
Concurrent pyomyositis with septic arthritis can present without systemic symptoms. A high index of suspicion, early imaging, and interdisciplinary collaboration can dramatically improve outcomes.
Dr. Sameer Tyagi, Consultant Orthopedic Surgeon, Holy Family Hospital, Mumbai, Maharashtra, India. E-mail: drsameertyagi@gmail.com
Abstract
Introduction: Concurrent pyomyositis and septic arthritis without systemic symptoms is uncommon and may delay diagnosis.
Case Report: A 36-year-old immunocompetent male presented with isolated right knee swelling, without fever or trauma. Magnetic resonance imaging revealed joint effusion and myositis in surrounding muscles. Joint aspiration confirmed Methicillin-resistant Staphylococcus aureus septic arthritis. Despite intravenous antibiotics, a growing intramuscular abscess in the gastrocnemius was detected on serial ultrasound. Surgical drainage was performed. The patient was treated with IV vancomycin for 2 weeks, followed by oral linezolid, and recovered fully.
Conclusion: Pyomyositis should be considered in septic arthritis with atypical presentations. Serial imaging and inflammatory markers are essential for guiding treatment.
Keywords: Methicillin-resistant Staphylococcus aureus, septic arthritis, pyomyositis, gastrocnemius, vancomycin, C-reactive protein, immunocompetent, knee joint.
Septic arthritis coexisting with pyomyositis is typically seen in immunocompromised individuals or tropical regions. However, such presentations in otherwise healthy patients, especially without systemic signs, such as fever, are rare. This case emphasizes the importance of considering muscle involvement in joint infections, even when classical symptoms are absent.
Pyomyositis, a primary bacterial infection of skeletal muscle, has traditionally been associated with tropical climates and immunocompromised states, such as HIV infection, diabetes mellitus, malignancy, or corticosteroid use [1,2]. However, recent literature suggests an increasing incidence of pyomyositis in immunocompetent individuals and in temperate regions [3-6]. Staphylococcus aureus remains the most common causative organism, with methicillin-resistant strains methicillin-resistant S. aureus (MRSA) increasingly implicated in musculoskeletal infections [5,6]. The coexistence of pyomyositis with septic arthritis is uncommon and may occur due to contiguous spread or hematogenous dissemination [3].
Importantly, the diagnosis of pyomyositis is frequently delayed due to its insidious onset and non-specific clinical presentation, particularly in the absence of systemic symptoms, such as fever [7,8]. Advanced imaging, especially magnetic resonance imaging (MRI), plays a crucial role in early detection of muscle involvement, while ultrasound is valuable for identifying evolving abscesses and guiding intervention [7].
Recent reports, including a case series by Shukla et al. [10], have demonstrated that pyomyositis can present in immunocompetent individuals without classical systemic features, further contributing to diagnostic challenges.
A 36-year-old healthy male presented to the Orthopaedic Unit at Holy Family Hospital, Mumbai, with a 4-day history of right knee swelling. He denied trauma, fever, or constitutional symptoms.
Clinical examination:
- Tense knee effusion
- Mild warmth
- Restricted flexion
- No systemic toxicity.
Timeline of events:
- Day 1–4: Knee swelling without fever
- Day 4: MRI showed joint effusion with myositis (Fig 1, 2, 3). An ultrasound showed collection in gastrocnemius muscle
- Day 5: Joint aspiration → MRSA confirmed by culture (Fig. 4)
- Day 5–7: IV antibiotics switched to targeted antibiotics as per sensitivity (piperacillin-tazobactam → vancomycin)
- Day 8–10: C-reactive protein (CRP) plateau observed (Fig. 5)
- Day 10: Repeat ultrasonography → gastrocnemius collection increased instead of subsiding despite targeted antibiotics (Fig. 7)
- Day 11: Surgical incision and drainage performed; culture sent confirmed the bacteria in the intramuscular collection as isolated from the synovial fluid (Fig. 8).
- Post-operative: CRP decline and clinical improvement
- 4 weeks: Full recovery.
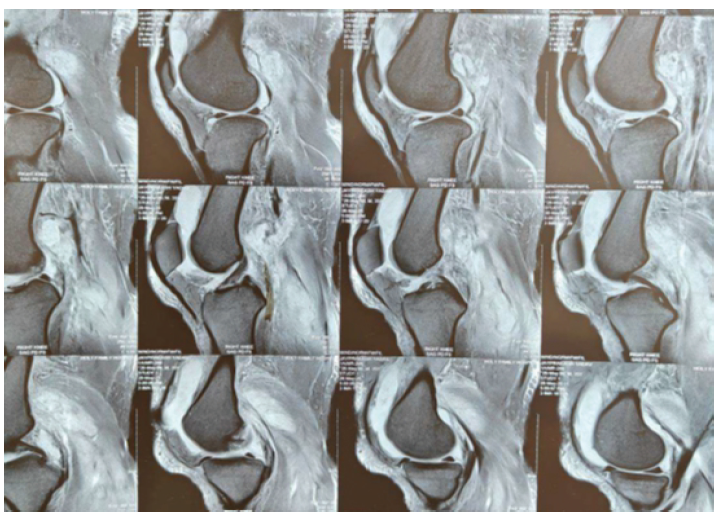
Figure 1: Magnetic resonance imaging (MRI) of the right knee (sagittal T2-weighted fat-suppressed image) showing moderate joint effusion with synovial enhancement and surrounding muscle edema suggestive of myositis. Usually, pyomyositis is diagnosed late, an immunocompetent individual presenting with only knee swelling, is likely to receive treatment for a few weeks before the infection spreads to other areas, one of the important points in this case was that the patient presented early to an orthopedic surgeon who ordered an MRI of the knee which also incidentally picked up the pus collections in the muscles making a diagnosis of pyomyositis.
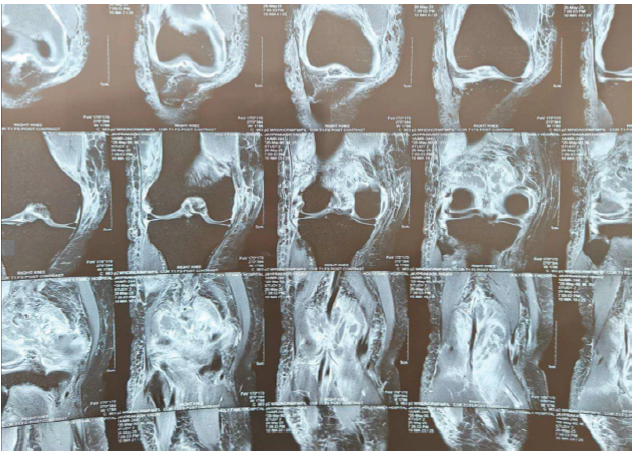
Figure 2: Coronal magnetic resonance imaging image of the knee showing intramuscular collections.
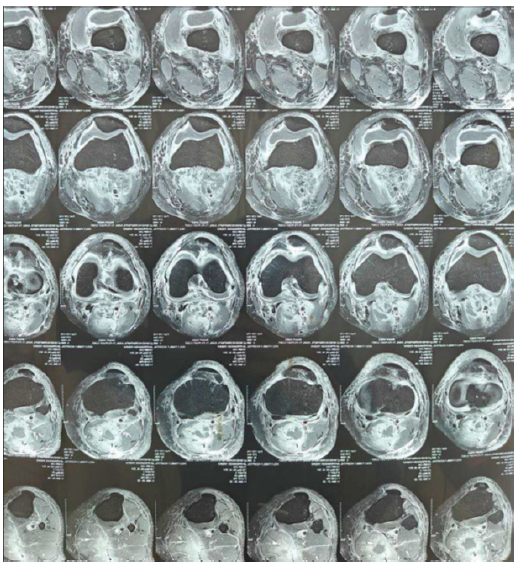
Figure 3: Magnetic resonance imaging axial T2-weighted image showing diffuse hyperintensity in the vastus lateralis, vastus medialis, and medial gastrocnemius muscles consistent with pyomyositis.
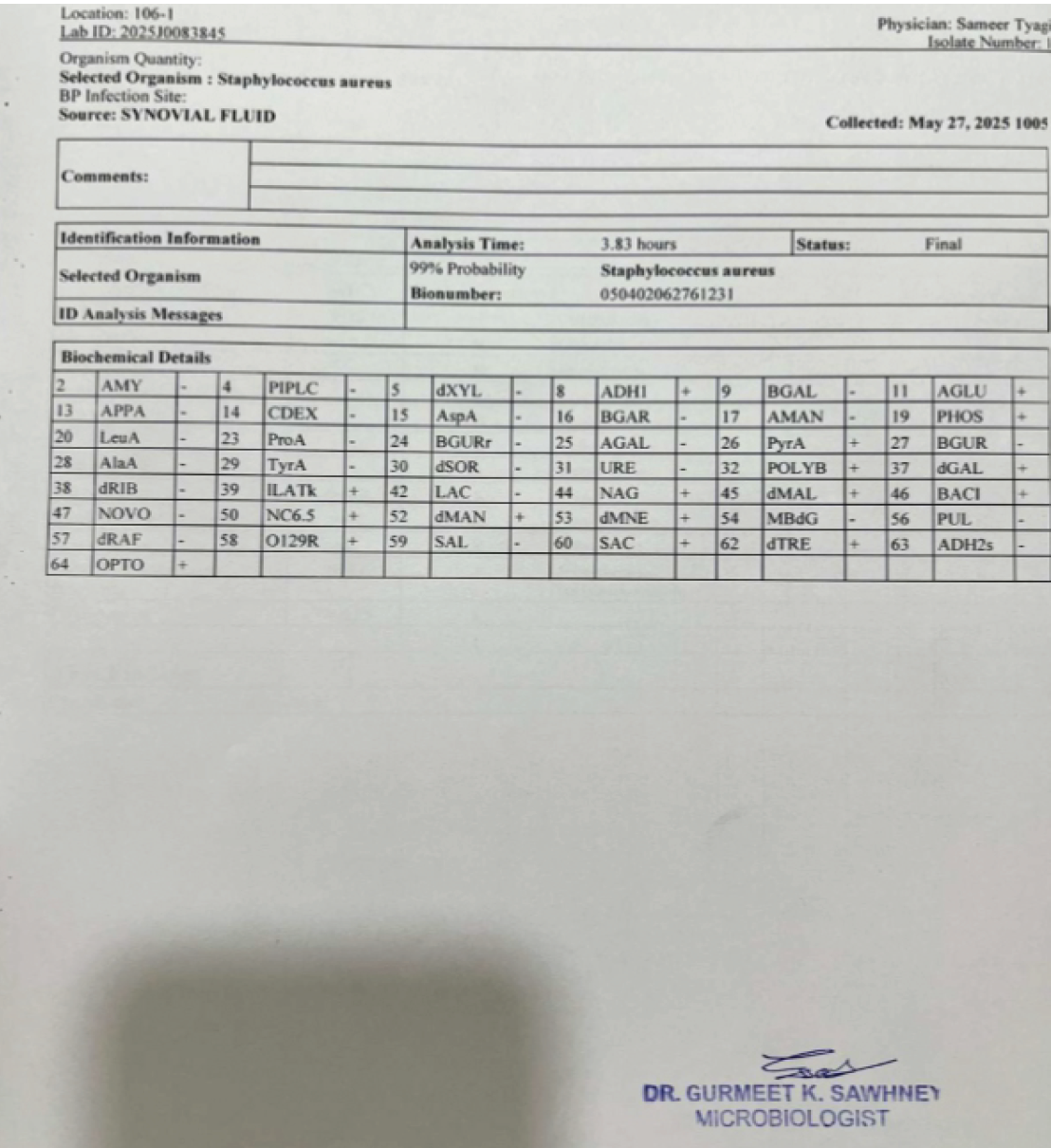
Figure 4: Knee was aspirated and synovial fluid sent for culture, which led to identification of Methicillin-resistant Staphylococcus aureus (culture report attached below). Injection of vancomycin was started for this; however, C-reactive protein and total leukocyte count values did not decrease, which led to the decision of incision and drainage. Culture Vitech identification (99% probability) and sensitivity reports with mic values of synovial fluid and pus.
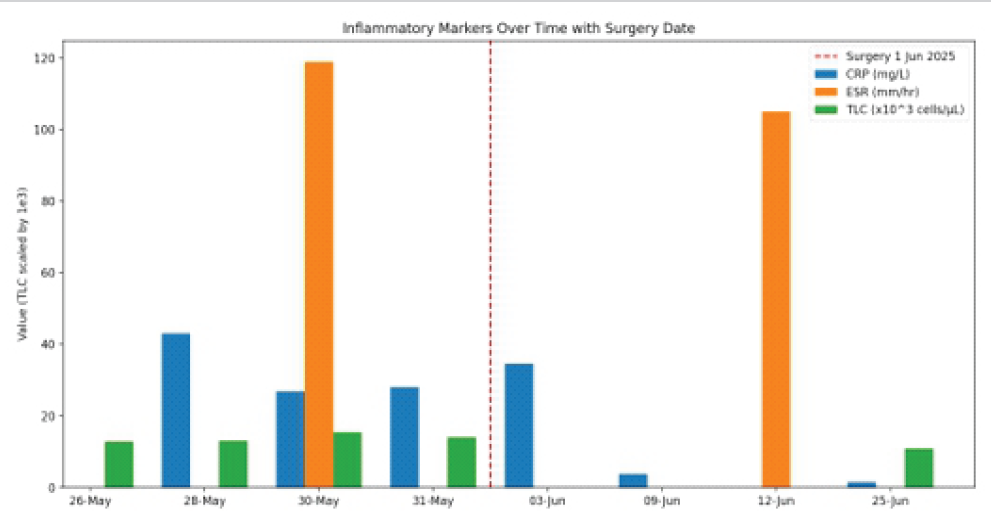
Figure 5: Trend of inflammatory markers (C-reactive protein [CRP], erythrocyte sedimentation rate, total leukocyte count [TLC]) over time in relation to surgery date (1 June 2025). Serial evaluation of Inflammatory markers and TLC shows raised values even after targeted antibiotic therapy. The CRP plateau prompted repeat ultrasound and surgical drainage, followed by steady post-operative decline.
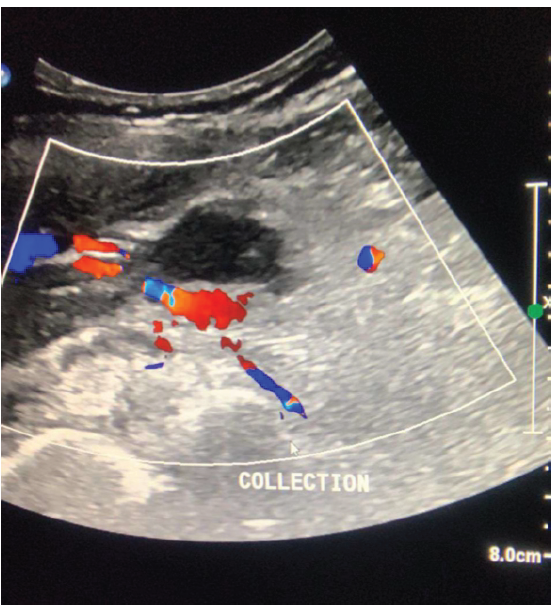
Figure 6: First ultrasound of gastrocnemius collection 27 May 2025. Ultrasound image with color Doppler showing anechoic intramuscular collection with internal echoes and peripheral vascularity in the medial gastrocnemius muscle (27 May 2025).

Figure 7: Repeat ultrasound showing increased size (instead of expected decrease) of the medial gastrocnemius collection despite ongoing IV vancomycin therapy (31 May 2025) which prompted surgical drainage.
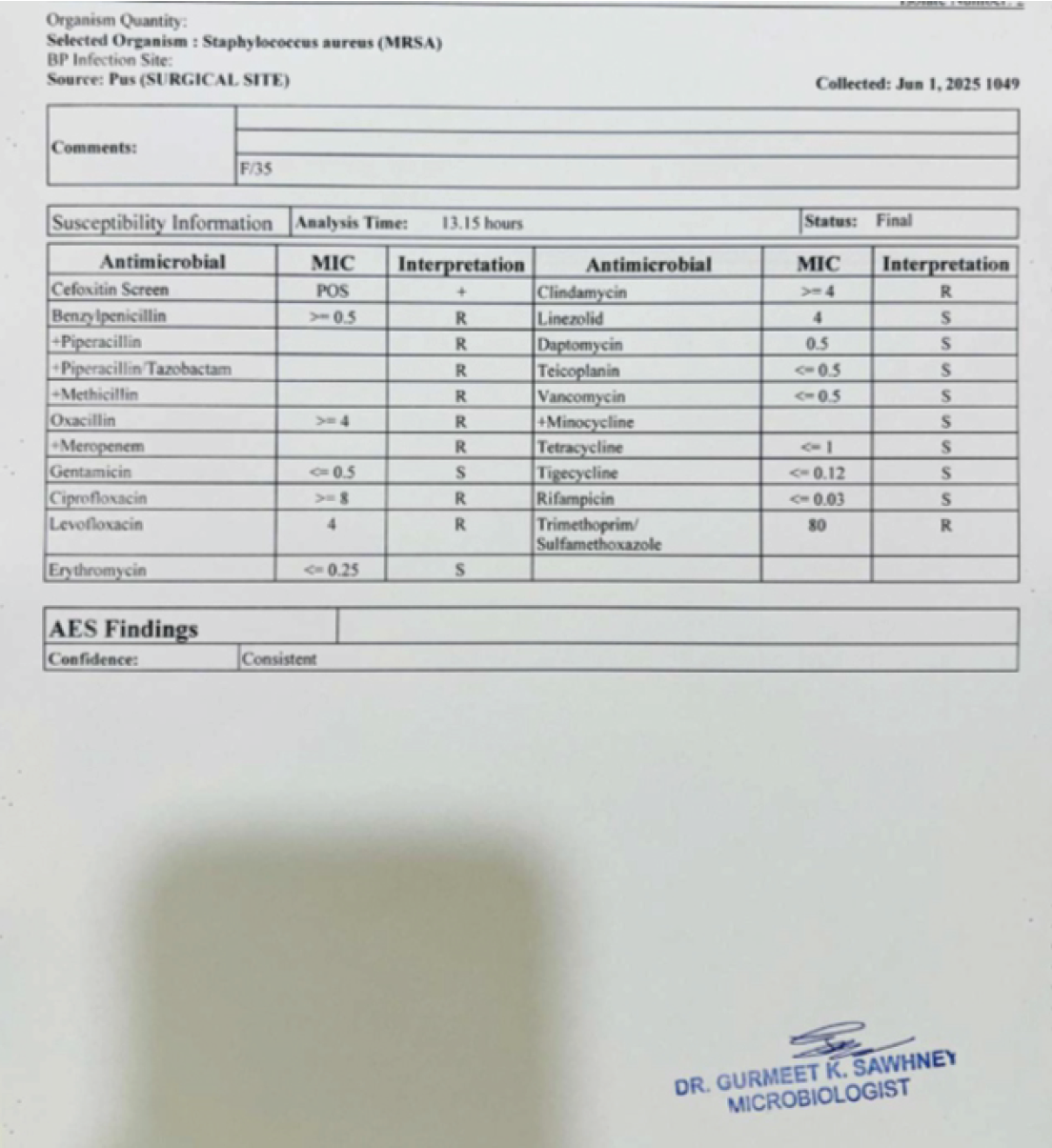
Figure 8: Culture report from the intramuscular collection at the time of incision and drainage shows the same Methicillin-resistant Staphylococcus aureus (MRSA) organism isolated from the synovial fluid. After the incision and drainage, patient’s condition improved rapidly. VITEK-2 identification and antimicrobial susceptibility profile of S. aureus (MRSA) isolate from intramuscular pus showing resistance to methicillin and sensitivity to vancomycin and linezolid.
MRI findings:
- Moderate right knee effusion
- Edema of vastus lateralis, medialis, and gastrocnemius
- Diagnosis: Septic arthritis with surrounding myositis.
Management and course:
- Diagnostic aspiration: Purulent fluid
- Gram stain: Gram-positive cocci
- Culture: MRSA
- Initial antibiotic: IV piperacillin-tazobactam, escalated to IV vancomycin post-sensitivity.
Despite initial improvement, CRP plateaued. Repeat ultrasound showed a growing collection in the medial gastrocnemius in spite of giving antibiotics as per sensitivity. Surgical incision and drainage were performed. Necrotic tissue was debrided. Pus culture again confirmed MRSA.
Post-operative care:
- CRP declined steadily
- Switched to oral linezolid after 2 weeks of IV vancomycin
- Wound managed with regular dressings
- At 4-week follow-up, the patient had full knee mobility with no signs of recurrence.
Literature review:
Pyomyositis, originally regarded as a tropical disease, is now being increasingly reported in temperate regions and among varied populations. It is traditionally associated with immunocompromised states – particularly HIV/AIDS, diabetes mellitus, malignancies, or corticosteroid use. A review by Crum [1] (2008) noted that over 90% of adult pyomyositis cases occurred in patients with identifiable immune compromise. However, reports in immunocompetent individuals remain rare. Paediatric series by Chauhan et al. [2] and a small number of adult case reports have described pyomyositis in otherwise healthy individuals, but often with atypical locations or delayed presentation. Recent case series by Shukla et al. [10] also highlight similar atypical presentations in immunocompetent patients, supporting our findings. In addition, literature often emphasises delayed diagnosis, with symptoms evolving over 1–3 weeks before imaging or intervention is performed. This delay is often due to vague initial symptoms or deep muscle involvement not easily visible on examination. In contrast, our patient was immunocompetent and had no underlying systemic illness. The presence of knee joint swelling prompted early MRI, which revealed both the joint effusion and surrounding muscle oedema – enabling early diagnosis and timely management [3,4,7,8,9].
MRSA septic arthritis may present atypically in immunocompetent individuals. The absence of fever can mislead the diagnosis. While initial MRI showed only myositis, progression to abscess necessitated close monitoring with inflammatory markers and imaging. Serial CRP and ultrasound helped guide timely surgical intervention. Targeted antimicrobial therapy and aggressive wound care contributed to a successful outcome. In contrast, our case demonstrates that early imaging combined with CRP monitoring can enable timely intervention. The plateau in CRP was a key indicator prompting repeat imaging. Although pyomyositis may coexist with septic arthritis, such concurrent presentations remain uncommon [3]. Our case is distinct in demonstrating both conditions without systemic symptoms. Recent case series by Shukla et al. [10] also highlight similar atypical presentations in immunocompetent patients, supporting our findings An important aspect of this case was the use of interdisciplinary collaboration facilitated through a digital medium. Upon diagnosis, a dedicated WhatsApp group was created involving the orthopaedic team, microbiologist, general surgeon, and infectious disease specialist. This real-time communication channel allowed all involved clinicians to remain updated, share inputs promptly, and make joint decisions regarding antibiotic escalation, the need for surgical intervention, and discharge planning. This approach not only enhanced clinical coordination but also reduced delays in care, especially in the evolving phase of the patient’s condition. It underscores the growing value of digital communication platforms in streamlining multidisciplinary care, particularly in acute infections where timely action is critical.
Clinicians should consider evolving pyomyositis in septic arthritis cases with persistent inflammatory markers or atypical imaging findings. Early culture-guided antibiotics, close surveillance, and surgical drainage when needed are crucial for recovery.
In patients with septic arthritis and persistent inflammation or atypical imaging findings, pyomyositis should be considered – even in immunocompetent individuals. Early MRI and serial inflammatory markers are key to timely diagnosis and intervention. Targeted antibiotic therapy may not be enough, and surgical evacuation of the abscesses may be required in addition to IV antibiotics.
References
- 1. Crum NF. Bacterial pyomyositis in the United States. Am J Med 2008;121:486-91. [Google Scholar] [PubMed]
- 2. Chauhan S, Jain S, Varma S, Chauhan SS. Tropical pyomyositis (myositis tropicans): Current perspective. Postgrad Med J 2004;80:267-70. [Google Scholar] [PubMed]
- 3. Gubbay AJ, Isaacs D. Pyomyositis in children. Pediatr Infect Dis J 2000;19:1009-12; quiz 1013. [Google Scholar] [PubMed]
- 4. King RJ, Laugharne D, Kerslake RW. Pyomyositis – a tropical disease in a temperate climate. Ann R Coll Surg Engl 2003;85:333-4. [Google Scholar] [PubMed]
- 5. Menezes GA, Harish BN, Sujatha S, Vinothini K, Parija SC. MRSA in India: Prevalence & susceptibility pattern. Indian J Med Res 2008;127:212-5. [Google Scholar] [PubMed]
- 6. Mathews CJ, Weston VC, Jones A, Field M, Coakley G. Bacterial septic arthritis in adults. Lancet 2010;375:846-55. [Google Scholar] [PubMed]
- 7. Lee YJ, Sadigh S, Mankad K, Kapse N, Rajeswaran G. The imaging of pyomyositis: A pictorial review. Insights Imaging 2018;9:753-62. [Google Scholar] [PubMed]
- 8. Kumar N, Menon A, Gopinathan NR. Pyomyositis of the lower limb muscles: clinical features and management of 40 cases in a tertiary care centre. Indian J Orthop 2014;48:297-302. [Google Scholar] [PubMed]
- 9. Mehta Y, Gupta A. Role of digital tools like WhatsApp in multidisciplinary clinical decision-making: boon or risk? Indian J Crit Care Med 2019;23:333-4. [Google Scholar] [PubMed]
- 10. Shukla RV, Dubey IP, Kumar A, Kompella K, Khan S, Mohanan K, et al. Tropical pyomyositis in immunocompetent hosts posing diagnostic challenges: A case series. J Mar Med Soc 2024;26:127-31. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2025 Primary Pyogenic Abscess in an Immunocompetent Child: An Indian Perspective
February 1, 2025 Primary Pyogenic Abscess in an Immunocompetent Child: An Indian Perspective August 6, 2024 Neonatal Septic Arthritis with Acyanotic CHD: A Case Study
August 6, 2024 Neonatal Septic Arthritis with Acyanotic CHD: A Case Study March 10, 2023 Bilateral Knee Septic Arthritis after Prostatic Urethral Lift: A Case Report
March 10, 2023 Bilateral Knee Septic Arthritis after Prostatic Urethral Lift: A Case Report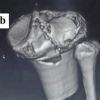 August 1, 2026 Bicruciate Ligament Avulsions, Lateral Meniscus Dual Root Avulsions – “Tibial Avulsion Tetrad” – with Menisco-capsular Injury – Floating Meniscus in Innocuous Looking Proximal Tibia Fracture
August 1, 2026 Bicruciate Ligament Avulsions, Lateral Meniscus Dual Root Avulsions – “Tibial Avulsion Tetrad” – with Menisco-capsular Injury – Floating Meniscus in Innocuous Looking Proximal Tibia Fracture