. Popliteal neurovascular bundle is safe during inside-out repair of medial meniscus without a safety incision. Knee Surg Sports Traumatol Arthrosc 2019;27:153-65. [Google Scholar | PubMed]
- 7.Oehler N, Foerg A, Haenle M, Blanke F, Vogt S. Assessment of popliteal neurovascular safety during all-inside suturing of the posterior horn of the lateral meniscus using upright MRIs of the knee joint. Knee 2021;33:234-42. [Google Scholar | PubMed]
- 8.Schachne JM, Heath MR, Yen YM, Shea KG, Green DW, Fabricant PD. The safe distance to the popliteal neurovascular bundle in pediatric knee arthroscopic surgery: An age-based magnetic resonance imaging anatomic study. Orthop J Sports Med 2019;7:2325967119855027. [Google Scholar | PubMed]
- 9.Cuéllar A, Cuéllar R, Cuéllar A, Garcia-Alonso I, Ruiz-Ibán MA. The effect of knee flexion angle on the neurovascular safety of all-inside lateral meniscus repair: A cadaveric study. Arthroscopy 2015;31:2138-44. [Google Scholar | PubMed]
- 10.Yen YM, Fabricant PD, Richmond CG, Dingel AB, Milewski MD, Ellis HB, et al. Proximity of the neurovascular structures during all-inside lateral meniscal repair in children: A cadaveric study. J Exp Orthop 2018;5:50. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Short-term Clinical and Radiologic Outcomes, and Survivorship Following Primary Total Knee Arthroplasty Using a Novel High-Flexion System among Indian Patients
June 1, 2026 Short-term Clinical and Radiologic Outcomes, and Survivorship Following Primary Total Knee Arthroplasty Using a Novel High-Flexion System among Indian Patients June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report October 10, 2020 Non-operative Management of an Adult Both Bone Forearm Fractures – A Case Report and Literature Review
October 10, 2020 Non-operative Management of an Adult Both Bone Forearm Fractures – A Case Report and Literature Review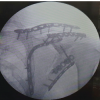 July 1, 2026 Varied Reduction and Fixation Modalities for Scapula Fractures: A Case Series
July 1, 2026 Varied Reduction and Fixation Modalities for Scapula Fractures: A Case Series