
Iatrogenic dissociation of bipolar hemiarthroplasty during closed reduction is a rare but serious complication, stressing the need for careful patient assessment and precise technique.
Dr. Catarina Reis Rodrigues, Department of Orthopaedic, Local Health Unit of Alto Minho, Portugal. E-mail: crtrod@gmail.com
Abstract
Introduction: Bipolar hemiarthroplasty (BHA) is widely used for femoral neck fractures, particularly in elderly patients. However, complications such as the rare dissociation of the bipolar cup can severely impact outcomes. This study aims to investigate iatrogenic BHA dissociation following closed reduction, identify risk factors, and discuss preventive strategies.
Material and Methods: A retrospective study was conducted on patients who underwent BHA for femoral neck fractures at our institution between 2019 and 2024. Included patients had a minimum post-operative survival of 3 months. Parameters analyzed included demographics, comorbidities, implant design, dislocation characteristics, and revision procedures.
Results: Among 490 patients who underwent BHA, 64 dislocation episodes were identified. The incidence of component dissociation related to closed reduction was 20.3%, representing 13 iatrogenic cases. One patient experienced two episodes of dissociation. The mean Charlson comorbidity index was 6.0, indicating a high comorbidity burden. All dissociations involved implants with a single circumferential polyethylene locking ring. The “O-shape sign” was evident in nine cases. Revision procedures included total hip arthroplasty, open reduction with component replacement, or Girdlestone resection arthroplasty.
Conclusion: Iatrogenic dissociation of BHA following closed reduction, though rare, represents a serious complication with significant clinical implications. This study highlights the critical role of implant design, particularly single locking mechanisms, in increasing dissociation risk. Careful pre-reduction assessment, use of fluoroscopic guidance, and awareness of radiographic risk signs are vital to prevention. Multidisciplinary management addressing frailty and comorbidities is essential for optimizing outcomes.
Keywords: Bipolar hemiarthroplasty, dissociation, dislocation, closed reduction, polyethylene locking ring.
Hip hemiarthroplasty (HA) is a well-established surgical treatment for femoral neck fractures, particularly in the elderly. Despite evolving articles that increasingly favor total hip arthroplasty (THA) for more active patients [1,2], HA remains a preferred option for those with lower functional demands. While HA is associated with a higher reoperation rate, it offers a lower reported risk of dislocation compared to THA [3]. Among HA complications, dislocation is uncommon but significantly impacts morbidity, quality of life, and mortality. Higher dislocation rates have been observed in patients with pre-operative acetabular dysplasia, suggesting they may be better candidates for THA [4]. The debate between unipolar and bipolar HA (BHA) remains unresolved, with some evidence suggesting that bipolar implants may offer advantages in delaying acetabular wear and improving quality of life beyond the first 2 years after surgery [5,6,7], whereas others have shown no differences in hip function, complications, and dislocation risk [8,9]. Notably, BHA designs have been associated with a lower revision rate than unipolar implants, though unipolar HA may be justified for patients with a limited life expectancy (<2.5 years) [10]. A rare but serious complication is dissociative BHA dislocation, where the inner femoral head separates from the outer acetabular cup. The most common cause reported is spontaneous dissociation (48.6%) without preceding trauma. However, trauma-related cases (18.1%) have also been noted, as well as iatrogenic cases (26.4%) following closed reduction maneuvers [11]. The consequences of this complication can be severe, often requiring revision surgery and substantially affecting patient outcomes. Given the rarity and clinical significance of this complication, this study aims to contribute to the existing literature by presenting thirteen cases of bipolar cup dissociation occurring after closed reduction of a dislocated prosthesis, in the absence of mechanical failures. In addition, we provide a comprehensive literature review to enhance understanding of this uncommon yet critical issue.
The study protocol was approved by the institutional ethics committee (IEC No. 23/2025; approval date: June 25, 2025), and the requirement for informed consent was waived. We conducted a retrospective descriptive review of all patients who underwent BHA for femoral neck fractures at our institution between 2019 and 2024. Inclusion criteria encompassed patients with a minimum post-operative survival of 3 months and documented post-operative dislocation followed by closed reduction attempts complicated by implant component dissociation. Exclusion criteria included prosthetic mechanical failures unrelated to reduction maneuvers and incomplete clinical records. Data collected comprised demographics, comorbidities, implant design details, time to dislocation, mechanism of injury leading to dislocation, radiographic characteristics focusing on dislocation morphology, and details of revision surgeries. Descriptive statistics were applied to clinical and radiological data.
During the study period, a total of 514 BHA were performed. After applying the inclusion criteria, 490 BHAs were included in our analysis. Hip dislocation occurred in 33 patients (6.7%), some of whom experienced multiple episodes, resulting in 64 dislocation events (13.1%). The mean time to first dislocation was 19 days postoperatively. Among these, 13 cases (20.3%) developed iatrogenic dissociation of the acetabular cup following the close reduction. One patient had two episodes of dissociation. Table 1 summarizes the patient demographics, comorbidities, prosthetic details, dislocation characteristics, and management strategies. Analysis of the clinical backgrounds of patients experiencing BHA dissociation revealed common demographic and medical traits linked with increased risk.
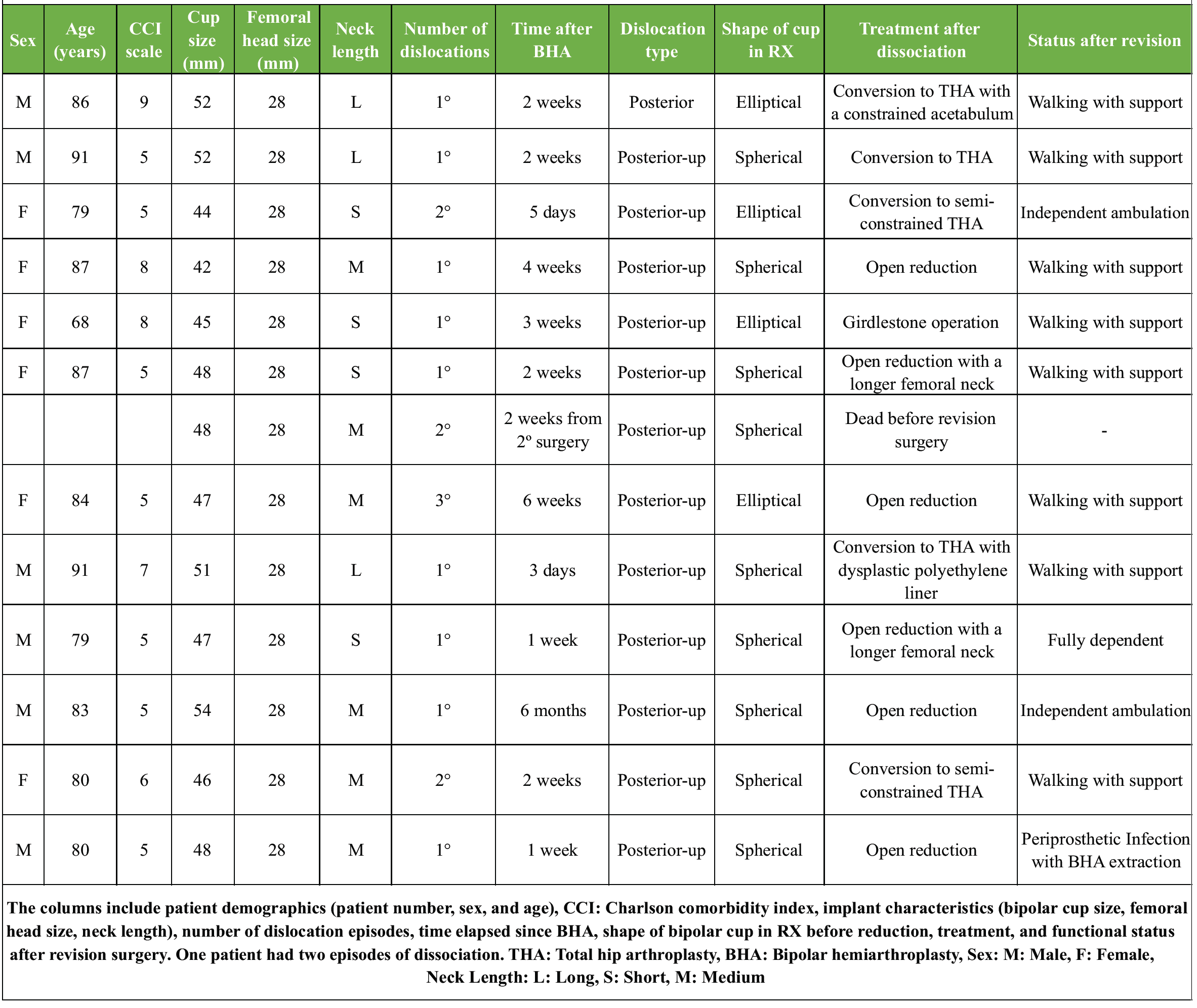
Table 1: Detailed clinical and surgical data of patients who experienced dissociation after bipolar hip hemiarthroplasty
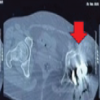
The cohort consisted mainly of elderly patients (mean age 78.4 years), most of whom had significant functional dependence and resided in long-term care facilities. Cardiovascular comorbidities – including hypertension, ischemic heart disease, and congestive heart failure – were highly prevalent, and advanced respiratory disease, such as chronic obstructive pulmonary disease, was present in four patients. Neurological impairments were frequent, with Parkinson’s disease diagnosed in 5 patients (45%), dementia in 4 (36%), and prior cerebrovascular accidents resulting in residual hemiparesis in two. The mean Charlson comorbidity index (CCI) of 6.0 indicates a high burden of chronic conditions. All cases were performed using a posterolateral surgical approach and involved bipolar head prostheses with a single circumferential polyethylene locking ring. The femoral head was 28 mm, and the bipolar acetabular cup diameter ranged from 42 to 52 mm, with the neck length ranging from S to L. The mean time to dislocation was 4 weeks post-surgery, with 12 cases showing posterior-up dislocations. Notably, in nine patients, dissociation occurred during the first episode of dislocation. Pre-reduction radiographs exhibited a spherical or “O-shaped” acetabular cup in nine cases (Fig. 1), previously thought to predict successful closed reductions.
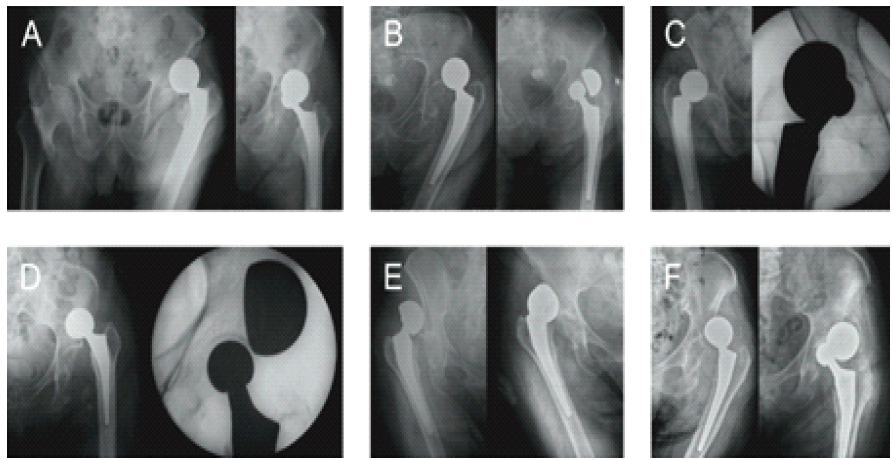
Figure 1: Pre-reduction dislocation and associated dissociation after closed reduction. (a, b, c) The spherical shape of the acetabular cup, the “O-Shaped” sign. (d, e, f) The elliptical shape of the acetabular cup.
No fluoroscopic imaging was utilized during closed reduction procedures, which were performed using conventional maneuvers under sedation and muscle relaxation. Revision procedures included constrained or semi-constrained THA (five cases), open reduction and replacement with the same size acetabular cup and femoral head ± a longer femoral neck (six cases), and Girdlestone resection arthroplasty (one case). Functional outcomes varied, with some patients regaining functional mobility while others required prolonged rehabilitation.
Guo et al. classified BHA dissociation into three types based on etiology. Type I, iatrogenic dissociation, occurs during closed reduction due to mechanical failure – commonly described as the “bottle opener effect,” in which the posterior acetabular rim acts as a fulcrum, forcing the cup away from the femoral head (Fig. 2).
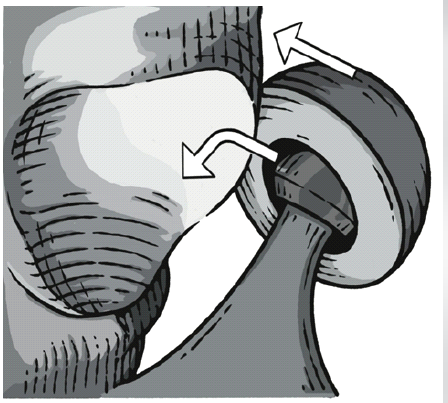
Figure 2: “Bottle opener effect” illustration. The posterior acetabular rim acts as a fulcrum during traction, locking the cup and levering it away from the femoral head, which predisposes to component dissociation.
Type II, polyethylene insert erosion, results from chronic wear that weakens the locking ring. Type III, spontaneous dissociation, arises from progressive intra-acetabular dislocation [12]. This study highlights iatrogenic BHA dissociation (Type I) following closed reduction and presents, to date, the largest number of reported cases of iatrogenic dissociation (Table 2), surpassing prior reports such as Lee et al. 13% (7/55 dislocations) [13].
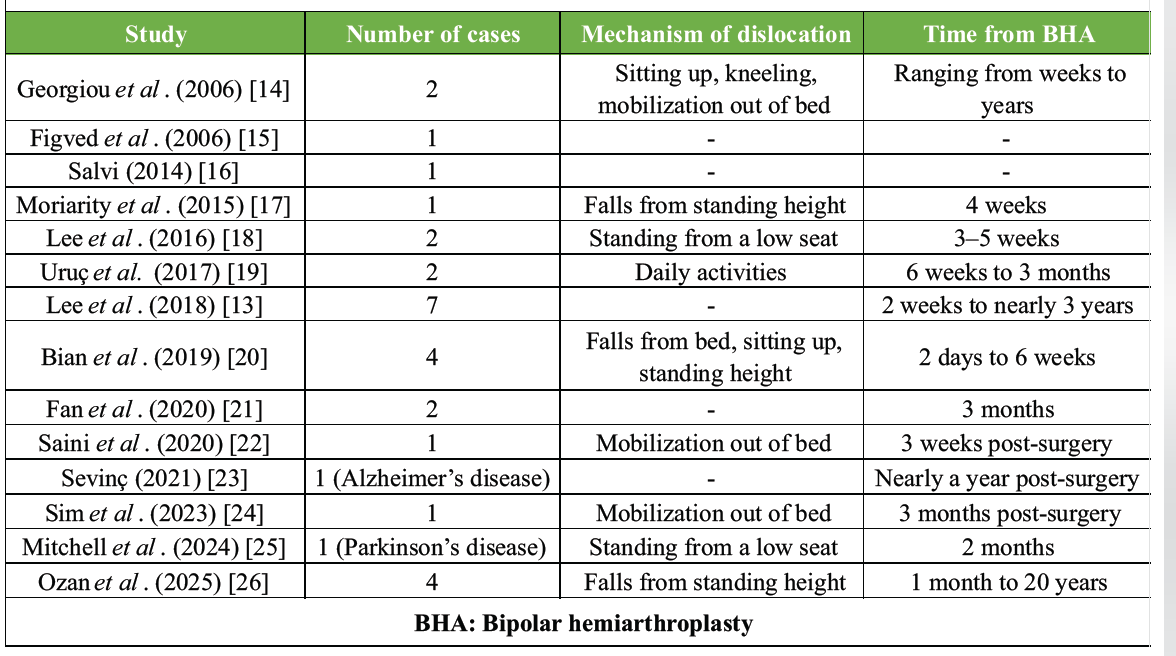
Table 2: Case reports in the literature of BHA iatrogenic dissociation secondary to close reduction after dislocation
Our findings emphasize the critical role of patient comorbidities, implant design, reduction techniques, and radiographic predictors in preventing dissociation and improving patient outcomes.
Patient comorbidities
Our findings highlight that patients experiencing BHA dissociation form a highly vulnerable group characterized by advanced age and significant functional dependence, frequently living in long-term care facilities. The mean CCI score of 6.0 in our cohort reflects a substantial burden of comorbidities. Neurological disorders, such as Parkinson’s disease, dementia, previous cerebrovascular events with residual impairments, and cognitive dysfunction, are increasingly recognized as independent and potent predictors of BHA instability, as evidenced by recent multivariate analyses [27,28]. These neurological deficits impair motor coordination and amplify fall risk, thereby contributing crucially to the mechanical instability that predisposes to implant dislocation.
Role of implant design
Bipolar implants utilize either single or dual locking mechanisms to secure the femoral head within the outer metal shell. Single-lock designs rely on a polyethylene ring that expands into a groove within the polyethylene liner, whereas dual-lock designs incorporate an additional metal locking ring for enhanced stability. Our study exclusively involved prostheses featuring a single circumferential polyethylene locking ring. Although somewhat outdated, these implant designs remain clinically relevant as they are still widely implanted globally, particularly in regions with limited access to newer prosthetic technologies. Lee et al. previously highlighted this single locking mechanism as a factor potentially increasing dissociation risk during closed reduction by concentrating stress on the polyethylene ring instead of distributing it across a dual locking system [13]. Ozan et al. classified BHA cups into three design types. Type 1 features a polyethylene insert integrated with the metal acetabular shell; Type 2 includes a single circumferential polyethylene locking ring, as used in our cases; and Type 3 combines a polyethylene locking ring with a conical metal shell. Their study used cam-out and pull-out tests to simulate forces that might cause dissociation during clinical procedures. The cam-out test measures how rotational and axial forces can displace components, whereas the pull-out test assesses the force needed to separate the femoral head from the acetabular component [26]. Type 2 implants showed greater vertical displacement before release in cam-out tests compared to Types 1 and 3, suggesting better resistance during closed reduction maneuvers. However, despite this biomechanical strength, clinical dissociations still occurred in our study, likely because of additional levering forces during closed reductions – known as the “bottle opener” effect – which are not replicated in static tests. Therefore, although Type 2 implants show superior vertical displacement resistance in controlled testing, they remain vulnerable under the complex dynamic forces involved in actual reduction maneuvers.
Radiographic predictors of dissociation
The “O-shape sign” on pre-reduction radiographs has been suggested as an important predictor of closed reduction success. Sim et al. reported that a concentric “O”-shaped femoral head and cup on anteroposterior views correlates with successful closed reduction, whereas an elliptical appearance is associated with dissociation risk [24]. In our study, however, nine out of thirteen cases displayed spherical form or the “O-shape sign” yet still experienced dissociation, indicating that while this radiographic finding may suggest an optimal reduction trajectory, it is not a fail-proof predictor of stability.
Alternative reduction techniques
To minimize the risk of iatrogenic dissociation, Bian et al. proposed a modified reduction technique known as the “Push-Turnover-Pull” maneuver. This approach helps prevent excessive leveraging forces on the polyethylene ring, thereby reducing the likelihood of dissociation. In addition, in cases where resistance is encountered, dynamic fluoroscopic imaging should be utilized to guide reduction and confirm the integrity of the components [20]. Once dissociation occurs, management must be tailored to the patient’s specific needs, considering acetabular integrity, functional status, and the surgeon’s expertise. In our study, revision strategies included open reduction and component replacement, where the acetabular cup and femoral head were replaced with components of the same size to ensure proper engagement of the locking mechanism. In cases requiring additional stability, a longer femoral neck was used to improve joint mechanics. Conversion to THA was preferred for patients at high risk of recurrent instability, with both constrained and non-constrained liners considered based on the individual patient’s needs. Girdlestone resection arthroplasty was reserved for low-demand patients with limited mobility, severe comorbidities, or cases deemed non-reconstructable, offering pain relief at the expense of hip function. Cases of failed BHA converted to THA demonstrated improved pain relief and function, with perioperative complications comparable to standard revision THA procedures [29,30]. In addition, optimizing soft-tissue tension and, when necessary, utilizing a longer femoral neck (offset) contributed to joint stability and helped reduce the risk of further dislocations. The use of unipolar HA remains a topic of discussion, particularly considering the risk of dissociation associated with BHA. While bipolar prostheses may offer reduced acetabular wear, the need for surgical intervention in cases of dissociation can offset this advantage. Given this risk, some authors suggest opting for unipolar prostheses in certain cases to minimize future complications [25].
This study highlights the significant clinical issue of iatrogenic dissociation following closed reduction of dislocated BHA, with an incidence of 20.3% in a cohort of 64 BHA dislocations. The vulnerability of patients with multiple comorbidities, advanced age, and neurological impairments must be recognized as a key contributor to prosthetic instability. All of the cases involved prostheses with a single circumferential polyethylene locking ring, underscoring the critical influence of implant design on dissociation risk. While biomechanical testing suggests Type 2 prostheses (single locking ring) demonstrate superior resistance to simple cam-out forces compared to other designs, clinical evidence may reveal vulnerability to levering forces described as the “bottle opener” effect during dynamic reduction maneuvers. To minimize dissociation risk, surgeons should employ gentle, controlled reduction techniques such as the Push-Turnover-Pull maneuver and use dynamic fluoroscopic imaging for real-time guidance. Radiographic predictors such as the O-shape sign may guide reduction attempts but are insufficient alone to guarantee stability. In instances where resistance is encountered during reduction, proceeding directly to open reduction may be the safest approach. Pre-operative comprehensive assessments of frailty, comorbid diseases, and neurological status are paramount for optimizing outcomes. Further research is warranted to refine prosthetic designs and reduction techniques, focusing on enhancing patient safety and minimizing complications in this fragile population.
Limitations
This retrospective single-center study has limitations, including: No control group, descriptive statistics only, heterogeneous unstratified comorbidities, non-standardized reductions or surgeon experience, single polyethylene locking rings (no dual-locking comparison), absent biomechanical/radiographic analyses, no validated long-term functional/patient-reported outcome measures, and limited external validity for modern bipolar systems with improved locking mechanisms. Although our series represents one of the larger cohorts of iatrogenic bipolar dissociations reported to date, the absolute number of dissociation events (13 cases) remains relatively small and precludes more definitive conclusions or robust hypothesis testing.
When reducing a dislocated BHA in high-risk patients, clinicians should avoid forceful traction and use fluoroscopic or modified maneuvers to limit the “bottle opener effect” to minimize the risk of catastrophic component dissociation and the need for complex revision surgery.
References
- 1. Meermans G, Talevski D, Studers P, Togrul E, Nazaruddin RG, Sukhonthamarn K, et al. Is there a difference in outcomes between hemiarthroplasty and total hip arthroplasty for patients who have displaced femoral neck fractures? J Arthroplasty 2025;40:S138-40.e4. [Google Scholar] [PubMed]
- 2. Liu Y, Chen X, Zhang P, Jiang B. Comparing total hip arthroplasty and hemiarthroplasty for the treatment of displaced femoral neck fracture in the active elderly over 75 years old: A systematic review and meta-analysis of randomized control trials. J Orthop Surg Res 2020;15:215. [Google Scholar] [PubMed]
- 3. Zi-Sheng A, You-Shui G, Zhi-Zhen J, Ting Y, Chang-Qing Z. Hemiarthroplasty vs primary total hip arthroplasty for displaced fractures of the femoral neck in the elderly: A meta-analysis. J Arthroplasty 2012;27:583-90. [Google Scholar] [PubMed]
- 4. Zanna L, Innocenti M, Secci G, Cipolleschi L, Carulli C, Civinini R. Acetabular morphology predicts the risk of dislocation following hemiarthroplasty for femoral neck fractures in the elderly. J Arthroplasty 2023;38:1773-8. [Google Scholar] [PubMed]
- 5. Inngul C, Hedbeck CJ, Blomfeldt R, Lapidus G, Ponzer S, Enocson A. Unipolar hemiarthroplasty versus bipolar hemiarthroplasty in patients with displaced femoral neck fractures: A four-year follow-up of a randomised controlled trial. Int Orthop 2013;37:2457-64. [Google Scholar] [PubMed]
- 6. Hedbeck CJ, Blomfeldt R, Lapidus G, Törnkvist H, Ponzer S, Tidermark J. Unipolar hemiarthroplasty versus bipolar hemiarthroplasty in the most elderly patients with displaced femoral neck fractures: A randomised, controlled trial. Int Orthop 2011;35:1703-11. [Google Scholar] [PubMed]
- 7. Imam MA, Shehata M, Abdallah AR, Ahmed H, Kader N, Ernstbrunner L, et al. Unipolar versus bipolar hemiarthroplasty for displaced femoral neck fractures: A pooled analysis of 30,250 participants data. Injury 2019;50:1694-708. [Google Scholar] [PubMed]
- 8. Comeau-Gauthier M, Bzovsky S, Axelrod D, Poolman RW, Frihagen F, Bhandari M, et al. Is the use of bipolar hemiarthroplasty over monopolar hemiarthroplasty justified? A propensity score-weighted analysis of a multicentre randomized controlled trial. Bone Jt Open 2023;4:370-7. [Google Scholar] [PubMed]
- 9. Khan AQ, Mohammad J, Qamar R, Siddiqui YS, Sabir AB, Abbas M. Cemented unipolar or modular bipolar hemiarthroplasty for femoral neck fractures in elderly patients – which is better? Int J Burns Trauma 2021;11:447-55. [Google Scholar] [PubMed]
- 10. Farey JE, Cuthbert AR, Adie S, Harris IA. Revision risk after unipolar or bipolar hemiarthroplasty for femoral neck fractures: An instrumental variable analysis of 62,875 procedures from the Australian orthopaedic association national joint replacement registry. J Bone Joint Surg Am 2021;103:195-204. [Google Scholar] [PubMed]
- 11. Yang Y, Fu G, Li Q, Zhang R, Liao W, Ma Y, et al. Multivariable analysis of risk factors affecting dislocation after bipolar hemiarthroplasty in patients with femoral neck fracture. Ther Clin Risk Manag 2022;18:101-11. [Google Scholar] [PubMed]
- 12. Guo JJ, Yang H, Yang T, Tang T. Disassembly of cemented bipolar prothesis of the hip. Orthopedics 2008;31:813. [Google Scholar] [PubMed]
- 13. Lee YK, Park CH, Ha YC, Koo KH. What is the frequency of early dissociation of bipolar cups and what factors are associated with dissociation? Clin Orthop Relat Res 2018;476:1585-90. [Google Scholar] [PubMed]
- 14. Georgiou G, Siapkara A, Dimitrakopoulou A, Provelengios S, Dounis E. Dissociation of bipolar hemiarthroplasty of the hip after dislocation. A report of five different cases and review of literature. Injury 2006;37:162-8. [Google Scholar] [PubMed]
- 15. Figved W, Norum OJ, Frihagen F, Madsen JE, Nordsletten L. Interprosthetic dislocations of the charnley/hastings hemiarthroplasty–report of 11 cases in 350 consecutive patients. Injury 2006;37:157-61. [Google Scholar] [PubMed]
- 16. Salvi AE. “Bottle-opener” effect in bipolar hip prostheses dislocations. J Arthroplasty 2014;29:2053-4. [Google Scholar] [PubMed]
- 17. Moriarity A, Ellanti P, Talha S, McKenna J. Dislocation and dissociation of bipolar hip hemiarthroplasty. BMJ Case Rep 2015;2015:bcr2015210282. [Google Scholar] [PubMed]
- 18. Lee SC, Baek JH, Nam CH, Choi KW, Chang SH, Ha YC. Dissociation of inner bearing of bipolar cups during closed reduction: A report of two cases with biomechanical testing. Curr Orthop Pract 2016;27:E1-3. [Google Scholar] [PubMed]
- 19. Uruç V, Özden R, Duman İG, Kalacı A. Five cases of early dissociation between the bipolar hip endoprosthesis cup components; Either spontaneously or during reduction maneuvers. Acta Orthop Traumatol Turc 2017;51:172-6. [Google Scholar] [PubMed]
- 20. Bian YY, Wang LC, Xiao K, Jin J, Zhang BZ, Weng XS. Hip dislocation and femoral component disassembly after bipolar hemiarthroplasty: A report of four cases and introduction of new reduction maneuvers. Chin Med J (Engl) 2019;132:370-2. [Google Scholar] [PubMed]
- 21. Fan X, Wang J, Zhang D, Mao F, Liao Y. Early Recurrent Dislocation and Dissociation of Bipolar Cup: Two Intricate Cases and Review of Literature. United States: Research Square; 2020. [Google Scholar] [PubMed]
- 22. Saini MK, Reddy NR, Reddy PJ. Disassembly of components of a monoblock bipolar hip prosthesis following dislocation: A case report and review on “bottle opener effect”. J Orthop Case Rep 2020;10:90-3. [Google Scholar] [PubMed]
- 23. Sevinç HF. Dissociation of bipolar components following bipolar hemiarthroplasty: A report of two different cases and review of the literature. Ulus Travma Acil Cerrahi Derg 2021;27:600-3. [Google Scholar] [PubMed]
- 24. Sim SB, Son SW, Shim BJ. Be aware of the “O” sign in the bipolar cup dissociation during closed reduction of bipolar dislocation: A case report. Medicine (Baltimore) 2023;102:e35234. [Google Scholar] [PubMed]
- 25. Mitchell A, Belkin N, Sarpong N, Herndon CL, Hickernell TR. A rare complication of intraprosthetic dissociation of cemented bipolar hemiarthroplasty during closed hip reduction: Case report and literature review. J Hip Surg 2024;8:58-64. [Google Scholar] [PubMed]
- 26. Ozan F, Okur KT, Mavi F, Pekedis M. Biomechanical and clinical assessment of dissociation in bipolar hip hemiarthroplasty. Biomed Mater Eng 2025;36:185-99. [Google Scholar] [PubMed]
- 27. Graulich T, Graeff P, Jaiman A, Nicolaides S, Omar Pacha T, Örgel M, et al. Risk factors for dislocation after bipolar hemiarthroplasty: A retrospective case-control study of patients with CT data. Eur J Orthop Surg Traumatol 2021;31:627-33. [Google Scholar] [PubMed]
- 28. Suh KT, Kim DW, Lee HS, Seong YJ, Lee JS. Is the dislocation rate higher after bipolar hemiarthroplasty in patients with neuromuscular diseases? Clin Orthop Relat Res 2012;470:1158-64. [Google Scholar] [PubMed]
- 29. Park KS, Chan CK, Lee DH, Yoon TR. Midterm results of conversion from failed bipolar hemiarthroplasty to total hip arthroplasty. Indian J Orthop 2018;52:369-73. [Google Scholar] [PubMed]
- 30. Poursalehian M, Hassanzadeh A, Lotfi M, Mortazavi SM. Conversion of a failed hip hemiarthroplasty to total hip arthroplasty: A systematic review and meta-analysis. Arthroplast Today 2024;28:101459. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Neglected Bipolar Hemiarthroplasty Dislocation in a Young Adult with Superior Acetabular Wall Defect – A Case Report
May 1, 2026 Neglected Bipolar Hemiarthroplasty Dislocation in a Young Adult with Superior Acetabular Wall Defect – A Case Report May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report
May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report May 1, 2026 Traumatic Obturator Variant of Anterior Hip Dislocation – A Case Series
May 1, 2026 Traumatic Obturator Variant of Anterior Hip Dislocation – A Case Series February 1, 2026 Closed Traumatic Dislocation of 2nd–4th Metatarsophalangeal Joints with Associated 5th Metatarsal Base Fracture: A Rare Case Report
February 1, 2026 Closed Traumatic Dislocation of 2nd–4th Metatarsophalangeal Joints with Associated 5th Metatarsal Base Fracture: A Rare Case Report