
Intramedullary fibular nailing provides a safe, minimally invasive, and effective alternative to traditional plating in the management of complex comminuted Weber C ankle fractures, particularly in elderly patients with significant comorbidities.
Dr. Ajith Kumar Kannan, Department of Health Informatics, Rutgers - School of Health Professions, 675 Hoes Lane West, Piscataway, NJ 08854, E-mail: ak2442@scarletmail.rutgers.edu
Introduction: Ankle fractures are among the most common lower extremity injuries, accounting for approximately 9% of all fractures. Various methods exist for the internal fixation of fibular fractures, with open reduction and internal fixation using plates and screws currently regarded as the gold standard. However, plate and screw fixation is highly invasive and may lead to significant post-operative complications. Intramedullary (IM) nails, offering a less invasive alternative, have conventionally been indicated for non-comminuted Weber B and C fractures. To our knowledge, this is one of the few reports in the literature demonstrating the successful application of IM nails in a comminuted Weber C fracture.
Case Report: We describe an 80-year-old female of Caucasian descent who presented with a comminuted Weber C ankle fracture following a fall. The patient was treated with fibular nail fixation, a minimally invasive technique that achieved successful alignment and stabilization. The patient had an uneventful recovery with no post-operative complications, highlighting the potential of this method in managing complex fractures in elderly patients with comorbidities.
Conclusion: This case underscores the versatility and efficacy of IM nails in treating complex fibular fractures, including comminuted Weber C fractures. It highlights the clinical relevance of this technique as a less invasive and complication-reducing alternative to traditional plating systems, particularly for elderly patients with high surgical risks. The findings suggest that IM fixation has the potential to significantly advance fracture management strategies and reduce associated morbidity.
Keywords: Ankle fracture, intramedullary nails, Weber C fracture, fibular fixation, Fibulock, minimally invasive surgery.
Ankle injuries encompass a wide range of conditions, with some being more common, such as lateral malleolus fractures, medial malleolus fractures, and bimalleolar fractures, and others less frequently encountered, such as trimalleolar fractures and pilon fractures [1]. In addition, combinations of these injuries have been documented, including the coexistence of lateral and medial malleolus fractures, as well as the “ankle triad,” comprising fractures of the lateral malleolus, medial malleolus, and posterior malleolus [2]. While surgical outcomes following open reduction and internal fixation (ORIF) are generally favorable in restoring ankle joint stability, complication rates as high as 40% have been reported in the literature [3,4]. Factors such as pre-existing comorbidities, post-operative wound healing complications, and periprosthetic fractures significantly prolong recovery time and increase the financial burden on both patients and health-care systems. In addition, reoperation rates for ankle fractures remain substantial, varying by fracture type: 11% for Weber A, 37.8% for Weber B, and 51.2% for Weber C fractures [4]. This study delves into the unique challenges of managing ankle fractures in elderly patients, with a focus on the impact of factors such as reduced bone density, comorbidities, and limited mobility, which complicate treatment decisions. To underscore the clinical relevance of alternative surgical techniques, we present the case of an 80-year-old female with an ankle fracture successfully treated with fibular rod fixation. This case highlights the efficacy of fibular rods in managing complex ankle fractures and provides valuable insights into their potential as a reliable and less invasive option in this patient population.
An 80-year-old female with a medical history of hypertension, chronic obstructive pulmonary disease, and two prior surgeries – a left ankle ORIF and a right total knee arthroplasty – presented to the Emergency Department with a right ankle injury following a mechanical fall. The patient reported an inability to bear weight on the right lower extremity since the fall. She denied any history of peripheral vascular disease, diabetes mellitus, or Vitamin D deficiency. On physical examination, there was ecchymosis and moderate soft-tissue swelling over the right ankle. Dorsalis pedis and posterior tibial pulses were palpable bilaterally. Neurological assessment revealed intact protective sensation bilaterally. Orthopedic examination showed no gross pedal deformities, but there was a limited range of motion in the right ankle due to pain. Tenderness was noted on palpation over the medial superior ankle, where moderate soft-tissue swelling and ecchymosis were observed (Fig. 1-3). An X-ray of the right ankle confirmed an oblique mildly displaced comminuted fracture of the distal right fibula (Fig. 4 and 5). 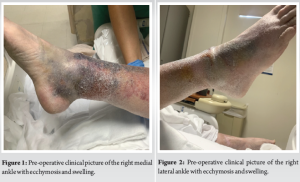

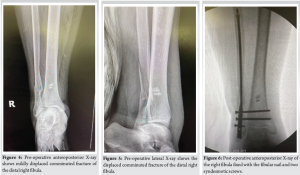
The patient underwent a comprehensive orthopedic surgical procedure to address a complex right ankle injury, specifically a trimalleolar equivalent ankle fracture with syndesmotic rupture. The procedure included ORIF of the fibula using the Fibulock Intramedullary (IM) Fixation system, butterfly fragment fixation utilizing FiberTape, and syndesmotic repair. The surgical approach involved anesthetic management with a laryngeal mask airway and a pre-operative popliteal block administered to the right lower extremity. The patient’s right lower extremity and foot were meticulously scrubbed, prepped, and draped using a standard aseptic technique. Fluoroscopy was employed throughout the procedure to confirm anatomical alignment, and the surgical site was thoroughly irrigated with normal saline. The procedure began with a 3 cm incision on the lateral aspect of the distal fibula, proximal to the fracture site. Using a combination of blunt and sharp dissection, the hematoma was irrigated with normal saline, and the fracture site was localized under fluoroscopy. Coagulated blood was removed, soft-tissue impingements were addressed, and a reduction clamp was applied to reapproximate the bone fragments. To further stabilize the fracture, an angled hemostat was used to place FiberTape around the fibula fracture, encircling the fibular shaft at the butterfly fragment. The cerclage suture tails were secured to provide tension to the FiberTape, and fragment apposition was confirmed under fluoroscopy. Next, attention was directed to the lateral aspect of the right ankle, where a longitudinal incision was made 1 cm distal to the fibula’s tip. Percutaneous reduction of the fibular fracture was achieved with appropriate alignment of the ankle joint and fracture reduction. A guidewire was advanced from the distal aspect of the fibula through the fracture site, followed by drilling the fibula with an IM drill. The diaphyseal canal was reamed, and a 3 × 130 mm fibular nail, assembled with a target guide, was inserted through the incision. The fibular nail facilitated the reduction of the ankle fracture, and two syndesmotic screws were applied within the fibular construct to enhance ankle stability and provide additional support to the posterior malleolus fragment (Fig. 6 and 7).

The subcutaneous layers and periosteum were closed using a combination of 2-0 and 3-0 Vicryl sutures. The skin incisions were then closed with 4-0 nylon using a Hemigard suture technique. The surgical site was dressed with Betadine, 4 × 4 dressings, and Kerlix, followed by the application of a well-padded posterior splint to the right lower extremity.
The patient tolerated the procedure well and was transferred from the operating room to the recovery area with stable vital signs and intact neurovascular status (Fig. 8-10).


The surgical intervention successfully stabilized the complex right ankle fracture. However, post-operative complications, including fracture blisters, were observed, requiring ongoing management and care. The patient achieved a successful recovery following the procedure, with no significant complications, and has since returned to normal activities with good functional outcomes. This case was selected for our study because it demonstrates that comminuted fibular fractures with butterfly fragments do not preclude the use of a fibular nail. Although fibular nails have traditionally been indicated for Weber B and C non-comminuted fractures, the integration of advanced cerclage systems enables us to explore and expand the indications for fibular rod or IM nail procedures. This case challenges conventional practices and underscores the potential to broaden the applicability and effectiveness of fibular nail interventions in managing complex fractures.
At present, the first-line treatment for unstable ankle fractures is ORIF. Common fixation methods include locking and tubular plates, typically steel or titanium, attached to the fibula with screws or fixation plates used on the tibia to stabilize the bones. However, wound complications remain a frequent issue with ORIF due to limited soft-tissue cover in the injured area, with additional risks of infection and hardware failure. These risks are heightened in elderly, immunocompromised patients, and those with comorbidities [1]. Consequently, minimally invasive techniques are gaining traction to mitigate periosteal damage and soft-tissue dissection. IM nailing, introduced through the ANK nail at the Vakif Gureba Teaching Hospital from 1990 to 1997 [5], has been studied extensively for distal fibula fractures, particularly in elderly and immunocompromised patients [6,7]. Several prospective studies report comparable outcomes between fibular nails and standard ORIF, with fibular nails demonstrating significantly reduced rates of wound breakdown compared to plating techniques [8-12]. These findings align with recent reviews on IM fibular nails, which document their effectiveness in reducing wound complications and improving overall patient outcomes, especially in adults with ankle fractures [13]. The distinction between IM nails and plates with screws lies in their stabilization mechanisms. While IM nails provide relative stability without compression across the fracture site, plates and screws offer compression and more rigid fixation. Despite this difference, IM rods, when accurately executed, are effective in maintaining length better than traditional plates and screws. Dynamized implants, which permit micromotion and progressive axial loading, have been shown to promote external callus formation and optimize healing over time [14]. Thus, selecting between these methods depends on fracture type, location, and the desired balance between stability and flexibility. IM fixation for fibular fractures does not significantly impact surgical time or quality of reduction when performed by experienced surgeons [11]. Studies suggest that although the initial implant cost for IM nailing may be higher, long-term costs – encompassing reduced dressing changes, outpatient consultations, and shorter hospital stays – make it a more economical choice. Given its low complication rates, minimally invasive nature, and financial viability, IM nailing is a compelling alternative for a wide range of patients. Fibular nails represent a pivotal advancement in orthopedic surgery, especially for complex comminuted fractures. These fractures are challenging due to extensive fragmentation and compromised stability. Fibular nails address these issues by stabilizing the fibular fragment, promoting alignment, and facilitating healing. Their design enables precise placement and compression, effectively securing fractured segments even in severe comminution. By targeting fibular instability, these nails restore lower limb function and reduce complications linked to inadequate stabilization [15]. Furthermore, fibular nails offer versatility in fracture management, especially in cases where traditional fixation methods are impractical. Their minimally invasive nature reduces soft-tissue disruption, making them advantageous in complex fracture scenarios. The modular design allows for patient-specific approaches, enhancing outcomes in challenging cases. As orthopedic practices evolve, fibular nails remain an invaluable tool, providing innovative solutions for complex fractures and contributing to improved patient care and recovery.
As the demand for optimal patient care continues to grow, it is crucial for physicians to be aware of diverse treatment options for managing distal fibula fractures. This case underscores the fibular nail as a promising alternative to traditional plating systems, offering distinct advantages such as a minimally invasive approach, reduced complication rates, and potential cost-effectiveness. These attributes make the fibular nail particularly valuable for elderly patients and those with comorbidities, who are at higher risk for adverse outcomes with conventional methods. This report contributes to advancing the surgical management of distal fibula fractures by demonstrating the clinical relevance and utility of the fibular nail. It holds significance not only within orthopedic specialties but also has broader implications for improving outcomes across diverse patient populations. Future research should explore large cohort studies to comprehensively compare the long-term stability, rotational displacement management, pain levels, and recovery outcomes between fibular nails and traditional plating techniques. Such studies will further validate the fibular nail’s potential to redefine standard treatment protocols and enhance patient recovery trajectories.
This case underscores the value of fibular nails as a minimally invasive and effective alternative to traditional plating systems in managing distal fibula fractures. It highlights the technique’s advantages, particularly in elderly patients with comorbidities, by reducing complication rates and promoting faster recovery. The report serves as a valuable reference for clinicians seeking innovative approaches to optimize outcomes in complex ankle fracture management.
References
- 1.Yip G, Hay D, Stringfellow T, Ahluwalia A, Ahluwalia R. Assessment and management of adult ankle fractures: Understanding the evidence. Br J Hosp Med (Lond) 2021;82:1-9. [Google Scholar | PubMed]
- 2.Auston DA. Lateral malleolus fixation with fibular rod. J Orthop Trauma 2020.10.1097/bot.0000000000001754, Ahead of Print. [Google Scholar | PubMed | CrossRef]
- 3.Kibble KM, Cunningham BP, Rivard RL, Vang S, Nguyen MP. Ankle fractures: High implant cost is not associated with better patient reported outcomes. Injury 2023;54:110963. [Google Scholar | PubMed]
- 4.Macera A, Carulli C, Sirleo L, Innocenti M. Postoperative complications and reoperation rates following open reduction and internal fixation of ankle fracture. Joints 2018;6:110-5. [Google Scholar | PubMed]
- 5.Kara AN, Esenyel CZ, Sener BT, Merih E. A different approach to the treatment of the lateral malleolar fractures with syndesmosis injury: The ANK nail. J Foot Ankle Surg 1999;38:394-402. [Google Scholar | PubMed]
- 6.Anderson SA, Li X, Franklin P, Wixted JJ. Ankle fractures in the elderly: Initial and long-term outcomes. Foot Ankle Int 2008;29:1184-8. [Google Scholar | PubMed]
- 7.Beleckas CM, Szatkowski JP. Nontraditional methods of fibula fixation. Orthop Clin North Am 2021;52:123-31. [Google Scholar | PubMed]
- 8.White TO, Bugler KE, Appleton P, Will E, McQueen MM, Court-Brown CM. A prospective randomised controlled trial of the fibular nail versus standard open reduction and internal fixation for fixation of ankle fractures in elderly patients. Bone Joint J 2016;98-b:1248-52. [Google Scholar | PubMed]
- 9.Coifman O, Bariteau JT, Shazar N, Tenenbaum SA. Lateral malleolus closed reduction and internal fixation with intramedullary fibular rod using minimal invasive approach for the treatment of ankle fractures. Foot Ankle Surg 2019;25:79-83. [Google Scholar | PubMed]
- 10.Rehman H, Gardner WT, Rankin I, Johnstone AJ. The implants used for intramedullary fixation of distal fibula fractures: A review of literature. Int J Surg 2018;56:294-300. [Google Scholar | PubMed]
- 11.Abdelgaid SM, Moursy AF, Elgebaly EA, Aboelenien AM. Minimally invasive treatment of ankle fractures in patients at high risk of soft tissue wound healing complications. J Foot Ankle Surg 2018;57:557-71. [Google Scholar | PubMed]
- 12.Bäcker HC, Vosseller JT. Fibula fracture: Plate versus nail fixation. Clin Orthop Surg 2020;12:529-34. [Google Scholar | PubMed]
- 13.Bharadwaj S, Ilyas J. Review of outcomes of intramedullary fibular nails in the management of ankle fractures in adults. Cureus 2024;16:e75275. [Google Scholar | PubMed]
- 14.Schmidt EC, Judkins LM, Manogharan G, Mehta S, Hast MW. Current concepts in fracture healing: Temporal dynamization and applications for additive manufacturing. OTA Int 2022;5:e164. [Google Scholar | PubMed]
- 15.Rodriguez-Materon S, Trynz S, Fanfan D, Fleites J, Gil J, Hodgkins C. Use of fibula nails with proximal and distal fixation. Foot Ankle Orthop 2024;9:24730114241230563.10.1177/24730114241230563 [Google Scholar | PubMed | CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review
January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study
January 1, 2026 Outcomes of Unilateral Biportal Endoscopic Surgery for Prolapsed Intervertebral Disc: A Single-center Study November 1, 2025 Arthroscopic Fixation of an Atraumatic Osteochondral Defect of the Knee: A Case Report
November 1, 2025 Arthroscopic Fixation of an Atraumatic Osteochondral Defect of the Knee: A Case Report April 1, 2025 Acute Traumatic Lumbar Spondyloptosis with Complete Neurological Deficit: A Case Report and Literature Review
April 1, 2025 Acute Traumatic Lumbar Spondyloptosis with Complete Neurological Deficit: A Case Report and Literature Review