
In endemic regions, a cystic lumbar spinal lesion causing paraparesis or cauda equina syndrome should prompt consideration of hydatid disease, where early surgical decompression with adjunct albendazole is crucial to prevent irreversible deficits.
Dr. Himanshu Kaushal, Department of Neurology, Guru Gobind Singh Medical College and Hospital, Faridkot, Punjab, India. E-mail: himanshukaushal1993@gmail.com
Abstract
Introduction: Spinal hydatid disease is a rare manifestation of echinococcosis, accounting for <1% of all hydatid infections, with lumbar involvement being uncommon.
Case Report: We report a 40-year-old woman presenting with progressive paraparesis and acute bladder and bowel dysfunction secondary to a primary lumbar spinal hydatid cyst. Imaging revealed a cystic lesion involving the L4 vertebra with extradural compression. The patient underwent posterior decompression, fixation, and complete cyst excision followed by albendazole therapy, with significant neurological improvement on follow-up.
Conclusion: Primary lumbar spinal hydatid disease, though rare, should be considered in endemic regions when evaluating cystic spinal lesions. Early surgical decompression combined with antihelminthic therapy is essential to prevent permanent neurological deficits.
Keywords: Spinal hydatid cyst, lumbar hydatid cyst, cauda equina syndrome, echinococcosis, paraparesis.
Hydatid disease is a parasitic infection caused by the larval stage of Echinococcus granulosus. The liver and lungs are the most commonly affected organs, while skeletal involvement is rare, constituting 0.5–4% of all cases [1]. Spinal hydatid disease is exceptionally uncommon, accounting for 0.2–1% of all hydatid infections, with the thoracic vertebrae most frequently involved, followed by the lumbar spine [1,2]. Spinal hydatid disease poses a diagnostic challenge because of its slow progression, non-specific clinical features, and high recurrence rate [3,4,5]. Neurological compromise usually results from extradural compression or vertebral collapse. We report a rare case of primary lumbar spinal hydatid cyst presenting as acute cauda equina syndrome.
A 40-year-old female presented with a 6-month history of progressive bilateral lower limb weakness, followed by acute urinary and bowel retention for 20 days. There was no history of trauma, fever, weight loss, or contact with livestock. Neurological examination revealed motor power of 3/5 at the knees and 1/5 at the ankles bilaterally. Saddle anesthesia was present, and both knee and ankle reflexes were absent. Upper limb examination was normal. Laboratory investigations showed hemoglobin of 11.6 g/dL, total leukocyte count of 7000/mm3, and an ESR of 40 mm in the 1st h. X-ray of the lumbosacral spine showed mild wedge collapse of the L4 vertebra with well-defined lytic lesions involving the vertebral body and pedicle. Magnetic resonance imaging (MRI) revealed a multiloculated cystic lesion involving the L4 vertebra with pre-vertebral extension and extradural spinal canal compression, findings consistent with hydatid disease. The lesion appeared hypointense on T1-weighted images and markedly hyperintense on T2-weighted images, with minimal peripheral enhancement following gadolinium administration. The intervertebral discs were preserved, a characteristic imaging feature of spinal hydatid disease. Based on imaging characteristics, differential diagnoses considered included spinal tuberculosis, metastatic vertebral disease, and epidural abscess; however, the absence of marrow edema, paravertebral soft-tissue mass, and ring-enhancing abscess favored hydatid disease. To establish the diagnosis of primary spinal hydatid disease, a comprehensive systemic evaluation was performed. Abdominal ultrasonography and contrast-enhanced chest imaging revealed no evidence of hepatic or pulmonary hydatid involvement. Serological testing for echinococcosis was non-contributory, thereby supporting the diagnosis of primary spinal disease. Albendazole therapy was administered at a dose of 15 mg/kg/day (400 mg twice daily), initiated pre-operatively and continued post-operatively for a total duration of three months, in accordance with established recommendations for spinal hydatid disease. Intraoperatively, extensive destruction of the L4 vertebral body with extradural compression was noted. Decompression was achieved through meticulous excision of the cystic lesion. Posterior pedicle screw fixation (L3-L5) with interbody cage placement (L4-L5) was performed to restore spinal stability in view of significant vertebral body compromise. Extreme care was taken to avoid cyst rupture and spillage, with gentle dissection and copious irrigation using scolicidal agents to minimize the risk of recurrence and anaphylaxis. Multiple pearly white cystic structures were removed, and the operative field was irrigated with 20% hypertonic saline as a scolicidal agent. Histopathological examination confirmed a hydatid cyst. Pre-operatively, the patient had severe motor weakness in both lower limbs with medical research council (MRC) grade 2/5 power distally and sensory impairment in the L4-S1 dermatomes. Post-operatively, neurological improvement was noted with recovery to MRC grade 4/5 power proximally; however, bilateral foot drop (MRC grade 2/5) persisted at the past 2-year follow-up. No radiological recurrence was observed. Figure 1. shows preoperative and postoperative radiological findings and cysts removed during the operation.
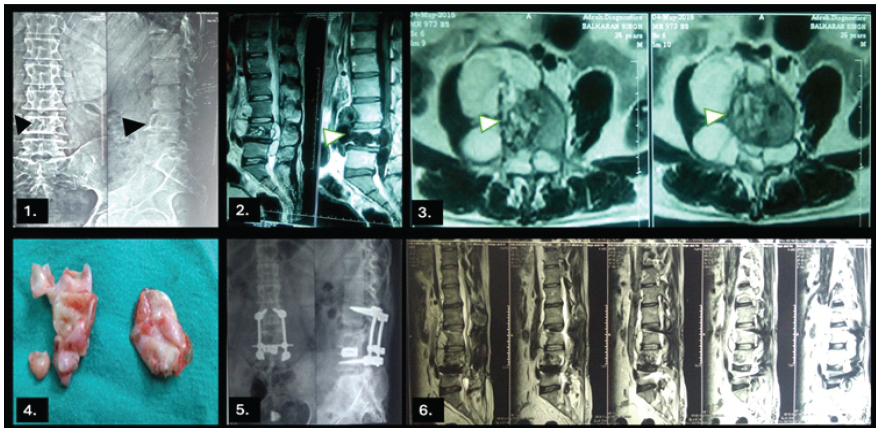
Figure 1: (1) Pre-operative lumbar spine X-ray Anteroposterior and Lateral views showing cystic L4 vertebral lesion (Black solid arrowheads) (2) Pre-operative magnetic resonance imaging (MRI) of the lumbar spine showing a multiloculated cystic lesion involving the L4 vertebral body with epidural extension (arrows) causing significant compression of the thecal sac on T2-weighted sagittal (solid white arrowheads) (3) Pre-operative T2-weighted axial images showing a multiloculated cystic lesion involving the L4 vertebral body with epidural extension (arrows) causing significant compression of the thecal sac (solid white arrowheads) (4) Specimen recovered (5) Post-operative X-ray showing L3-L5 screw fixation and L4-L5 vertebral intrabody cage in place (6) Post-operative MRI showing post-operative findings.
Spinal hydatid disease is a rare but severe form of echinococcal infection. Lumbar involvement accounts for approximately 30–40% of spinal cases [1,5]. The parasite spreads hematogenously through porto-vertebral venous shunts, leading to vertebral destruction and extradural extension [4]. Clinical manifestations include chronic back pain, radiculopathy, paraparesis, paraplegia, and sphincter dysfunction. Acute cauda equina syndrome, as seen in our patient, is extremely rare and results from sudden extradural compression. MRI is the investigation of choice, demonstrating multiloculated cystic lesions that appear hypointense on T1-weighted images and hyperintense on T2-weighted images with non-enhancing walls [2,6,7]. Important differentials include spinal tuberculosis, metastatic disease, and epidural abscess. Surgery remains the cornerstone of treatment and is aimed at complete cyst excision without rupture, adequate spinal cord decompression, irrigation with scolicidal agents, and spinal stabilization [4,5,6]. Albendazole is recommended as adjuvant therapy to decrease the risk of recurrence, although its efficacy in osseous disease remains limited [7]. Recurrence rates range from 30% to 100%, thus necessitating long-term follow-up [1,7]. Indian literature contains only a limited number of documented cases of primary spinal hydatid disease [3,6,8,9,10]. The present case is remarkable for its rare lumbar location, presentation as acute cauda equina syndrome, and favorable neurological recovery following early surgical intervention.
Primary lumbar spinal hydatid cyst is a rare but potentially devastating disease. Early diagnosis using MRI and prompt surgical decompression combined with prolonged albendazole therapy are crucial for neurological recovery and prevention of recurrence.
Primary spinal hydatid disease is a rare but clinically significant cause of acute cauda equina syndrome in endemic regions. This case highlights the importance of considering hydatid disease in cystic vertebral lesions with preserved intervertebral discs, as timely radiological recognition and early surgical decompression combined with prolonged antihelminthic therapy can prevent irreversible neurological deficits.
References
- 1. Turgut M. Hydatid disease of the spine: A survey study from Turkey. Infection 1997;25:221-6. [Google Scholar] [PubMed]
- 2. Braithwaite PA, Lees RF. Vertebral hydatid disease: Radiological assessment. Radiology 1981;140:763-6. [Google Scholar] [PubMed]
- 3. Sharma NK, Chitkara N, Bakshi N, Gupta P. Primary spinal extradural hydatid cyst. Neurol India 2003;51:89-90. [Google Scholar] [PubMed]
- 4. Pamir MN, Akalan N, Ozgen T, Erbengi A. Spinal hydatid cysts. Surg Neurol 1984;21:53-7. [Google Scholar] [PubMed]
- 5. Prabhakar MM, Acharya AJ, Modi DR, Jadav B. Spinal hydatid disease: A case series. J Spinal Cord Med 2005;28:426-31. [Google Scholar] [PubMed]
- 6. Kandwal P, Vijayaraghavan G, Upendra BN, Jayaswal A. Single-stage vertebrectomy for hydatid disease involving L3 vertebra: Five year follow-up. Neurol India 2018;66:1499-501. [Google Scholar] [PubMed]
- 7. Neumayr A, Tamarozzi F, Goblirsch S, Blum J, Brunetti E. Spinal cystic echinococcosis–a systematic analysis and review of the literature: Part 2. Treatment, follow-up and outcome. PLoS Negl Trop Dis 2013;7:e2458. [Google Scholar] [PubMed]
- 8. Gopal NN, Chauhan SP, Yogesh N. Primary spinal extradural hydatid cyst causing spinal cord compression. Indian J Orthop 2007;41:76-8. [Google Scholar] [PubMed]
- 9. Agnihotri M, Goel N, Shenoy A, Rai S, Goel A. Hydatid disease of the spine: A rare case. J Craniovertebr Junction Spine 2017;8:159-60. [Google Scholar] [PubMed]
- 10. Zali A, Shahmohammadi M, Biazar BH, Masoumi N, Samieefar N, Akhlaghdoust M. Spinal hydatid cyst initially diagnosed as spinal tumor: A case report and review of the literature. Clin Case Rep. 2023;11(5):e7244. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Acute Cauda Equina Syndrome Following Transpedicular Biopsy of a Lumbar Vertebral Lesion: A Case Report of Spinal Non-Hodgkin’s Lymphoma
July 1, 2026 Acute Cauda Equina Syndrome Following Transpedicular Biopsy of a Lumbar Vertebral Lesion: A Case Report of Spinal Non-Hodgkin’s Lymphoma March 1, 2026 Silently Gradually Progressing Paraparesis Pott’s Spine Lumbar Vertebra with Bilateral Psoas Abscess
March 1, 2026 Silently Gradually Progressing Paraparesis Pott’s Spine Lumbar Vertebra with Bilateral Psoas Abscess November 1, 2025 Multiple Myeloma Presenting as Cauda Equina Syndrome: A Rare and Early Spinal Manifestation
November 1, 2025 Multiple Myeloma Presenting as Cauda Equina Syndrome: A Rare and Early Spinal Manifestation February 1, 2025 Late Presentation of Cauda Equina Syndrome with Isolated Bladder Bowel Incontinence in Massive Lower Lumbar Disc Herniation: A Series of Three Cases
February 1, 2025 Late Presentation of Cauda Equina Syndrome with Isolated Bladder Bowel Incontinence in Massive Lower Lumbar Disc Herniation: A Series of Three Cases