
Isolated distal radioulnar joint dislocation is a rare injury which requires thorough clinical examination and true anteroposterior and lateral radiographic imaging to correctly diagnose and manage to avoid long-term complication.
Dr. Stephen Murphy, Department of Trauma and Orthopaedics, Cork University Hospital, Whilton, Cork, T12 DC4A, Ireland. E-mail: sfmurphy101@gmail.com
Abstract
Introduction: Isolated distal radioulnar joint (DRUJ) dislocation is a rare injury, often presenting following direct trauma with difficulty in active and passive pronation/supination. Accurate and prompt diagnosis is to essential to correctly treat and avoid long-term complications such as pain, stiffness, and loss of function.
Case Report: We present the case of a 16-year-old male with an acute isolated DRUJ dislocation following a sporting injury. The patient was referred to our major trauma center from a tertiary orthopaedic unit following failed closed reduction (CR). Successful CR was performed in our department. Temporary casting and early rehab with physiotherapy gave the patient good functional results with full recovery at 3 months.
Conclusion: Careful history and examination, as well as appropriate imaging, including true anterioposterior and lateral radiographs +/− computed tomography or magnetic resonance imaging, is need to accurately diagnosis this injury. Consider this injury in a patient with difficulty in supination/pronation with reported wrist pain following trauma.
Keywords: Isolated distal radioulnar joint dislocation, trauma, pronation/supination, closed reduction.
Distal radioulnar joint (DRUJ) injuries are rare and are more commonly seen with associated distal radius and or ulnar fracture [1,2]. Galeazzi described one such fracture pattern in the radial diaphysis with associated DRUJ dislocation which now bears his name [3]. While DRUJ dislocation with associated fractures is more clinically and radiologically obvious, isolated DRUJ injuries are commonly misdiagnosed and hence incorrectly managed, which can lead to long-term pain and reduced functionality [4,5]. Treatment of isolated DRUJ dislocations generally involves closed reduction (CR) and casting, however, if CR fails, open reduction may be necessary, with or without stabilization with Kirschner wire (K wire) or soft-tissue repair [6]. We aim to describe the case of a young boy referred to our tertiary orthopedic unit with an irreducible DRUJ dislocation.
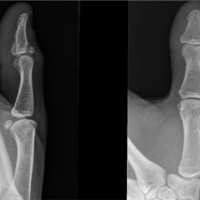
We present the case of a 16-year-old male who suffered a hypersupination injury while playing rugby. He attended his local orthopedic center where he reported pain and limited movement in his right wrist. On examination, he had swelling and diffuse tenderness of his right wrist, with restricted supination and pronation. Examination of his ipsilateral elbow and shoulder was normal and he was neurovascularly intact. Initial plain film radiographs of his right wrist showed a volar dislocation of the right distal radioulnar joint with associated ulnar styloid fracture (Fig. 1). CR was attempted at the time but failed (Fig. 2). He was then referred to our tertiary orthopedic unit.

On arrival to our unit, he underwent computed tomography (CT) scan before the theater (Fig. 3). He subsequently underwent CR under general anaesthetic (Fig. 4). An above elbow (AE) cast was applied postoperatively. He was seen 4 weeks postoperatively in an outpatient’s clinic. He had no tenderness on the exam and was placed into a futura splint. Subsequent radiographs were all in the joint. He was referred to physiotherapy to commence a range of motion exercises and to wean from his splint over the following 2 weeks. He had returned to normal function at 3 months post-injury. His DASH score at 41 at 11 months.

Systematic review
A literature review on PubMed was undertaken to find all case reports investigating DRUJ dislocations. The following Boolean terms “isolated DRUJ dislocation’ or DRUJ dislocation with ulnar styloid fracture” or “isolated DRUJ subluxation” were used in this search. The year of publication was set from 1983 to 2024. Case reports of isolated DRUJ dislocation were included. Any case reports investigating DRUJ injury with associated distal or proximal radius or ulnar fracture were excluded as well as papers reporting on both DRUJ and proximal radioulnar joint (PRUJ) injuries. Papers published in English and with full text available were included in the study. A total of 78 papers were found. After duplication and abstract screening, 63 papers were removed, leaving a total of 15 papers for inclusion (Table 1).

A summary of included papers is shown below (Table 2). Average age was 34 years (range 12–58 years). Males accounted for 87% (n = 13). There was one case of recurrent dislocation, both incidents being dorsal dislocations [7]. Hence, a total of 16 isolated DRUJ dislocations were examined.

Dorsal dislocations were seen in 31% (n = 5) and volar in 69% (n = 11). 25% (n = 4) had some delay in diagnosis, ranging from 1 day to 8 weeks [8-11].
The history of presenting complaints varied among the 16 dislocations analyzed. The most commonly seen cause was a fall on the out-stretched hand injury, documented in 43% of cases (n = 7). Other causes included direct trauma to the wrist, road traffic accidents, and crush injuries. All cases reported some form of limited pronation/supination on examination. CR in the emergency department (ED) was attempted and failed in 6 of the total 16 dislocations (37.5%). CR only, either in the ED or in the operating room, was successful in 62.5% (n = 10). CR with K wire stabilization was done in 12.5% (n = 2) of cases. Open reduction was seen in 25% (n = 4) of cases, one of these also used K wires to stabilize the DRUJ [12]. Post-reduction regimen differed vastly among included cases. AE casting was specifically listed as initial splinting in 69% (n = 11) of cases. However, the duration of AE casting varied from 2 to 6 weeks. Three papers only mentioned that some form of splinting was applied but did not specified type of casting or whether this was AE or Below Elbow. A hinged elbow brace was used in one case [13] and sugar tong followed by muenster splints were use in another case [12]. 3 papers used K wires to stabilize the DRUJ. Both papers utilizing K wires with CR were removed at 6 weeks in 2 cases [14,15] while K wires used with open reduction were removed at 4 weeks [12]. 12 papers reported on time to return to normal range of movement. This varied greatly, from <1 week to 72 weeks.
The DRUJ is an important articulation between the radius and ulna which, along with the PRUJ and the interosseous membrane, functions to allow pronation and supination of the forearm [1,16]. The articular surface of the distal ulna sits within the sigmoid notch of the distal radius, forming this complex synovial joint. The rim of the sigmoid notch provides stability to the joint, reinforced with a complex ligamentous and muscular anatomy [1,17,18]. DRUJ dislocations and subluxations are typically described as volar or dorsal based on the ulnar position relative to the radius [4,17]. DRUJ dislocation is uncommon and when encounter, it is more commonly seen with distal radius fracture and is most often dorsal [1,2,18]. Isolated DRUJ injuries without distal radial or ulnar fracture are rare [19]. Isolated injuries may also be missed, with reports of misdiagnosis estimated at 36–50% [4,20,21]. True lateral radiographs of the wrist are essential to accurate diagnosis [4]. CT or magnetic resonance imaging (MRI) may be needed to further assess injuries of the wrist with restricted pronation/supination if radiographs are unclear [17]. As there are few cases of isolated injury, there is no strong evidence for optimal treatment, however, many are successfully treated with CR and a period of immobilization of forearm pronation/supination [4,6]. If CR is unsuccessful, higher-order imaging (CT or MRI) may be warranted to assess the anatomy to investigate if a mechanical block or soft-tissue injury is obstructing reducing. These injuries may need open reduction with soft tissue repair, depending on imaging results. The outcomes of this systematic review indicate a successful result in the majority of cases examined. Notably, the sole patient who reported long-term limitations in range of motion and decreased grip strength was one who presented 8 weeks post-injury due to an initial misdiagnosis [9]. This underscores the critical importance of accurate diagnosis at the time of presentation. Fortunately, the other two cases of initially misdiagnosed DRUJ dislocations were promptly identified — within one and 2 days, respectively — and managed appropriately [8,10].
Isolated DRUJ injuries are rare injuries. Prompt diagnosis and treatment are important to restore function and avoid long-term complications such as pain and stiffness. Interestingly, this study found a large proportion of patients with acute difficulty in pronation/supination following their injury, which is unusual in wrist injuries. This highlights the importance of thorough physical examination in all patients presenting with a musculoskeletal injury. Abnormal findings should trigger appropriate investigation with imaging of the entire forearm. This case report describes successful treatment with CR in theatre and good functional outcomes after an isolated DRUJ injury.
Isolated DRUJ injuries are rare, however, a low index of suspicion should be adopted for these injuries’ in patients with limited pronation/supination post-wrist injury. A thorough examination is, therefore, required along with true AP and lateral wrist radiographs to avoid missing this injury which can potentially lead to worse functional outcomes.
References
- 1.Adams BD. Distal Radioulnar Joint Instability Hand Surgery. Philadelphia, PA: Lippincott Williams and Wilkins; 2004. p. 337-54. [Google Scholar | PubMed]
- 2.Geissler WB, Fernandez DL, Lamey DM. Distal radioulnar joint injuries associated with fractures of the distal radius. Clin Orthop Relat Res 1996;327:135-46. [Google Scholar | PubMed]
- 3.Giannoulis FS, Sotereanos DG. Galeazzi fractures and dislocations. Hand Clin 2007;23:153-63. [Google Scholar | PubMed]
- 4.O’malley O, Brown OC, Duncan L, Cheung G, Stevenson HL, Brown DJ. Isolated volar dislocation of the distal radioulnar joint: A case series and systematic review. Ann R Coll Surg Engl 2023;105:196-202. [Google Scholar | PubMed]
- 5.Rainey RK, Pfautsch ML. Traumatic volar dislocation of the distal radioulnar joint. Orthopedics 1985;8:896-900. [Google Scholar | PubMed]
- 6.Ellanti P, Grieve PP. Acute irreducible isolated anterior distal radioulnar joint dislocation. J Hand Surg Eur Vol 2012;37:72-5. [Google Scholar | PubMed]
- 7.Wassink S, Lisowski LA, Schutte BG. Traumatic recurrent distal radioulnar joint dislocation: A case report. Strategies Trauma Limb Reconstr 2009;4:141-3. [Google Scholar | PubMed]
- 8.Köroglu M, Özdeş HU, Taşkıran G, Aslantürk O. Acute isolated volar distal radioulnar joint dislocation: First surgery or conservative? Trauma Case Rep 2023;48:100952. [Google Scholar | PubMed]
- 9.Li Y, Yan H. Isolated irreducible chronic volar dislocation of the distal radioulnar joint: A case report. JBJS Case Connect 2014;4:e119. [Google Scholar | PubMed]
- 10.Takami H, Takahashi S, Ando M. Isolated palmar dislocation of the distal radioulnar joint in a football player. Arch Orthop Trauma Surg 2000;120:598-600. [Google Scholar | PubMed]
- 11.Mittal R, Kulkarni R, Subsposh SY, Giannoudis PV. Isolated volar dislocation of distal radioulnar joint: How easy to miss. Eur J Emerg Med 2004;11:113-6. [Google Scholar | PubMed]
- 12.Garrigues GE, Aldridge JM 3rd. Acute irreducible distal radioulnar joint dislocation. A case report. J Bone Joint Surg Am 2007;89:1594-7. [Google Scholar | PubMed]
- 13.Tang CY, Cheung JP, Fung B. A rare combination: Locked volar distal radio-ulnar joint dislocation with isolated volar capsule rupture. Hand Surg 2014;19:413-7. [Google Scholar | PubMed]
- 14.Daradkeh ST, Elayan B, Daradkeh YT, Al Dabouby FS. Case report: Isolated acute dorsal distal radioulnar joint (DRUJ) dislocation. Int J Surg Case Rep 2022;95:107190. [Google Scholar | PubMed]
- 15.Haouzi MA, Bassir RA, Boufettal M, Kharmaz M, Lamrani MO, Mahfoud M, et al. Isolated dorsal dislocation of the distal radioulnar joint: A case report. Trauma Case Rep 2020;29:100349. [Google Scholar | PubMed]
- 16.Zimmerman RM, Jupiter JB. Instability of the distal radioulnar joint. J Hand Surg Eur Vol 2014;39:727-38. [Google Scholar | PubMed]
- 17.Szabo RM. Distal radioulnar joint instability. J Bone Joint Surg Am 2006;88:884-94. [Google Scholar | PubMed]
- 18.Tsai PC, Paksima N. The distal radioulnar joint. Bull NYU Hosp Jt Dis 2009;67:90-6. [Google Scholar | PubMed]
- 19.Lichtman DM, Joshi A. Acute injuries of the distal radioulnar joint and triangular fibrocartilage complex. Instr Course Lect 2003;52:175-83. [Google Scholar | PubMed]
- 20.Weseley MS, Barenfeld PA, Bruno J. Volar dislocation distal radioulnar joint. J Trauma 1972;12:1083-8. [Google Scholar | PubMed]
- 21.Dukan R, Hassan SK, Delvaque JG, Khaled I, Nizard R. Isolated volar dislocation of the distal radioulnar joint: A case report. J Orthop Case Rep 2020;10:97-100. [Google Scholar | PubMed]
- 22.Petitto A, Minicelli MG. Isolated acute dorsal distal radioulnar joint dislocation: A case report. J Orthop Case Rep 2023;13:133-6. [Google Scholar | PubMed]
- 23.Glazier MT, Schuette HB, Schnee BA, Skura B, Goubeaux C. Isolated volar dislocation of the distal radioulnar joint treated with successful closed reduction. Cureus 2021;13:e15656. [Google Scholar | PubMed]
- 24.Bouri F, Fuad M, Abdolenour AE. Locked volar distal radioulnar joint dislocation. Int J Surg Case Rep 2016;22:12-4. [Google Scholar | PubMed]
- 25.Israelyan A, Chiang J, Cooper KC, Lew VL, Murphey GC, Durant E. Isolated volar radioulnar joint dislocation with associated ulnar styloid fracture. Cureus 2024;16:e61977. [Google Scholar | PubMed]
- 26.Werthel JD, Masmejean E, Silvera J, Boyer P, Schlur C. Acute isolated volar dislocation of the distal radio-ulnar joint: Case report and literature review. Chir Main 2014;33:364-9. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2021 Management for Bony Mallet Thumb with a Single Extension Blocking Kirschner Wire
May 10, 2021 Management for Bony Mallet Thumb with a Single Extension Blocking Kirschner Wire August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report
August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report August 1, 2026 Volar Carpometacarpal Dislocation Associated with Fracture of the Second, Third, and Fourth Metacarpal Bases Treated by Closed Reduction and Percutaneous Fixation: A Case Report
August 1, 2026 Volar Carpometacarpal Dislocation Associated with Fracture of the Second, Third, and Fourth Metacarpal Bases Treated by Closed Reduction and Percutaneous Fixation: A Case Report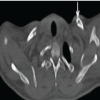 July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report
July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report