
Eosinophilic synovitis can mimic septic arthritis in children, necessitating careful diagnostic evaluation to guide appropriate management.
Dr. Sharafuddeen Mammu, Department of Orthopaedics, Fathima Hospital, Kozhikode, Kerala, India. E-mail: sharafuddeen786@gmail.com
Abstract
Introduction: Eosinophilic synovitis, though rare, can closely mimic septic arthritis in children, often complicating diagnosis. This inflammatory condition is typically linked to allergic reactions or parasitic infections, though idiopathic cases have been documented.
Case Report: We describe a 4-year-old boy initially diagnosed with septic arthritis of the knee. The patient underwent arthrotomy, and synovial fluid analysis surprisingly revealed significant eosinophilia. Histopathology confirmed eosinophilic synovitis. Following a 3-week course of diethylcarbamazine (DEC), the patient achieved full recovery with no recurrence.
Conclusion: This case emphasizes the importance of synovial fluid analysis in pediatric monoarticular joint swelling, as eosinophilic synovitis should be considered in differential diagnoses to avoid misdiagnosis and unnecessary interventions.
Keywords: Septic arthritis, synovitis, eosinophilia, diethylcarbamazine.
Knee swelling in pediatric patients presents a diagnostic challenge, with septic arthritis being a primary concern due to its potential for rapid joint destruction and long-term disability if left untreated [1,2]. The diagnostic approach relies on clinical presentation, inflammatory markers, and synovial fluid analysis to differentiate infectious from non-infectious causes. However, conditions that mimic septic arthritis, such as eosinophilic synovitis, can complicate decision-making and potentially lead to unnecessary surgical interventions [3,4]. Eosinophilic synovitis is an exceptionally rare entity, with its exact incidence not well-documented in the literature. However, Vázquez-Triñanes et al. analyzed 982 synovial fluid samples and found that synovial fluid eosinophilia had a prevalence of 1.02%, highlighting its rarity and the potential for misdiagnosis [5]. Despite this finding, eosinophilic synovitis remains poorly understood, with limited case reports available, making it a diagnostic challenge. Eosinophilic synovitis can involve various joints, with the knee being the most commonly affected. Other joints such as the hip, ankle, and elbow may also be involved, but reports are limited. The etiology remains unclear, though hypersensitivity reactions, environmental allergens, food allergens, drug hypersensitivity, and parasitic infections (e.g., filariasis, schistosomiasis, toxocariasis) have been implicated [6,7]. Despite these associations, many cases remain idiopathic, with no identifiable underlying trigger. Histopathological examination remains the gold standard for diagnosing eosinophilic synovitis. Key findings include marked eosinophilic infiltration of the synovial membrane, synovial hypertrophy, fibrosis, and microvascular proliferation. The presence of eosinophilic-rich inflammatory infiltrates on biopsy confirms the diagnosis, helping to distinguish eosinophilic synovitis from other inflammatory arthropathies [8,9]. The standard approach for managing a swollen, painful joint with fever and restricted motion in pediatric patients involves joint aspiration, followed by arthrotomy if necessary. Given the rarity of eosinophilic synovitis, arthrotomy should not be considered an unnecessary intervention, especially when performed to exclude septic arthritis. However, a normal C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) in acute synovitis should raise suspicion for eosinophilic synovitis, allowing for careful monitoring as an alternative to immediate surgical intervention. This case report emphasizes the importance of recognizing eosinophilic synovitis as a rare but significant differential diagnosis in pediatric knee arthritis. Awareness of its distinct histopathological and clinical features may help prevent unnecessary surgical interventions, optimize patient outcomes, and guide appropriate management strategies.
A previously healthy 4-year-old boy presented with acute pain and swelling in the left knee, which had been progressively worsening over the past 2 days and was associated with fever. The patient had no history of recent systemic infections or trauma. In addition, there were no symptoms of cough with expectoration, gastrointestinal issues such as diarrhea or dysentery, or any similar episodes in the past. The family history was also unremarkable for comparable illnesses. On physical examination, the child was febrile and appeared ill. Notable findings included localized warmth and swelling around the left knee, with significant pain on attempted movement of the joint (Fig. 1). The hip joint was assessed and found to be clinically normal. There was no evidence of inguinal or popliteal lymphadenopathy, and the systemic examination was otherwise unremarkable. 
Radiographic evaluation of the left knee showed normal bone morphology but indicated capsular distension and soft-tissue expansion (Fig. 2). Ultrasound imaging revealed a moderate amount of joint effusion with coarse internal echoes. Given the clinical presentation and examination findings, the differential diagnosis included reactive synovitis, juvenile arthritis, low-grade septic arthritis, and effusion due to blood dyscrasia.

Further investigations were conducted to refine the diagnosis. Blood tests included a complete blood count with peripheral smear, ESR, CRP, rheumatoid factor, anti-nuclear antibody, Filaria card test (antigen), and serum immunoglobulin E. Stool examination for ova and cysts was performed and returned negative. Laboratory tests demonstrated leucocytosis with an elevated polymorph count and a notable increase in eosinophil count, which was 29%. The ESR was 18 mm/h, and the CRP level was 3 mg/L (Table 1).

Despite normal CRP levels, the clinical presentation and imaging findings were highly suggestive of septic arthritis. Due to the challenges associated with performing arthrocentesis in young children without anesthesia, this procedure was not undertaken. After thorough consultation with the pediatrician, sonologist, and pediatric orthopedician, it was decided to proceed with management under the assumption of septic arthritis.
At our hospital, we follow a standard septic arthritis treatment protocol (Fig. 3), which was promptly initiated. The child underwent an arthrotomy of the left knee.

In this case, a lateral suprapatellar arthrotomy was performed instead of a medial approach. This choice was made to avoid injury to the medial retinaculum and medial patellofemoral ligament, both of which are critical for patellar stability. The lateral approach minimizes the risk of postoperative patellar instability, making it the preferred surgical technique in this case. A lateral incision, approximately 4 cm in length, was made at the superior lateral border of the patella. This incision was deepened to expose and open the knee capsule laterally. The serosanguinous fluid was drained, which exhibited normal threadability, and was sent for comprehensive analysis. Synovial tissue was also collected for histopathological examination. The skin was closed over a drain to facilitate fluid removal and minimize the risk of infection. Broad-spectrum antibiotic therapy with intravenous cefuroxime was commenced. The child’s condition improved significantly, and the drain was removed after 48 h. The patient was discharged after a total hospital stay of 5 days. Throughout the illness, CRP levels remained normal. Cultures of the aspirated fluid did not yield any microbial growth, and the histopathology results confirmed the diagnosis of eosinophilic synovitis with synovial tissue showing dense inflammation with eosinophilic predominance (Fig. 4).

Following the confirmation of eosinophilic synovitis, the patient was treated with oral diethylcarbamazine (DEC) for a duration of 3 weeks. The DEC therapy led to a normalization of blood parameters, a significant improvement in the range of knee movements, and a complete resolution of symptoms. There were no further episodes of pain or swelling observed during the follow-up period (Fig. 5).

The challenge of diagnosing knee swelling in pediatric patients is compounded by the need to distinguish between septic arthritis and other less common conditions. Septic arthritis is a serious condition that necessitates prompt treatment to avoid severe joint damage, including deformities and long-term complications such as limb length discrepancies [1,2]. The diagnostic process often relies heavily on clinical evaluation alongside investigative techniques like joint lavage, which help to confirm or exclude infection [3,4]. In this context, eosinophilic synovitis emerges as a rare but important condition to consider. This form of synovitis, marked by high eosinophil counts in the synovial fluid, can closely mimic septic arthritis, creating diagnostic challenges [6]. The association of eosinophilic synovitis with allergic and parasitic conditions is well-documented, although it can also occur without a clear underlying cause [7,8]. A notable study conducted in southwestern India identified eosinophilic synovitis in 12 out of 72 patients with knee synovitis. Despite the rarity of peripheral eosinophilia, these cases had synovial fluid eosinophil levels exceeding 60%, indicating that eosinophilic synovitis can occur even when peripheral eosinophil counts are not elevated [9]. This finding emphasizes the importance of evaluating synovial fluid in the diagnostic process. Further evidence from New Zealand highlights that eosinophilia is present in 15.6% of cases of transient synovitis of the hip, a rate significantly higher than the incidental eosinophilia observed in the general population [10]. Eosinophilic synovitis is categorized based on the proportion of eosinophils in the synovial fluid: major eosinophilic synovitis if eosinophils constitute more than 10% of the total leukocytes, and minor eosinophilic synovitis if eosinophils are <10% [11]. This classification aids in distinguishing eosinophilic synovitis from other types of synovitis, such as those associated with tuberculosis or rheumatoid arthritis [12]. Diagnosis typically involves confirming high eosinophil counts in the synovial fluid and may be supported by synovial biopsy, which reveals eosinophilic infiltrates in the hypertrophied synovium. Eosinophilic synovitis is often observed in the knee joint, primarily affecting adolescent girls, and can present as either monoarticular or oligoarticular [13]. Treatment generally involves NSAIDs, which usually result in significant symptom relief within a week. In addition, DEC has been found to be effective in managing eosinophilic synovitis, with research indicating that a 3-week course of DEC can lead to substantial symptom reduction and decreased peripheral eosinophilia, with no recurrence [14]. In this case, the patient was treated with oral DEC. DEC therapy, administered for 3 weeks, resulted in significant clinical improvement. The patient’s blood parameters normalized, and there was a substantial improvement in the range of knee movements with no recurrence of symptoms. DEC is beneficial in treating eosinophilic synovitis as it directly targets the eosinophilia, addressing the underlying cause of the inflammation and facilitating recovery.
This case illustrates the diagnostic complexity and management challenges associated with knee swelling in pediatric patients. This case emphasizes the importance of considering eosinophilic synovitis in differential diagnoses, the value of a multidisciplinary approach, and the need for tailored treatment strategies to ensure optimal outcomes in pediatric patients with atypical joint inflammation presentations.
This case highlights the importance of including eosinophilic synovitis in differential diagnoses for pediatric knee swelling, underscoring the need for a multidisciplinary approach and personalized treatment to achieve the best outcomes in children with uncommon inflammatory presentations.
References
- 1.Laor T, Horn BD. Evaluation and management of septic arthritis in children. Pediatric Emerg Med 2017;22:265-73. [Google Scholar | PubMed]
- 2.Dajani AS, Taubert KA. Infectious arthritis in children: Diagnosis and management. Clin Infect Dis 2020;71:221-8. [Google Scholar | PubMed]
- 3.Weiss J, Noonan T. Pediatric septic arthritis: A review of the diagnostic and management strategies. J Pediatric Orthop 2019;39:305-13. [Google Scholar | PubMed]
- 4.Haddad R, Wilkins K. Joint lavage and aspiration: Techniques and indications. Orthop Clin North Am 2018;49:573-81. [Google Scholar | PubMed]
- 5.Vázquez-Triñanes C, Sopena B, González-González L, Díaz R, Rivera A, Freire M, et al. Synovial fluid eosinophilia: A case series with a long follow-up and literature review. Rheumatol (Oxford) 2013;52:346-51. [Google Scholar | PubMed]
- 6.Roth J, Jansen C. Eosinophilic synovitis in children: A case report and review of the literature. Clin Rheumatol 2019;38:2785-92. [Google Scholar | PubMed]
- 7.Gupta V, Singh H. Challenges in diagnosing eosinophilic synovitis in children: A case report and literature review. Int J Rheum Dis 2017;20:1053-9. [Google Scholar | PubMed]
- 8.Kim SY, Lee JH. Eosinophilic synovitis: A case report and literature review. Int J Rheum Dis 2018;21:558-62. [Google Scholar | PubMed]
- 9.Tauro B, Muralidharagopalan NR. Eosinophilic synovitis in Southwestern India: A study of 12 cases. Indian J Rheumatol 1995;1:45-50. [Google Scholar | PubMed]
- 10.Alamri A, Russell D. Transient synovitis of the hip and its association with eosinophilia: A new Zealand perspective. J Pediatric Orthop 2020;40:300-5. [Google Scholar | PubMed]
- 11.Edwards CJ, Lee M. Management of eosinophilic synovitis in pediatric patients: Clinical insights and treatment options. Rheumatol Adv Pract 2023;7:rkac019. [Google Scholar | PubMed]
- 12.Kim HS, Lee JJ. Role of joint lavage in pediatric septic arthritis: A case series. J Pediatric Rheumatol 2021;23:29-34. [Google Scholar | PubMed]
- 13.Akikusa JD, Burgess M. Eosinophilic synovitis in children: A rare but important differential diagnosis. Pediatric Rheumatol Online J 2020;18:18. [Google Scholar | PubMed]
- 14.Muralidharagopalan NR, Suresh K. Diethylcarbamazine in the treatment of eosinophilic synovitis. Indian J Pediatric 1999;66:835-8. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Sub-acute Septic Arthritis of the Knee by Candida vishwanathii: Two Rare Case Reports and Review of Literature
August 1, 2026 Sub-acute Septic Arthritis of the Knee by Candida vishwanathii: Two Rare Case Reports and Review of Literature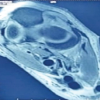 July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report
July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report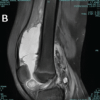 July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult
July 1, 2026 Atypical Presentation of MRSA Septic Arthritis with Concurrent Pyomyositis of the Calf Muscles in an Immunocompetent Adult