
Total knee arthroplasty using the Zenith® high-flexion system results in satisfactory post-operative knee range of movement, significant improvements in clinical outcome scores, and good prosthetic survivorship among Indian patients.
Dr. Umesh Nagare, Department of Orthopaedics, Vishwaraj Hospital, Near Loni Railway Station, Loni Kalbhor, Solapur-Pune Highway, Pune-412201, Maharashtra, India. E-mail: umeshnagare@yahoo.com
Abstract
Introduction: High-flexion total knee arthroplasty (TKA) prostheses permit deep knee flexion, which is important for day-to-day activities, especially among Indian patients. However, some high-flexion designs have been reported to be associated with early aseptic loosening and valgus instability in the past. Close monitoring of patients undergoing TKA using newer high-flexion prosthetic designs is imperative. The purpose of this study was to evaluate the short-term clinical outcomes and prosthetic survivorship of Indian patients following TKA using the Zenith® high-flexion system.
Materials and Methods: Overall, 101 patients who underwent TKA using the Zenith® high-flexion system for osteoarthritis of the knee between June 2022 and August 2023 across four tertiary care hospitals were studied. Their pre-operative and post-operative knee range of movement and clinical evaluation scores were assessed. In addition, short-term prosthetic survivorship was assessed. Adverse events, if any, were recorded.
Results: The study cohort included 51 men and 50 women with a mean age of 62.37 ± 6.96 years. Cruciate-retaining and posterior-stabilised prostheses were used in 58 and 43 patients, respectively. All patients were followed up for a minimum of 2 years postoperatively. Post-traumatic valgus instability necessitating revision TKA occurred in one patient; data pertaining to this patient were used for survivorship analysis, but not for evaluation of clinical outcome scores. Mild anterior notching occurred in one patient. No other adverse events were recorded. Knee flexion improved significantly from 97.82° ± 12.11° preoperatively to 114.11° ± 7.26° postoperatively (P < 0.001). Significant improvements in the Knee Society Knee Score (40.81 ± 15.18 preoperatively to 88.58 ± 8.41 postoperatively) (P < 0.001) and Knee Society Functional Score (59.56 ± 16.43 preoperatively to 95.69 ± 6.60 postoperatively) (P < 0.001) were noted. The mean Forgotten Joint Score at 2 years’ follow-up was 87.64 ± 15.57. When revision for all causes was considered, the 2-year prosthetic survivorship as evaluated using a Kaplan-Meier plot was 99%.
Conclusion: The Zenith® high-flexion system is associated with satisfactory short-term clinical outcomes and prosthetic survivorship. Further research is required to evaluate its performance in the mid- and long-term.
Keywords: Total knee arthroplasty, knee replacement, high flexion, Zenith, knee flexion, Indian patients.
Total knee arthroplasty (TKA) is one of the commonest surgical procedures performed in day-to-day orthopaedic practice. It aims to alleviate pain and improve knee function and quality of life among patients with end-stage knee arthritis through the restoration of lower limb alignment and attainment of medio-lateral gap balance and joint stability throughout physiologic knee range of movement [1]. Unlike total hip arthroplasty, which has been hailed as the “operation of the century” [2], however, nearly one-fifth of the patients remain dissatisfied with the outcomes of TKA [3], while one-third report that their prosthetic knee does not feel “normal” [4]. Despite advances in prosthetic design, precision of instrumentation, and surgical technology, the ability to perform high-flexion activity and restoration of activities of daily living rank among the top three improvements desired by patients in TKA outcomes [5]. The ability to perform deep knee flexion is known to positively influence patient-reported outcome measures following TKA but is not universally or uniformly restored postoperatively [6]. It is especially critical for Asian patients – for whom squatting, kneeling, and sitting cross-legged are part of their daily activities – and is shown to promote greater satisfaction with their postoperative outcomes and improved quality of life [7,8]. Knee range of movement following TKA is influenced by several factors, including pre-operative range of movement, joint line position, tibial component rotation, body mass index (BMI), and post-operative patellofemoral pain [9,10,11]. The design of TKA prostheses used presents an additional modifiable variable influencing the post-operative knee range of movement, with modern “high-flexion” designs offering superior flexion with comparable clinical outcomes and prosthetic survivorship vis-à-vis conventional designs [12,13]. Scant literature is available regarding the overall outcomes and survivorship of high-flexion TKA prostheses in the context of Indian patients, although initial reports seem promising [14,15]. We hypothesised that TKA using a high-flexion prosthetic design would result in satisfactory post-operative knee range of movement, improvements in clinical outcome measures, and acceptable prosthetic survivorship among Indian patients with advanced osteoarthritis of the knee. The purpose of this research was to assess the short-term post-operative clinical and radiologic outcomes and overall survivorship of the Zenith® high-flexion primary knee system (Plus Orthopaedics, Chennai, Tamil Nadu, India) at 2 years following primary TKA. To our knowledge, short- and/or mid-term results of this system in the Indian population have not been reported previously.
Study design, patient selection, and pre-operative evaluation:
Following ethical approval, a retrospective observational study was conducted across four tertiary care hospitals. The respective TKA databases of these institutes were reviewed. Consecutive patients who had undergone conventional manual TKA for end-stage primary osteoarthritis of the knee using the Zenith® high-flexion primary knee system (Figs. 1 and 2) between June 2022 and August 2023 were included.
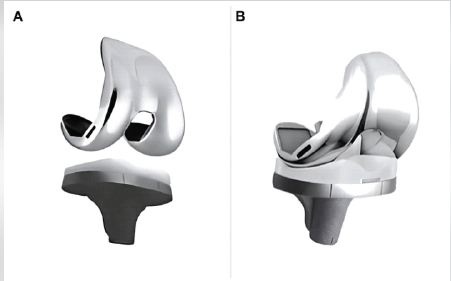
Figure 1: The Zenith® high-flexion total knee arthroplasty prosthetic designs. (a) Cruciate-retaining design. (b) Posterior-stabilized design.
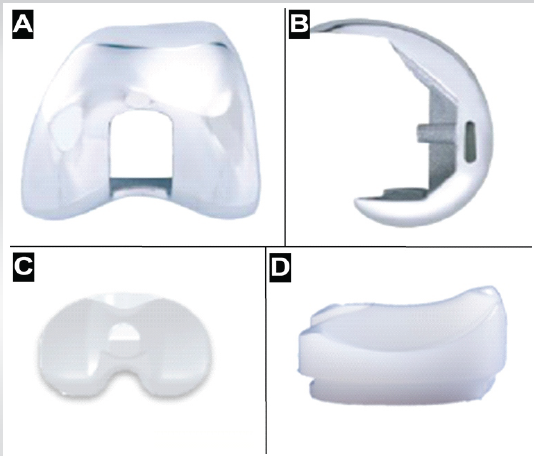
Figure 2: Design details of the Zenith® high-flexion total knee arthroplasty prostheses. (a) A posterior-stabilized femoral component (frontal view) showing an anatomic anterior arc and a deep trochlear groove. (b) Posterior stabilized femoral component (lateral view) showing a thicker posterior condylar portion and a thinner anterior condylar portion. (c) A posterior stabilized tibial insert (superior view) showing a deep anterior notch and a posteriorized peg. (d) A cruciate retaining tibial insert (lateral view) showing an anterior notch.
Patients with inflammatory arthritis, ankylosis, secondary osteoarthritis, bony dysplasia, hepatic or renal failure, or a prior history of lower limb surgery were excluded. Informed consent was obtained from all identified patients before recruiting them for this research. All included patients were followed up for a minimum of 2 years postoperatively. Their demographic details, including age, sex, and BMI, were retrieved. As per the institutional protocols, routine pre-operative evaluation of patients planned for TKA included assessment of the flexion deformity and range of flexion of the knee, evaluation of the mechanical hip-knee-ankle angle on weight-bearing anteroposterior long-leg radiographs as a means of quantifying the existing coronal deformity, and estimation of the Knee Society Knee and Functional Scores (KSKS and KSFS, respectively); these details were also retrieved from the respective institutional patient chart records.
Surgical technique, intraoperative data:
All included patients underwent TKA under spinal anaesthesia, using a similar technique. Joint exposure was obtained following an anterior midline incision and medial parapatellar arthrotomy. Osteophytes, menisci, and the anterior cruciate ligament were excised. One of the surgeons routinely released the posterior cruciate ligament (PCL) and used posterior-stabilised (PS) prostheses. The other three preserved the PCL and used cruciate-retaining (CR) prostheses wherever feasible, while sacrificing it only when deemed necessary for optimal gap balancing. Bony resection based on the adjusted mechanical alignment strategy was carried out in all cases, while targeting overall coronal alignment within 3° from the neutral mechanical axis. Soft-tissue releases to attain balanced medio-lateral gaps in flexion and extension were performed as necessary. A tibial stem extension was used where indicated. Water-tight closure of the arthrotomy incision and wound closure in layers was then performed. Intraoperative complications, if any, including anterior femoral notching and patellar maltracking, were documented. All relevant intraoperative details were retrieved from the patients’ operation notes.
Post-operative care and follow-up:
A similar protocol for post-operative care, rehabilitation, and follow-up was implemented at all the centres where the study was conducted. All patients were mobilised and encouraged to ambulate with weight-bearing as tolerated while using a walker from the 1st postoperative day onwards. Skin sutures were removed 2 weeks postoperatively. Ambulatory aids were gradually discontinued around 3 months following surgery. Patients were subsequently followed up at 6 months, 1 year, and 2 years postoperatively as per routine protocols. At each follow-up visit, knee range of movement was assessed, and knee radiographs were obtained to assess component positioning and fixation. Lower limb alignment was evaluated on these radiographs using a described technique [16]. At annual visits, clinical outcome scores including the KSKS, KSFS, and Forgotten Joint Score (FJS) were recorded. Complications, if any, including the need for reoperation or revision, were documented and appropriately managed. Retrospective data relevant to the present study were recovered from the patients’ respective outpatient records. The clinical and radiologic assessments at 2-year follow-up visits were recorded for all patients.
Sample size assessment, data analysis:
Reliable assessment of post-operative knee range of movement was central to evaluating the clinical outcomes of patients included in this research. Londhe et al. [14], in a study focusing on the outcomes of high-flexion PS TKA using another implant system among Indian patients, noted that the mean ± standard deviation (SD) post-operative knee range of motion at a minimum follow-up of 5 years was 127.69° ± 3.65°. Given that improvements in knee extension and flexion tend to plateau around 6 months and 3 months following TKA, respectively [17], based on the findings of Londhe et al. [14], to estimate the mean post-operative knee range of movement in a subsequent cohort of Indian patients undergoing TKA with high-flexion prostheses with a 5°-wide 95% confidence interval, a minimum sample size of nine patients was adequate. However, given the possibility of greater variance in our study cohort and for improved characterisation of all studied post-operative outcomes, a larger sample size of 100 was considered more appropriate for this study. Proportions and means with SDs were assessed for categorical and numerical variables, respectively. Normality of distribution was assessed using the Shapiro-Wilk test. Datasets of related numerical variables were compared using the paired T-test (where parametric distribution was noted) or the Wilcoxon signed-rank test (where non-parametric distribution was noted). Overall prosthetic survivorship was assessed through Kaplan-Meier survival plots. Statistical significance was set at 0.05. All statistical analysis was performed using Statistical Package for the Social Sciences Statistics for Windows, version 25 (IBM, USA). Linear associations between numerical variables were assessed using Pearson’s correlation coefficient.
Among 103 consecutive patients who fulfilled the inclusion criteria during the study period, two were lost to follow-up; this left 101 patients with a minimum follow-up of 2 years for an analysis of the post-operative outcomes and prosthetic survivorship. This cohort included 51 (50.5%) men and 50 (49.5%) women with a mean age of 62.37 ± 6.96 (range: 45–78) years and a mean BMI of 27.62 ± 4.21 (range: 16.66–39.56). In all, 58 (57.43%) patients received CR prostheses, while 43 (42.57%) received PS prostheses. None of the patients showed patellar maltracking. Mild anterior femoral notching occurred intraoperatively in one patient; this, however, did not affect her subsequent outcomes. Valgus instability was noted in a 74-year-old woman following a fall 4 months postoperatively, necessitating revision TKA with a modular semi-constrained rotating hinge system; data pertaining to her case were included for survivorship analysis but excluded from outcome analysis. No other complications occurred in the study population. The lower limb mechanical alignment significantly improved from a mean pre-operative value of 5.49° ± 8.49° (range: 20° varus to 15° valgus) to a mean post-operative value of 1.57° ± 1.24° (range: 2° varus to 3° valgus) (P < 0.001). In addition, significant post-operative improvements were noted in the patients’ knee range of movement and clinical scores (Table 1, Figs. 3 and 4).
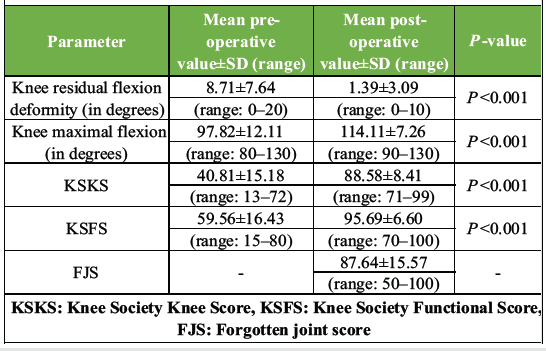
Table 1: A summary of the pre-operative and post-operative clinical evaluation parameters of the study cohort
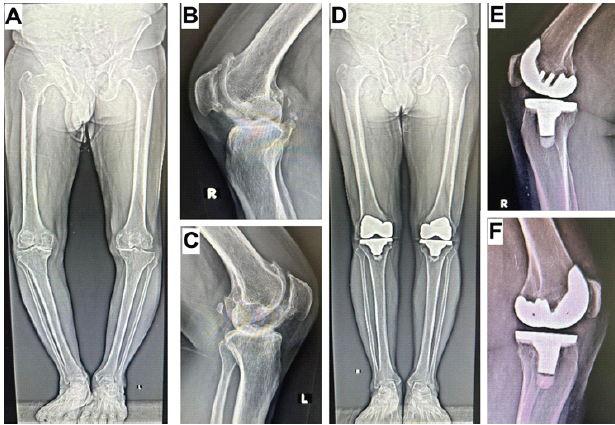
Figure 3: Pre-operative and post-operative radiographs of a patient with bilateral knee osteoarthritis who underwent bilateral total knee arthroplasty using Zenith® high-flexion prostheses. (a) Pre-operative weight-bearing anteroposterior long leg radiograph. (b) Pre-operative lateral radiograph of the right knee. (c) Pre-operative lateral radiograph of the left knee. (d) Post-operative weight-bearing anteroposterior long leg radiograph at 2 years follow-up. (e) Post-operative lateral radiograph of the right knee. (f) Post-operative lateral radiograph of the left knee.
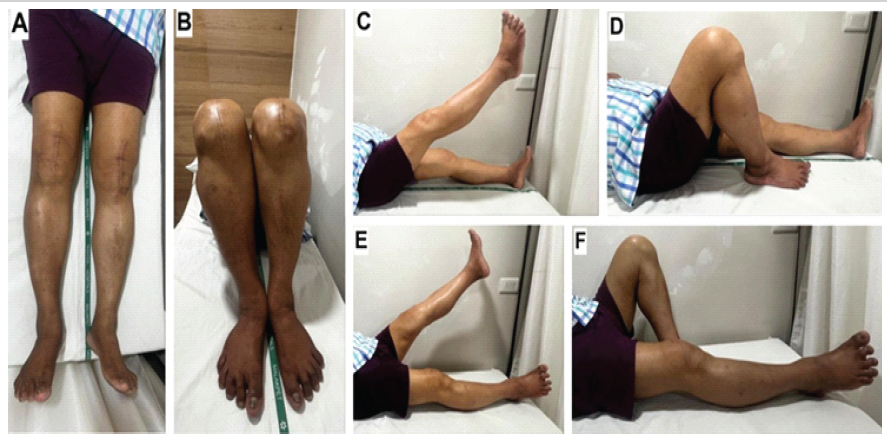
Figure 4: Clinical image of a patient showing full post-operative knee range of movement following bilateral total knee arthroplasty. (a) Patient is lying supine with both knees comfortably in full extension. (b) Foot end view of patient with both knees held in maximal flexion. (c) Right knee extension and straight leg raising. (d) Right knee deep flexion. (e) Left knee extension and straight leg raising. (f) Left knee deep flexion.
The achieved post-operative range of knee flexion did not demonstrate a significant correlation with the KSKS (R = −0.10, P = 0.318) and FJS (R = 0.12, P = 0.231). It, however, showed a weak but significant positive correlation with the KSFS (R = 0.248, P = 0.012). BMI did not show any correlation with residual post-operative flexion deformity (Pearson’s r = 0.075, P = 0.485), post-operative range of flexion (Pearson’s r = 0.003, P = 0.980), KSKS (Pearson’s r = 0.092, P = 0.396), KSFS (Pearson’s r = −0.064, P = 0.555) or FJS (Pearson’s r = −0.154, P = 0.153) at the last follow-up. Post-operative outcomes were comparable between men and women in terms of knee range of movement, KSKS, and KSFS; however, men showed significantly greater FJS postoperatively (Table 2).
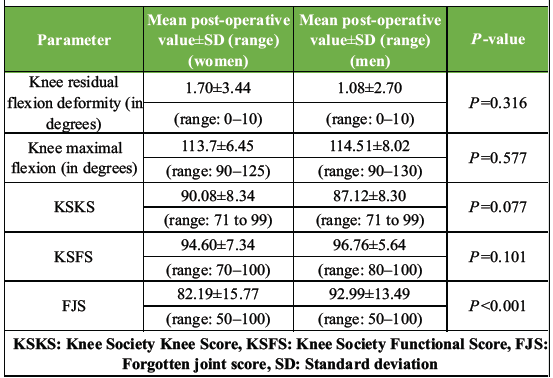
Table 2: A comparison of post-operative outcomes between men and women
Prosthetic survivorship at 2 years postoperatively was 100% when aseptic loosening was considered as the endpoint. When revision for all causes was considered, the 2-year survivorship as assessed using a Kaplan-Meier survival plot was estimated to be 99% (Fig. 5). No evidence suggestive of periprosthetic infection or aseptic component loosening was noted in any of the studied patients.
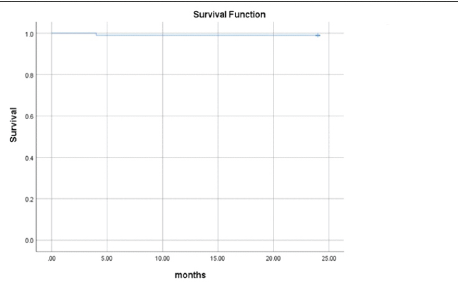
Figure 5: Prosthetic survivorship analysis using the Kaplan-Meier plot, with revision for all causes as the endpoint.
High-flexion prosthetic designs represent an evolutionary modification of conventional TKA prostheses; they are not a different class of implants. They were developed through subtle yet purposeful changes in component geometry that facilitate deep knee flexion. Likewise, the Zenith® high-flexion system of TKA prostheses used in this study differs from regular TKA prostheses in certain aspects. The single-radius femoral component demonstrates thicker and rounder posterior condyles to permit greater femoral rollback with better contact while delaying impingement against the insert. Its anterior condyle, however, is thinner, to prevent overstuffing of the patellofemoral joint and subsequent anterior knee pain. Likewise, it also has an anterior anatomic arc design to reduce pressure over the surrounding soft tissues and has a deeper trochlea with a lengthier recess to prevent patellar tendinitis. The cam-post mechanism in the PS system is designed for delayed engagement through posteriorisation of the post by 2 mm; this not only permits deep knee flexion but also reduces the impact force acting on the post, thereby reducing the risk of wear or breakage. The “aquiline nose shape” of the post reduces the risk of cam-post dislocation in deep flexion. The polyethylene insert has an anterior notch to reduce irritation of the patellar tendon during deep flexion. Finally, it can accommodate tibial stem extensions and augments for additional stability and defect reconstruction, respectively. Although these design variations have shown initial promise, certain concerns regarding the possibility of aseptic femoral component loosening and iatrogenic valgus instability due to increased bone resection have been raised in the past, necessitating research on clinical outcomes and survivorship following TKA with high-flexion systems. The principal finding of our study was that TKA using the Zenith® high-flexion primary knee system resulted in satisfactory short-term clinical outcomes among Indian patients, with considerable and significant improvements in the KSKS and KSFS and acceptable post-operative FJS values. These results are consistent with previously reported outcomes of high-flexion TKA using other prosthetic systems in varied populations. Kim et al. [18] reported significant long-term improvements in the Knee Society Score and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) following high-flexion TKA using the LOSPA knee system (Corentec Inc., Seoul, Korea). Lee et al. [19] and Jeon et al. [20] noted significantly improved mid- to long-term WOMAC and Knee Injury and Osteoarthritis Outcome Score values after high-flexion TKA with the Vega knee system (BBraun, Aesculap, Tuttlingen, Germany) and the NexGen LPS-flex system (Zimmer, Warsaw, USA), respectively. Likewise, long-term improvements in the KSKS and KSFS following TKA were reported by Baek et al. [21] and Crawford et al. [22] while using the Scorpio Non-Restrictive Geometry (Stryker Orthopaedics, Mahwah, USA) and Vanguard Complete Knee (Zimmer Biomet, Warsaw, USA) high-flexion knee systems. Similar mid-term outcomes were also noted with the PFC Sigma rotating-platform high-flexion (DePuy Synthes, Warsaw, USA) TKA system by Jain et al. [23]. A statistically significant and clinically relevant increase in the range of knee flexion was noted in our study population, with the mean post-operative flexion exceeding the minimum value of 110° considered essential to permit squatting [9]. This is consistent with the findings from prior studies on high-flexion TKA [18,19,20,21,22,23]. Interestingly, however, the extent of knee flexion achieved did not show any association with the KSKS and FJS and only showed a weak positive correlation with the KSFS. Ha et al. [24], in their research on the usefulness of current outcome measurement tools for evaluating the knee status during deep flexion, concluded that the KSKS, KSFS, and WOMAC were incapable of detecting small functional differences during deep knee flexion. Although they did subsequently report statistically significant correlations between knee range of movement and the KSKS, KSFS, and WOMAC, these associations were weak to moderate at best [8]. Our results corroborate their observations and reiterate the limitations of conventional clinical outcome measurement tools in assessing knee stability and function during activities involving deep flexion. We believe that this needs to be borne in mind when standard and high-flexion TKA prostheses are compared in future research, given the lack of universal advocacy for the latter in view of the general perception of “non-superior clinical outcomes and survivorship” despite a widespread acknowledgement of the superior knee range of movement afforded. Excellent short-term prosthetic survivorship, consistent with the reported overall mid- to long-term survivorship of high-flexion TKA in the literature [18,19,21,22,25], was noted in our study cohort. Despite the short duration of follow-up and an undeniable need for evaluating long-term survivorship of the studied system, our results are relevant for two reasons. First, the very permissibility of passive-maximal knee bending has been questioned in the past in view of concerns regarding the possibility of early aseptic loosening of the femoral component resulting from the lack of load-sharing between the prosthesis and condylar bone in deep flexion, as demonstrated during in vitro analysis [26]. This concern was also substantiated in some studies on certain earlier high-flexion prosthetic designs [27,28]. Despite subsequent research on more recent high-flexion prosthetic designs demonstrating excellent long-term survivorship, closely monitoring the longevity associated with all newer iterations is imperative. Second, given the smaller bone size and gross deformities at presentation among Indian patients and the need to resect more bone from the posterior femoral condyles when using high flexion as against conventional TKA systems, the theoretical risk of iatrogenic injuries and/or progressive detachment of the medial collateral ligament around the femoral origin exists [23]. Since all high-flexion prostheses are not designed similarly, monitoring for failure due to iatrogenic valgus instability is essential. Despite concerns regarding the possibility of certain complications arising from the design changes offered by high-flexion prosthetic systems, we believe that these are preventable through careful attention to proper surgical technique and that satisfactory outcomes can be achieved, as shown in our research. Several intraoperative strategies play a role in optimising postoperative outcomes following TKA with high-flexion systems. Attaining appropriate alignment and medio-lateral flexion gap balance is critical in this regard. This is achieved through proper bony resection, restoration of posterior femoral condylar offset, and the use of adjustments in posterior tibial slope or femoral component rotation within safe boundaries to adjust flexion gap imbalance. Adequate surgical exposure is essential, as it not only permits accurate gap assessment but also timely excision of osteophytes, loose bodies, and residual bone cement that might result in tightness or impingement. Appropriate component sizing to prevent overhang and joint overstuffing is also important to facilitate smooth impingement-free knee range of motion. We believe that careful attention to intraoperative joint exposure, bony resection, gap balance, posterior condylar offset restoration, component size, and excision of osteophytes, loose bodies, or excessive bone cement can prevent post-operative complications to a large extent. Our research has certain limitations and strengths. The retrospective single-arm observational study design may have introduced a certain degree of selection bias, but it was considered essential before undertaking prospective randomised trials. The inclusion of cases operated on by different surgical teams introduced a degree of variance in terms of surgical technique but also ensured adequate participant recruitment and enhanced the generalisability of the results. Prosthetic survivorship and outcomes were only assessed during short-term follow-up; this, however, was inevitable given the short interval of time between the introduction of the studied system and the commencement of this study. Subgroup analysis of CR and PS designs was not attempted as PCL sacrifice was not optional and based on surgeons’ personal preferences in most cases but rather consequent to its inevitability in knees where the medial and lateral gaps could not be balanced in extension and flexion intraoperatively by preliminary soft-tissue releases alone. Multivariate regression analysis of factors that could potentially influence post-operative knee range of movement was not carried out, as it was beyond the scope of the present research. Conventional outcome measures were used for evaluating clinical outcomes despite their purported limitations. This, however, was intentional, given the inherent need to compare the results of the studied high-flexion system with those of others reported in the literature and the futility of developing and validating a novel assessment tool capable of identifying knee functionality in deep flexion in a single-arm study.
The preliminary results of the Zenith® high-flexion primary knee system appear promising, with considerable improvements in knee range of movement, satisfactory clinical and radiologic outcomes, and excellent prosthetic survivorship. This system was primarily designed with Indian patients and their requirements in mind. Given that Asians, particularly Indians, require deep knee flexion during their daily activities, it presents a safe and effective alternative to conventional as well as high-flexion TKA prostheses. Future studies are required to compare the performance of this system against that of standard TKA systems and to evaluate its longevity and long-term outcomes.
High-flexion TKA prostheses permit deep knee flexion, which is important for Indian patients in their daily activities; however, certain prosthetic designs have been reported to be associated with early aseptic loosening and valgus instability in the past. Careful monitoring of patients undergoing TKA using novel iterations of these designs for clinical outcomes and potential adverse outcomes is imperative. The short-term outcomes and survivorship of the Zenith® high-flexion system appear to be satisfactory in the present study.
References
- 1. Eachempati KK, Parameswaran A, Dannana CS. Sliding condylar osteotomy for managing severe deformities in total knee arthroplasty. In: Sharma M, editor. Knee Arthroplasty New and Future Directions. 1st ed. Singapore: Springer; 2022. p. 227-48. [Google Scholar] [PubMed]
- 2. Learmonth ID, Young C, Rorabeck C. The operation of the century: Total hip replacement. Lancet 2007;370:1508-19. [Google Scholar] [PubMed]
- 3. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not? Clin Orthop Relat Res 2010;468:57-63. [Google Scholar] [PubMed]
- 4. Nam D, Nunley RM, Barrack RL. Patient dissatisfaction following total knee replacement: A growing concern? Bone Joint J 2014;96-B:96-100. [Google Scholar] [PubMed]
- 5. Kim SJ, Bamne A, Song YD, Kang YG, Kim TK. Patients still wish for key improvements after total knee arthroplasty. Knee Surg Relat Res 2015;27:24-33. [Google Scholar] [PubMed]
- 6. Scott CE, Holland G, Gillespie M, Keenan OJ, Gherman A, MacDonald DJ, et al. The ability to kneel before and after total knee arthroplasty: The role of the pattern of osteoarthritis and the position of the femoral component. Bone Joint J 2021;103-B:1514-25. [Google Scholar] [PubMed]
- 7. Han HS, Kim JS, Lee B, Won S, Lee MC. A high degree of knee flexion after TKA promotes the ability to perform high-flexion activities and patient satisfaction in Asian population. BMC Musculoskelet Disord 2021;22:565. [Google Scholar] [PubMed]
- 8. Ha CW, Park YB, Song YS, Kim JH, Park YG. Increased range of motion is important for functional outcome and satisfaction after total knee arthroplasty in Asian patients. J Arthroplasty 2016;31:1199-203. [Google Scholar] [PubMed]
- 9. Li T, Sun J, Du Y, Gao Z, Ma H, Zhou Y. Factors affecting squatting ability in total knee arthroplasty using high flexion prosthesis. Ther Clin Risk Manag 2021;17:1249-56. [Google Scholar] [PubMed]
- 10. Fuchs MC, Janssen RP. Clinical evaluation of 292 Genesis II posterior stabilized high-flexion total knee arthroplasty: Range of motion and predictors. Eur J Orthop Surg Traumatol 2015;25:161-6. [Google Scholar] [PubMed]
- 11. Niki Y, Takeda Y, Harato K, Suda Y. Factors affecting the achievement of Japanese-style deep knee flexion after total knee arthroplasty using posterior-stabilized prosthesis with high-flex knee design. J Orthop Sci 2015;20:1012-8. [Google Scholar] [PubMed]
- 12. Wang Z, Wei M, Zhang Q, Zhang Z, Cui Y. Comparison of high-flexion and conventional implants in total knee arthroplasty: A meta-analysis. Med Sci Monit 2015;21:1679-86. [Google Scholar] [PubMed]
- 13. Jain S, Pathak AC, Kanniyan K, Kulkarni S, Tawar S, Mane P. High-flexion posterior-stabilized total knee prosthesis: Is it worth the hype? Knee Surg Relat Res 2013;25:100-5. [Google Scholar] [PubMed]
- 14. Londhe SB, Shah RV, Khot R, Desouza C. Early results of bone-conserving high flexion posterior-stabilized total knee system in Indian population. Indian J Orthop 2022;56:1759-66. [Google Scholar] [PubMed]
- 15. Singh H, Mittal V, Nadkarni B, Agarwal S, Gulati D. Gender-specific high-flexion knee prosthesis in Indian women: A prospective randomised study. J Orthop Surg (Hong Kong) 2012;20:153-6. [Google Scholar] [PubMed]
- 16. Perka N, Kopf S, Hommel H. A whole leg radiograph is not necessary for postoperative determination of the mechanical leg axis after total knee arthroplasty. Arch Orthop Trauma Surg 2019;139:1455-60. [Google Scholar] [PubMed]
- 17. Mutsuzaki H, Takeuchi R, Mataki Y, Wadano Y. Target range of motion for rehabilitation after total knee arthroplasty. J Rural Med 2017;12:33-7. [Google Scholar] [PubMed]
- 18. Kim MS, Choi KY, Hur JH, In Y. A high-flexion design total knee prosthesis: A ten to twelve-year follow-up study. J Orthop Surg Res 2024;19:599. [Google Scholar] [PubMed]
- 19. Lee CR, Park DH, Heo KS, Jo SM, Seo KJ, Seo SS. Long-term outcomes of high-flexion design total knee arthroplasty with a short posterior flange. Clin Orthop Surg 2024;16:251-8. [Google Scholar] [PubMed]
- 20. Jeon YS, Shin JS, Jung JH, Kim MK. Total knee arthroplasty using NexGen LPS-flex® improves clinical outcomes without early loosening: Minimum 6-year follow-up results. J Orthop Surg Res 2016;11:83. [Google Scholar] [PubMed]
- 21. Baek JH, Lee SC, Choi K, Ahn HS, Nam CH. Long-term survivorship of total knee arthroplasty with a single-radius, high-flexion posterior stabilized prosthesis. Knee 2021;30:275-82. [Google Scholar] [PubMed]
- 22. Crawford DA, Adams JB, Hurst JM, Berend KR, Lombardi AV Jr. Ten-year minimum outcomes and survivorship with a high flexion knee system. J Arthroplasty 2019;34:1975-9. [Google Scholar] [PubMed]
- 23. Jain S, Pathak AC, Kalaivanan K. Minimum 5-year follow-up results and functional outcome of rotating-platform high-flexion total knee arthroplasty: A prospective study of 701 knees. Arthroplast Today 2016;2:127-32. [Google Scholar] [PubMed]
- 24. Ha CW, Park YB, Song YS, Lee WY, Park YG. Are the current outcome measurement tools appropriate for the evaluation of the knee status in deep flexion range? J Arthroplasty 2016;31:87-91. [Google Scholar] [PubMed]
- 25. Rhee SJ, Hong SM, Suh JT. High-flexion total knee arthroplasty using nexgen LPS-flex system: Minimum 5-year follow-up results. Knee Surg Relat Res 2015;27:156-62. [Google Scholar] [PubMed]
- 26. Bollars P, Luyckx JP, Innocenti B, Labey L, Victor J, Bellemans J. Femoral component loosening in high-flexion total knee replacement: An in vitro comparison of high-flexion versus conventional designs. J Bone Joint Surg Br 2011;93:1355-61. [Google Scholar] [PubMed]
- 27. Han HS, Kang SB, Yoon KS. High incidence of loosening of the femoral component in legacy posterior stabilised-flex total knee replacement. J Bone Joint Surg Br 2007;89:1457-61. [Google Scholar] [PubMed]
- 28. Cho SD, Youm YS, Park KB. Three- to six-year follow-up results after high-flexion total knee arthroplasty: Can we allow passive deep knee bending? Knee Surg Sports Traumatol Arthrosc 2011;19:899-903. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report
July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report