
Scapula fractures are operated less often and there exists lack of references for fixation
Dr Shivam Sharma, H. No. 40, Sector 8A, Gandhinagar, Gujarat – 382007, India. E-mail: mailshivamsha@gmail.com
Abstract
Introduction: Scapula fractures usually comprise polytrauma and seldom are operated on, resulting in a dearth of literature and clinical experience. The aim of this case series is to illustrate diverse patterns of scapula fracture and varied reduction and fixation modalities practised in different case scenarios.
Case Report: This is a retrospective descriptive case series, conducted at a teaching tertiary care centre over a period of 1 year. Fifteen patients (14 males and 1 female) of scapula fractures following high-energy trauma, with an average age of 32.5 years, were selected based on the inclusion and exclusion criteria. They were operated on by a single experienced trauma surgeon for internal fixation with a combination of different implant combinations and placements. Variedly classified scapula fractures requiring a specific approach, reduction, and fixation with case-tailored implant positioning are illustrated in detail. Augmentation techniques such as long sub-glenoid screw, dual lateral border construct, concurrent acromion and coracoid fixation using a sabre incision, corresponding intra-articular and extra-articular fracture, and lateral border reduction necessitating medial release using the reverse Judet approach were applied and found to be effective in the restoration of bony anatomy. This was evident by the restoration of radiographic (Cole’s) parameters assessed postoperatively and at 6-month follow-up. Furthermore, augmentation of traditional fixation allows early range of motion and hence a satisfactory functional outcome, as apparent by the Constant-Murley Score assessment at 6-month follow-up.
Conclusion: Scapular fractures have a varied type, which makes accurate classification and visualisation of fracture planes absolutely indispensable. Each pattern requires special consideration for choosing the appropriate surgical approach to achieve adequate reduction and final fixation using specific placement of different implants.
Keywords: Scapula fracture, glenoid fracture, shoulder trauma.
Scapula fractures comprise the body (45%) and glenoid (35%), with 0.4–1% of cases accounting for floating shoulder [1]. The broad spectrum of scapula fractures puts the treating surgeon in a quandary, with most cases being managed non-operatively owing to clinical inexperience or priority given to associated injuries [2]. Distributed and incoherent literature brings no resolve to the predicament of selecting accurate management. This retrospective descriptive case series depicts varied fracture patterns of the scapula and illustrates case-specific surgical approaches, reduction techniques, implant choice, and placement with different modalities of scapula fracture fixation.
After obtaining Institutional Ethics Committee approval at a teaching tertiary care centre, fifteen patients with scapula fracture (14 males and 1 female, average age 32.5 years) following high-energy trauma were selected over 1 year. Inclusion and exclusion criteria were used, and the selected patients included both extra-articular and intra-articular fracture varieties, with some having concurrent acromion, coracoid, or clavicle fractures. After availing the patient’s consent and pre-surgical fitness, they were operated on for open reduction and internal fixation by a single experienced surgeon. The surgical approach was tailored for each case, and fixation was achieved using a combination of different orientations of plates and screw placement, resulting in varied fixation modalities for different patterns of scapula fractures. Restoration of bony anatomy and Cole’s criteria were assessed in plain radiographs as the post-operative and 6-month follow-up radiological outcome measures. Functional assessment was done by evaluating the patients and interpreting the Constant-Murley Score (CMS) at a single 6-month follow-up.
Inclusion criteria:
- Age >18 years
- Operative scapular fractures based on Cole’s operative criteria [3]
- Floating shoulder (Superior Shoulder Suspensory Complex [SSSC] injury).
Exclusion criteria:
- Severely comorbid conditions due to trauma or chest trauma or those requiring intensive care
- Polytrauma cases
- Patients not meeting the surgical indication and managed conservatively
- Patients medically unfit for surgery
- Non-consenting patients.
Case-1: Biplanar lateral pillar construct:
An Ideberg type 5a intra-articular fracture with extra-articular extension may be fixed with a posterior surface 3.5 mm dynamic compression plate (DCP) augmented with a lateral surface 3.5 mm semi-tubular plate using a long (55 mm) subglenoid screw for simultaneous intra-articular fixation. Simultaneous use of lateral and posterior plates over the lateral border makes a stronger biplanar construct. Placing a lateral surface plate along the lateral border may require medialisation of the quadrangular space to expose the glenoid neck, that is, elevating the long head of the triceps off the lateral border, sparing the origin at the infraglenoid tubercle [4]. The medial border is fixed using a contoured 3.5 mm reconstruction plate (Fig. 1).
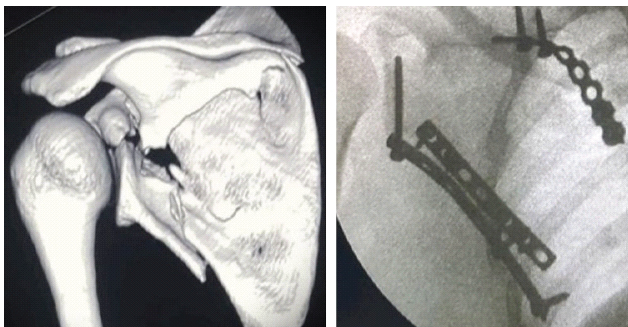
Figure 1: Bi-planar lateral pillar construct.
The preferred sub-glenoid screw directed (towards the coracoid base) usually ranges from 35 mm to 60 mm, the most common being 55 mm, through a semi-tubular or reconstruction plate along the lateral border to augment the posterior surface fixation, making a stronger and more stable biplanar construct.
Case-2: Reduction manoeuvre:
Ideberg type 2 intra-articular glenoid fractures in the axial plane are often irreducible, despite adequate exposure through the posterior approach. Using the coracoid as a fulcrum to achieve reduction by the Kapandji lever technique has a utilitarian benefit in such cases (Fig. 2). 6-month follow-up CMS – 82.

Figure 2: Reduction maneuver.
Case-3: Fixation through reverse Judet approach:
Ideberg Type 5a fracture fixed with anatomical posterior and medial plates with a 3.5 mm cortical screw for glenoid fixation, using the reverse Judet approach [5], which aids in reduction of the lateral pillar by allowing medial release and simultaneous visualization of both the medial and lateral pillars (Fig. 3).
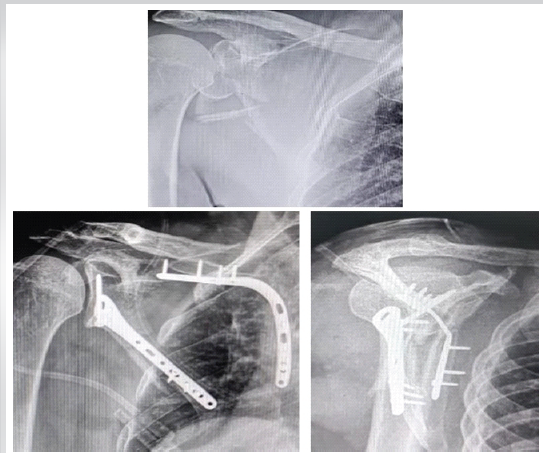
Figure 3: Fixation through Reverse Judet approach.
6-month follow-up CMS – 88.
Case 4: Lost K-wire technique:
Fixation of the extra-articular fracture with lateral border comminution with a K-wire, augmented by final fixation with a 3.5 mm lateral surface plate and a 3.5 mm Ellis T plate distally near the inferior angle through the Brodsky approach or temporary fixation over the medial border through the reverse Judet approach, is typical for comminuted fractures and aids in the reconstruction of the lateral and medial bony pillars. Angulation and medialisation may not be corrected unless fracture fragments over the body and medial border are not completely freed of soft-tissue pull [6] (Figs. 4 and 5). 6-month follow-up CMS – 88.
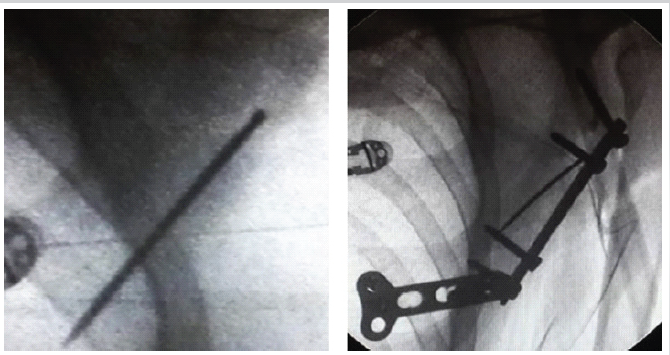
Figure 4: Lost K-wire technique.
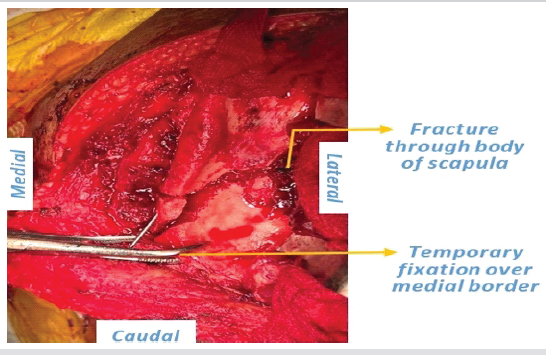
Figure 5: Lost K-wire technique.
Case 5: Bi-planar lateral pillar construct with arthrotomy:
The Ideberg Type 5c combined extra-articular and intra-articular fracture fixation, using a 2.7 mm semi-tubular plate over the posterior surface, augmented with a 3.5 mm long DCP along the lateral surface with a subglenoid screw through the modified Judet approach. Posterior joint arthrotomy was done in line with the posterior glenoid rim, and final fixation was achieved with a small posterior glenoid plate while keeping the posterior and lateral surface plate in situ (Fig. 6). 6-month follow-up CMS – 92.
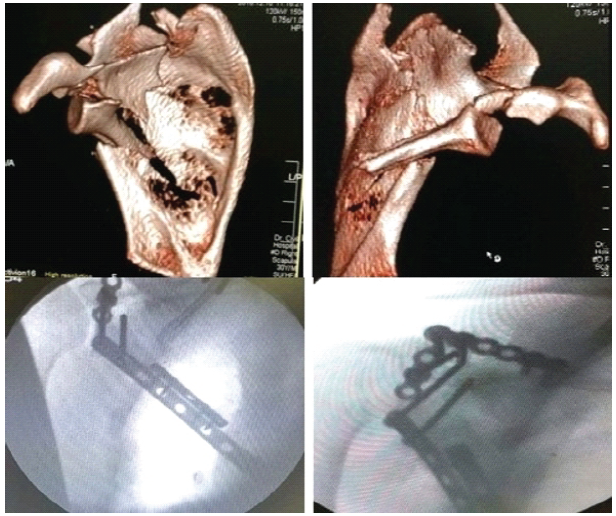
Figure 6: Bi-planar lateral pillar construct with arthrotomy.
Case-6: Contoured distal lateral pillar plate:
An extra-articular fracture with scapular body comminution and angulation was fixed using a medial anatomical plate, proximal lateral surface 3.5 mm semi-tubular plate, and distal posterior surface 3.5 mm reconstruction plate. The distal lateral border was fixed using a 3.5 mm reconstruction plate – proximally aligned along the lateral surface and twisted at 90° distally to contour along the posterior surface to achieve stable fixation of the lateral pillar (Fig. 7).
6-month follow-up CMS – 90.
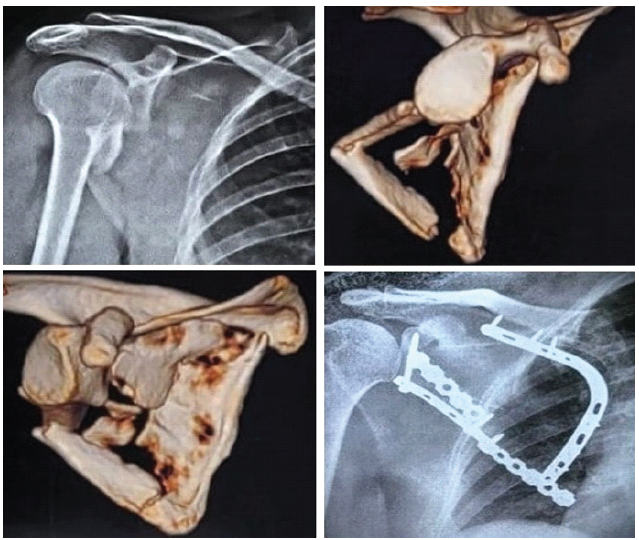
Figure 7: Contoured distal lateral pillar plate.
Case-7: Associated coracoid base fracture
An Ideberg type 5c comminuted scapular body, segmental lateral border with medial extension and coracoid base fracture were fixed using lateral and posterior plates for the lateral pillar, a medial anatomical plate for the medial pillar and a coracoid base screw through a half-sabre incision (Fig. 8). 6-month follow-up CMS – 82.
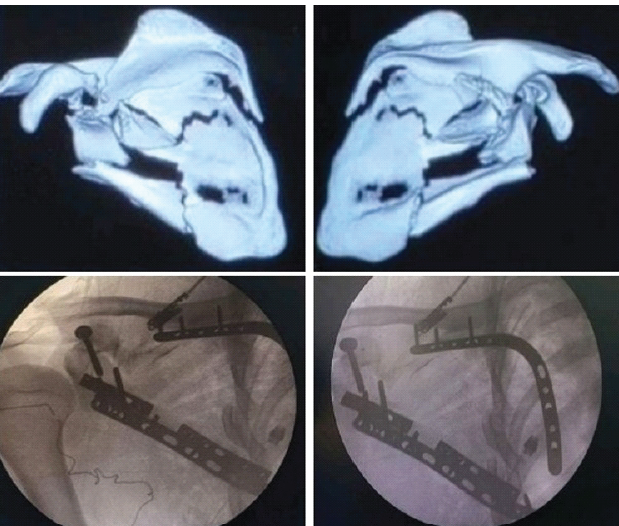
Figure 8: Associated coracoid base fracture.
Case-8: Associated acromion fracture:
An Ideberg type 5a fracture was fixed using a posterior and lateral surface plate with a long (60 mm) sub-glenoid screw and acromion fixation using a plate with tension band wiring through the reverse Judet approach (Fig. 9). 6-month follow-up CMS – 78.
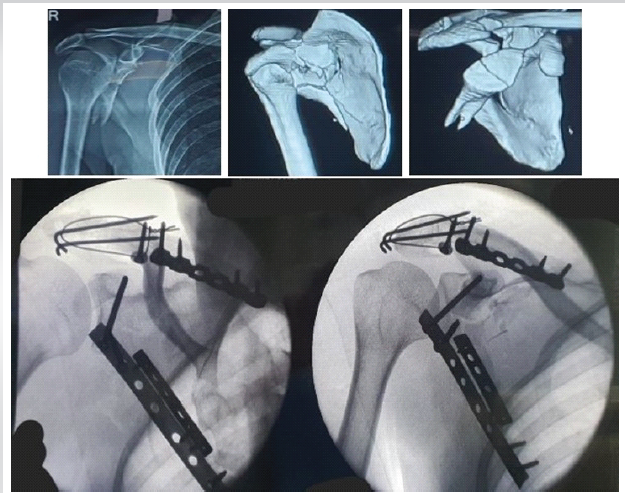
Figure 9: Associated acromion fracture.
Case 9: Temporary fixation, associated acromion fracture:
A comminuted Ideberg type 5a fracture was temporarily fixed with two posterior surface 3.5 mm semi-tubular plates and removed after final fixation with a 3.5 mm semi-tubular plate over the lateral surface with a long subglenoid screw and a 3.5 mm semi-tubular plate for the acromion, all by a single reverse Judet approach. Screw sizes over the medial and lateral border posterior plates range from 12 mm at thin cortices to 16 mm at thick cortices (Fig. 10). 6-month follow-up CMS – 86.
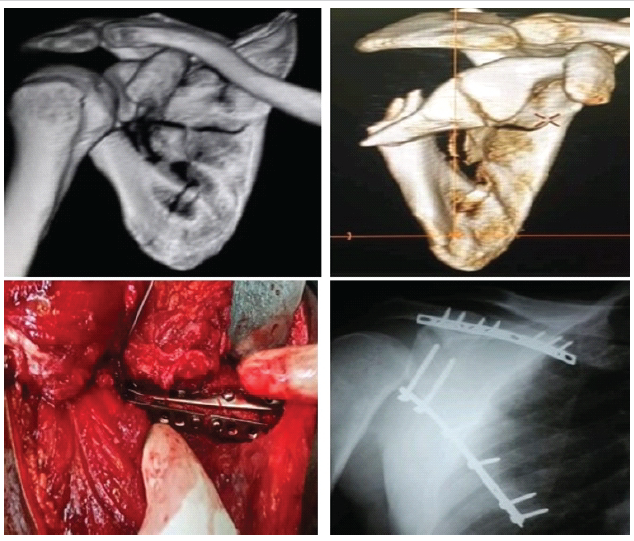
Figure 10: Temporary fixation, associated acromion fracture.
Case-10: Percutaneous glenoid fixation.
Arthroscopy-assisted percutaneous fixation [7] for Ideberg type 3 displaced glenoid fractures through a superior or posterior portal aids in achieving accurate reduction of the glenoid articular margin and allows stable fixation while avoiding drawbacks associated with open dissection (Fig. 11). 6-month follow-up CMS – 90.
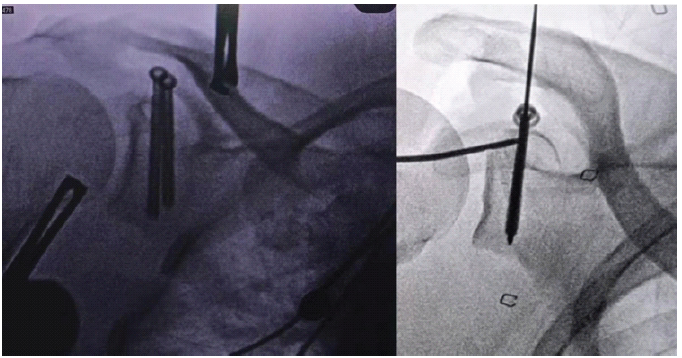
Figure 11: Percutaneous glenoid fixation.
Case-11: Associated clavicle fracture (SSSC injury – floating shoulder):
An extra-articular comminuted glenoid neck fracture with medial border, acromion, and clavicle fractures was managed with lateral and medial pillar acromion plating through the reverse Judet approach and anterior clavicle plating (Fig. 12). 6-month follow-up CMS – 88. (Table 1).
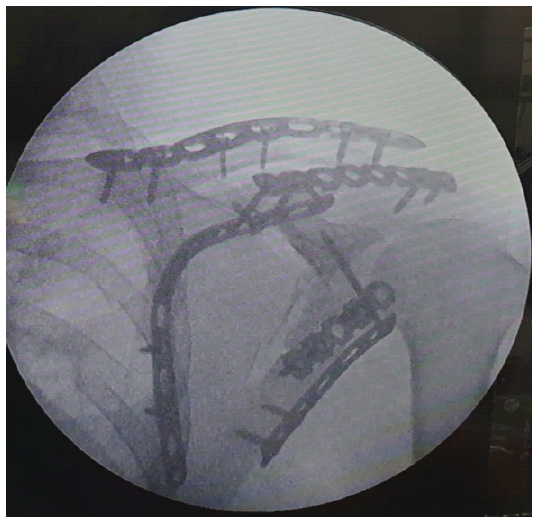
Figure 12: Associated clavicle fracture (Superior shoulder suspensory complex injury – floating shoulder).

Scapula fractures, often prone to “benign neglect”, if managed conservatively, may lead to loss of shoulder function due to malalignment or arthrosis, scapula-thoracic dyskinesia, and impingement pain. Operative fixation of scapula fractures, when indicated, is crucial for a satisfactory clinical outcome, as evident in studies by Herrera et al. [8], Bartoníček and Frič [9], Cole et al., and Schroder et al. [10]. The functional outcomes depend on a thoughtful management protocol designed on a cumulative consideration of patient profile, fracture pattern, and associated injuries. Surgical management often comes with challenges in the form of preoperative planning, surgical exposure, intraoperative handling of vital structures, accurate reduction, and strong fixation. This case series delves into various cases of scapular fractures and narrates how each was managed for the sake of reference of fellow orthopaedic surgeons. Choosing the right patient according to fracture classification, operative indication, patient bio-profile, and injury characteristics is vital. Furthermore, the most essential part of preoperative planning is selecting the most suitable approach – one which provides the most abundant exposure, allows easy manipulation of fracture fragments, and helps achieve varied hardware implantation. Taking any posterior approach to the scapula essentially involves dissection along the interval of the infraspinatus and teres minor. This interval may be identified by two methods: either looking for the direction of fibres starting laterally and tracing them medially, or alternatively, locating the teres minor fibre’s origin over the inferior angle of the scapula and tracing its run at a greater angle towards the humeral head. Authors found the reverse Judet approach aids in several aspects, which are as follows:
Merits of the reverse Judet approach:
- Greater exposure of multiple anatomical structures at once
- Both extra-articular and intra-articular can be addressed with a single approach
- Manipulation at both medial and lateral borders together, that is, exposure of bony elements of the scapula having adequate bone stock for internal fixation
- Allows plate placement over the lateral surface while manipulating the scapular body and medial border
- Prevention of misdiagnosis of concomitant supra-scapular nerve injury through dissection of spinoglenoid notch to rule out nerve entrapment (leading cause of infraspinatus atrophy)
- Allows exposure for open wedge osteotomy to address recurrent posterior shoulder dislocation
- Allows addressing lateral body fixation without removing the deltoid from scapular spine by wide abduction of the arm, aiding early mobilization and rehabilitation, without the need to wait for muscle healing
- Allows a stronger biplanar construct
- Best suited for comminuted fractures of the scapular body involving both medial and lateral pillars, intra-articular fractures involving the body and the acromion or coracoid processes, or cases with lateral border fixation requiring medial release
- Chen [11] concluded that the reverse Judet approach shortens the duration of surgery, reduces blood loss, and allows sufficient exposure for reduction and achieving stable fixation, thus allowing for early functional range of motion, proving to be a safe and efficient method for surgical fixation of complicated scapula fractures.
Often overlooked, some important aspects change the outcome of any case. Priority must be given to intra-articular fracture (i.e., reduction of articular step-off) in the presence of simultaneous extra-articular fracture to avoid painful arthritis. Reduction must be assessed in three views – Grashey AP view/Neer I projection, Y (outlet) view/Neer II projection, and axillary view. Screw penetration must be checked before closure that can result in a painful range of motion and early arthritis, which is visible in the Neer I and axillary views. The rotator cuff must be repaired, and the capsule should be closed. The Allgower-Donati suture technique may be preferred to preserve lateral flap vascularisation. Of importance is avoiding vital structures around the scapula. Wijdicks et al. [12] have characteristically identified critical danger zones comprising neurovascular structures. This includes a 4-7 cm triangle centred along the spinoglenoid notch, constituting essentially the suprascapular nerve and the ascending branch of the circumflex scapular artery. These must be carefully handled in any posterior approach to the scapula nearing the scapular neck. In this case series, there was no complication in either of the cases, and post-operative radiological criteria were met and found to be satisfactory. Authors acknowledge limitations of this study pertaining to the small sample size and lack of long-term outcome measure, but each is of value since they provide either a newer or an augmentation of previously existing fixation methods for various scapula fractures. It is highlighted that the dissection and surgical approaches used are already existent in the literature and widely practised. Furthermore, the series does not intend to establish the superiority of any single fixation technique; rather, it showcases augmentation to existing methods of fixation and adds to the knowledge of any operating orthopaedic surgeon some reduction techniques which can come in handy in everyday surgical practice. The reduction manoeuvres and augmentation techniques for existing fixation methods provide a better reduction as measured in a post-operative radiograph and on a 6-month follow-up and allow early range of motion. Functional evaluation using the CMS at a single 6-month follow-up of all cases placed twelve patients in the very good (86–100) category, whereas three patients fell in the good category (71–85), evident of a satisfactory outcome. Authors acknowledge that the study’s small sample size (n = 15), retrospective design, single-centre setting, and single-surgeon experience limit the strength of the evidence and the generalisability of the findings. They further advocate for a cohort study with a large sample size to assess and compare the functional outcomes with radiological parameters for long-term outcomes.
The case series illustrates the fact that scapular fractures have a diverse presentation, necessitating accurate classification and fracture plane visualisation. Each pattern requires special consideration while choosing the surgical approach, appropriate reduction technique, and varied implant placement to achieve a strong and rigid fixation to meet the post-operative criteria. The presented case series demonstrates the feasibility of various reduction and fixation strategies in selected patients and provides technical insights that may assist surgeons managing similar injuries. Authors emphasise that larger prospective studies with standardised protocols, comparative cohorts, and long-term follow-up are necessary before definitive recommendations can be made.
Diverse scapula fracture patterns require varied reduction and fixation modalities practiced in different case scenarios.
References
- 1. Schmidt V, Mukka S, Bergdahl C, Ekholm C, Brüggemann A, Wolf O. Epidemiology, treatment, and mortality of 3973 scapula fractures from the Swedish fracture register. J Shoulder Elbow Surg 2025;34:e47-56. [Google Scholar] [PubMed]
- 2. Kannan S, Singh HP, Pandey R. A systematic review of management of scapular fractures. Acta Orthop Belg 2018;84:497-508. [Google Scholar] [PubMed]
- 3. Cole PA, Freeman G, Dubin JR. Scapula fractures. Curr Rev Musculoskelet Med 2013;6:79-87. [Google Scholar] [PubMed]
- 4. Gauger EM, Cole PA. Surgical technique: A minimally invasive approach to scapula neck and body fractures. Clin Orthop Relat Res 2011;469:3390-9. [Google Scholar] [PubMed]
- 5. Manohara R, Kumar VP. A reverse judet approach to the scapula. Arch Orthop Trauma Surg 2018;138:669-73. [Google Scholar] [PubMed]
- 6. Pires RE, Giordano V, de Souza FS, Labronici PJ. Current challenges and controversies in the management of scapular fractures: A review. Patient Saf Surg 2021;15:6. [Google Scholar] [PubMed]
- 7. Marsland D, Ahmed HA. Arthroscopically assisted fixation of glenoid fractures: A cadaver study to show potential applications of percutaneous screw insertion and anatomic risks. J Shoulder Elbow Surg 2011;20:481-90. [Google Scholar] [PubMed]
- 8. Herrera DA, Anavian J, Tarkin IS, Armitage BA, Schroder LK, Cole PA. Delayed operative management of fractures of the scapula. J Bone Joint Surg Br 2009;91:619-26. [Google Scholar] [PubMed]
- 9. Bartoníček J, Frič V. Scapular body fractures: Results of operative treatment. Int Orthop 2011;35:747-53. [Google Scholar] [PubMed]
- 10. Schroder LK, Gauger EM, Gilbertson JA, Cole PA. Functional outcomes after operative management of extra-articular glenoid neck and scapular body fractures. J Bone Joint Surg Am 2016;98:1623-30. [Google Scholar] [PubMed]
- 11. Chen Y. Evaluation of reverse Judet approach in the treatment of scapular body complicated fractures. Int J Surg 2021;12:760-3. [Google Scholar] [PubMed]
- 12. Wijdicks CA, Armitage BM, Anavian J, Schroder LK, Cole PA. Vulnerable neurovasculature with a posterior approach to the scapula. Clin Orthop Relat Res 2009;467:2011-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Shoulder Injuries Secondary to Proning: Sequelae of Long COVID Syndrome: A Case Report
July 1, 2026 Shoulder Injuries Secondary to Proning: Sequelae of Long COVID Syndrome: A Case Report May 1, 2026 Arthroscopic Fixation of Acute Reverse Bony Bankart Lesion using Cancellous Cannulated Screws: A Rare Case Report
May 1, 2026 Arthroscopic Fixation of Acute Reverse Bony Bankart Lesion using Cancellous Cannulated Screws: A Rare Case Report November 1, 2025 Definitive Management of Open Clavicle Fracture with Locking Compression Plate as External Fixator
November 1, 2025 Definitive Management of Open Clavicle Fracture with Locking Compression Plate as External Fixator August 1, 2025 Fixation of Displaced Lateral Column and Spine of Scapula using Modified Judet Approach
August 1, 2025 Fixation of Displaced Lateral Column and Spine of Scapula using Modified Judet Approach