
Meticulous preoperative planning, including advanced imaging and identifying the cause of prior failure, is paramount for successful complex revision total hip arthroplasty, often necessitating patient-specific approaches and techniques like the use of metal augments for significant bone loss.
Dr. Shivam Chauhan, Department of Orthopaedic Surgery, All India Institute of Medical Sciences, Raipur - 492099, Chhattisgarh, India. E-mail: chauhanshivam9555@gmail.com
Abstract
Introduction: Revision arthroplasty is challenging, especially in severe acetabular bone loss cases. Metal augments have emerged as a viable option for managing such complex defects.
Case Report: We report a case of a 59-year-old male who underwent re-revision arthroplasty using a metal augment for severe acetabular bone loss, restoring limb length and anatomical hip center following a failed revision total hip arthroplasty in a case of neglected inferior hip dislocation. The patient presented with significant pain, instability, and limited mobility. Postoperative outcomes showed considerable improvement, with a Harris Hip Score increasing from 37 to 82 at the 12-month follow-up.
Conclusion: In conclusion, this case report demonstrates the effectiveness of metal augments in revision arthroplasty for managing significant bone loss. Careful patient selection and expert surgical techniques can provide a reliable solution for ensuring stable fixation and improving clinical outcomes in complex revision surgeries.
Keywords: Total hip arthroplasty, revision, metal augment
Revision arthroplasty surgeries are becoming more common due to the global prevalence of total hip arthroplasty (THA), one of the most successful orthopedic procedures [1,2]. Revision hip arthroplasty frequently involves issues such as acetabular defects and insufficient bone mass. Various surgical procedures have been used, such as structural bone grafts, anti-protrusion cages, cup-cage constructs, strengthening rings (reinforced cages and rings), jumbo cups, and custom tri-flange acetabular components. Nevertheless, these methods have drawbacks, including poor bone supply, resorption of bone grafts, high rates of loosening, and mechanical fixation failure. In the case of complex acetabular revision, porous trabecular metal acetabular components in conjunction with metal augments are considered promising treatment options [3-10] Porous metal’s qualities enable superior primary structural stability and later secondary biologically integrated fixation [11-13]. Compared to an uncemented hemispherical cup alone, trabecular titanium augments combined with uncemented porous-coated cups have produced superior outcomes in high grades of acetabular bone loss [12,14]. We share our experience of treating failed revision arthroplasty secondary to total hip replacement for hip arthritis in a case of inferior hip dislocation with metal augment and hemispherical cup for acetabular defect along with long diaphyseal fixation stem. Patient’s consent has been obtained for the submission of this case report.
A 59-year-old male presented to our institute’s outpatient department in the year 2023 with complaints of pain in the right hip, instability, and limited adduction. The patient had already surgery of revision THA elsewhere (Fig. 1).

The patient had a history of neglected hip dislocation due to a fall from a height 20 years back. This led to pain, and he underwent THA 18 years later. The patient’s previous radiographs (Fig. 2) and computed tomography (CT) (Fig. 3 and 4) showed inferior hip dislocation (obturator type), with the femoral head lying in a false acetabulum within the ischium bone. The femoral head collapsed, with multiple osteophytes around the false acetabulum. The true acetabulum was nearly half destroyed from below, with soft-tissue mass present within the remaining superior part of the true acetabulum, visible on MRI (Fig. 5 and 6).


According to the patient, even after a month of primary total hip replacement (Fig. 7), the patient continued to have pain and instability. Due to consistent complaints, the patient underwent revision arthroplasty with a change of the acetabular component and replacing the femoral stem with a diaphyseal fixation stem (Fig. 8).

After 1 year of revision arthroplasty, the patient presented to us with complaints of pain in bearing weight, instability, and limited adduction of the right hip. On examination, the patient had a painful hip and decreased range of motion in all directions. Diffuse atrophy of muscles was present around the right hip. The patient had a limb length discrepancy of 4.5 cm. The patient’s Harris Hip Score (HHS) was 37. The patient’s complaints were mainly thought to be due to the high hip center and decreased vertical and horizontal offset. The femoral stem was not well seated up to the calcar. The greater trochanter was high riding and also the lesser trochanter was abutting the ischial bone, making the hip unstable. Hence, it was decided to go for a second revision and restore the high hip center and offset to their anatomical location along with limb length discrepancy (Fig. 9).
Surgical technique
The posterior southern Moore’s approach was used for revision. Myositis ossification mass was removed along abductors. The previous stem was found to be loose; hence, it came out easily. Acetabular cup screws were removed, and the cup was found to be well-fixed. Using curved osteotomes, the cup was removed. Fibrous tissue was curetted out of the femoral canal, and a wound wash was given. Intra-op soft tissue samples were sent for cultures. A hip center was located using fluoroscopy and visualizing teardrops. Acetabular reaming was done, and the superolateral defect was found to be Paprosky type 2B. A hemispherical 50 mm multi-hole acetabular shell (Gription, Depuy Synthes) was fixed with three cancellous bone screws 6.5 × 20 mm, 6.5 × 30 mm, and 6.5 × 35 mm, revision metal augment 50/52 × 10 mm (Pinnacle Gription TF, Depuy Synthes) was fixed into the defect with cement between the shell and augment. Augment was locked with two locking screws, 5 × 30 mm and 5 × 35 mm (Fig. 10). Long diaphyseal fixation stem 10” × 15.0 mm right bowed 12/14 taper (Solution system hip stem with Porocoat, Depuy Synthes) was then placed into femoral canal with 28 mm femoral head + 8.5 12/14 taper (Articuleze, Depuy Synthes) and Constrained Liner + 4 neutral 28 mm ID/50 mm OD (Pinnacle GVF polyethylene acetabular liner, Depuy Synthes). The hip was then reduced and was stable through the range of motion. The wound was closed in layers.

Follow-up and outcome
The patient was discharged on postoperative day 5 and followed up at regular intervals, with suture removal done at 2 weeks postoperatively. The postoperative period was uneventful. Partial weight-bearing mobilization with a walker was started immediately postoperatively, along with hip strengthening exercises and full weight bearing from the 2nd week postoperatively. At 3-month follow-up, the patient’s hip and thigh pain complaints reduced significantly. HHS improved to 69. Radiographs were satisfactory, showing well-fixed acetabulum and good diaphyseal fixation of the stem (Fig. 11a). The patient used the cane on the left side for longer walks and had a moderate limp.

At 12 months of follow-up, the patient’s HHS was 82. He could bear weight, walk pain-free without support, and use a cane for only long walks. Radiographs showed no signs of loosening on either side or subsidence of the stem (Fig. 11b). The patient had remaining LLD of 1 cm (earlier 4.5 cm) and a satisfactory range of motion at the hip joint (flexion 0–70°; abduction 0–45°; adduction 0–30°; Internal Rotation 0–30°; External Rotation 0–50°); and knee joint (flexion 0–100°) (Fig. 12).

This case report highlights the successful management of a complex re-revision THA using a metal augment for significant acetabular bone loss following a neglected inferior hip dislocation and multiple prior failed revisions. The patient presented with significant pain, instability, and limited mobility, severely impacting their quality of life. The marked improvement in the patient’s HHS from 37 preoperatively to 82 at the 12-month follow-up demonstrates the effectiveness of this approach. A Systemic review of 19 studies on trabecular metal augments in revision arthroplasty reported a significant improvement in clinical outcomes, with a mean HHS increase of 44 points [15].
Tips and tricks
Several key intraoperative strategies contributed to the positive outcome in this challenging case. Meticulous dissection was essential to navigate the altered anatomy and manage scar tissue and potential heterotopic ossification from previous surgeries. Careful component removal, using flexible curved osteotomes to minimize further bone loss, was crucial, as was thorough debridement of the acetabulum to prepare for augment placement. Accurate assessment of the bone defect using CT and the Paprosky classification guided the selection of an appropriately sized metal augment. The use of metal augments minimized the risk of complications associated with bone grafting, such as graft resorption and nonunion. As the transverse acetabular ligament was not identified due to previous surgeries, an inferior retractor was placed at the superior border of the obturator foramen to guide proper implant placement. Restoring the hip center and offset was a critical objective, achieved through careful implant positioning. Dual mobility cups or constrained liners are beneficial in revision surgeries due to the high risk of dislocation, and consideration was given to a constrained liner to address the damaged abductors. Finally, addressing soft-tissue imbalances, including the removal of myositis ossificans, contributed to improved function and range of motion.
Algorithm for complex revision THA
This protocol outlines the management of complex revision THA utilizing metal augments for substantial bone loss. Preoperative planning is crucial and includes a thorough patient history, detailing prior surgeries, implants, complications, the initial injury, revision timeline, and current symptoms. A comprehensive clinical examination assesses pain, range of motion, gait, leg length discrepancy, and soft tissue and neurovascular status. Imaging modalities play a vital role, with radiographs evaluating the existing implant and bone stock, CT scans providing detailed information on bone loss (Paprosky classification), implant fixation, and augment planning, and MRI assessing soft tissues and potential masses. This information guides the development of a personalized surgical plan, encompassing implant selection, surgical approach, cementing techniques, trial reduction, and contingency plans. Intraoperatively, the procedure begins with careful exposure, including dissection, neurovascular protection, and management of scar tissue and ossification. Component removal focuses on minimizing further bone loss and includes debridement and obtaining cultures if indicated. Acetabular reconstruction involves meticulous defect assessment and secure fixation of the augment and shell. Stem implantation follows careful canal preparation and placement to achieve appropriate leg length and offset. Trial reduction assesses stability, range of motion, and impingement, with consideration of a constrained liner if necessary. Soft-tissue balancing addresses contractures and imbalances. Closure concludes the intraoperative phase. Postoperatively, immediate care focuses on pain control and early mobilization. A structured rehabilitation program guides progressive recovery. Regular follow-up appointments monitor progress, fixation, outcomes, and radiographic findings. Long-term monitoring is essential to detect potential loosening, subsidence, and other complications. This complex procedure necessitates a patient-specific, multidisciplinary approach with thorough documentation at each stage.
In conclusion, this case report demonstrates the effectiveness of metal augments in revision arthroplasty for managing significant bone loss. With careful patient selection, accurate preoperative planning, and expert surgical technique, metal augments can provide a reliable solution for restoring bone stock, ensuring stable fixation, and improving clinical outcomes in complex revision surgeries.
We need to consider all options, including Bone graft, custom-made implants, 3D printed implants, and metal augments, in addition to proper preoperative planning to get a stable hip and good outcome.
References
- 1.Varacallo MA, Herzog L, Toossi N, Johanson NA. Ten-Year trends and independent risk factors for unplanned readmission following elective total joint arthroplasty at a large urban academic hospital. J Arthroplasty 2017;32:1739-46. [Google Scholar | PubMed]
- 2.Varacallo M, Chakravarty R, Denehy K, Star A. Joint perception and patient perceived satisfaction after total hip and knee arthroplasty in the American population. J Orthop 2018;15:495-9. [Google Scholar | PubMed]
- 3.Schelfaut S, Cool S, Mulier M. The use of structural periacetabular allografts in acetabular revision surgery: 2.5-5 years follow-up. Arch Orthop Trauma Surg 2009;129:455-61. [Google Scholar | PubMed]
- 4.Beckmann NA, Weiss S, Klotz MC, Gondan M, Jaeger S, Bitsch RG. Loosening after acetabular revision: Comparison of trabecular metal and reinforcement rings. A systematic review. J Arthroplasty 2014;29:229-35. [Google Scholar | PubMed]
- 5.Baauw M, Van Hooff ML, Spruit M. Current construct options for revision of large acetabular defects: A systematic review. JBJS Rev 2016;4:e2. [Google Scholar | PubMed]
- 6.Barlow BT, Oi KK, Lee YY, Carli AV, Choi DS, Bostrom MP. Outcomes of custom flange acetabular components in revision total hip arthroplasty and predictors of failure. J Arthroplasty 2016;31:1057-64. [Google Scholar | PubMed]
- 7.Sculco PK, Ledford CK, Hanssen AD, Abdel MP, Lewallen DG. The evolution of the cup-cage technique for major acetabular defects: Full and half cup-cage reconstruction. J Bone Joint Surg Am 2017;99:1104-10. [Google Scholar | PubMed]
- 8.De Martino I, Strigelli V, Cacciola G, Gu A, Bostrom MP, Sculco PK. Survivorship and clinical outcomes of custom triflange acetabular components in revision total hip arthroplasty: A systematic review. J Arthroplasty 2019;34:2511-8. [Google Scholar | PubMed]
- 9.Volpin A, Konan S, Biz C, Tansey RJ, Haddad FS. Reconstruction of failed acetabular component in the presence of severe acetabular bone loss: A systematic review. Musculoskelet Surg 2019;103:1-13. [Google Scholar | PubMed]
- 10.Wang CX, Huang ZD, Wu BJ, Li WB, Fang XY, Zhang WM. Cup-cage solution for massive acetabular defects: A systematic review and meta-analysis. Orthop Surg 2020;12:701-7. [Google Scholar | PubMed]
- 11.Fryhofer GW, Ramesh S, Sheth NP. Acetabular reconstruction in revision total hip arthroplasty. J Clin Orthop Trauma 2020;11:22-8. [Google Scholar | PubMed]
- 12.Bobyn JD, Stackpool GJ, Hacking SA, Tanzer M, Krygier JJ. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J Bone Joint Surg Br 1999;81:907-14. [Google Scholar | PubMed]
- 13.Meneghini RM, Meyer C, Buckley CA, Hanssen AD, Lewallen DG. Mechanical stability of novel highly porous metal acetabular components in revision total hip arthroplasty. J Arthroplasty 2010;25:337-41. [Google Scholar | PubMed]
- 14.Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J Arthroplasty 1994;9:33-44. [Google Scholar | PubMed]
- 15.Xiong C, Meng D, Ni R, Cai H. Metal augments used in revision hip arthroplasty: A systematic review and single-arm meta-analysis. J Arthroplasty 2023;38:389-96.e1. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report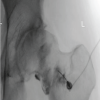 August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report
August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report