
Distal femur fractures are complex in nature and their management is technically challenging. Retrograde nailing is associated with better outcomes in our study, however larger, multi-center studies may be required for guiding a consensus.
Dr. Faisal Harun, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: dr.faisalharun@gmail.com
Abstract
Introduction: Distal femur fractures due to their complex characteristics can give nightmares to trauma surgeons. Goal of treatment is to restore normal anatomy, achieve bone union and restore early joint movement. Both retrograde nail (RN) and locking compression plate (LCP) are used for internal fixation. However, superiority of one over other is debatable.
Aims and Objectives: The aim of the study was to compare functional outcome, intra-operative parameters and complications of LCP and RN.
Materials and Methods: This was a prospective comparative study conducted between August 2022 and August 2024. 46 skeletally mature patients of distal femur fracture were included in the study, out of which 23 were treated with LCP and 23 with RN. Fractures classified as AO Type A2, A3, and C1 fractures were included in the study. Hospital for special surgery knee rating scale (HSS) was used for functional outcome. Complications such as non-union, infection, anterior knee pain and knee stiffness were compared between two groups during follow-up.
Results: Blood loss was significantly more in plating group, whereas radiation exposure was significantly more in nailing group. The patients were followed-up for a duration of 18 months. Knee flexion was significantly more in RN group. Early union was seen in nailing, with more cases of anterior knee pain, whereas more flexion deformity and extensor lag were observed in the LCP group. One case of each non-union and infection was seen in RN group. However, these parameters were comparable (P > 0.05). Mean HSS score at final follow-up was 77.32 ± 16.70 in the LCP group and 84.16 ± 10.23 in RN group, with no significant difference.
Conclusion: Retrograde nailing comes out with better outcomes in terms of early union, less intra-operative blood loss and less post-operative complications. However, a larger study may still be needed for the results to be accepted into standard practice.
Keywords: Distal femur fracture, locking compression plate, retrograde nail, union.
Distal femur fractures are defined as fractures up to 15 cm from the distal articular surface of femur [1]. Less than 1% of all fractures and 4–6% of all femoral fractures are said to be distal femur fractures. Two distinct mechanisms of injury cause distal femur fractures in two separate populations [2]. Distal femur fractures mainly result from low-energy trauma, such as falls and sprains that are worsened by a high rate of comorbidity in the elderly population with osteoporotic bone and a fragile soft-tissue environment. High-energy trauma in young patients causes complex injury with comminuted and open fracture pattern [3]. The distal femur is anatomically composed of a broad medullary cavity and a thin cortical bone. Rigid fixation of these fractures is challenging due to extensive soft-tissue damage, extension of the fracture line into the joint, severe comminution and displacement [4]. The goal of treatment for distal femur fractures is to achieve bone union and restore early knee joint movement [5]. Despite widespread use of both locking plate and retrograde nail (RN), the optimal method among the two is a topic of debate, with superiority of one over the other in the context of pros and cons of their use. The purpose of this study was to compare both techniques in terms of functional outcome, intraoperative parameters and post-operative complications.
This was a prospective comparative study performed in a tertiary care hospital between August 2022 and August 2024. After obtaining approval from the Institutional Ethical Committee (IEC Approval No: IECJNMC/830, dated October 19, 2022) and getting an informed consent form duly signed, 46 patients with distal femur fractures were included in the study following the inclusion and exclusion criteria.
Inclusion criteria
- Skeletally mature patients
- AO Type A2, A3 and C1 distal femur fractures
- Closed and Gustilo Type 1 and 2 open fractures
- Unilateral fractures
- Patients who were able to walk without any assistance before
Exclusion criteria
- Pathological fractures
- Periprosthetic distal femur fractures
- Fractures associated with neurovascular
Out of 46 patients, 23 patients were treated by a single lateral locking compression plate (LCP), whereas 23 patients were treated by RN. Implants used in both groups were manufactured by the same company, and most cases were done in the emergency OT. Tourniquet was not used in any of the cases.
Surgical techniques LCP
Patients were placed supine with the knee flexed to 30° (a bolster was placed in supracondylar region to correct hyperextension deformity at the fracture site). A bump was also placed below the ipsilateral hip to maintain neutral rotation of femur. Minimally Invasive Plate Osteosynthesis was used in cases where fracture geometry was simple and extra-articular, but in intra-articular and complex unreducible fractures, the fracture site exposed using either a lateral parapatellar or a direct lateral approach. In cases of intra-articular fractures, a 6.5 mm locking cancellous screws were used for interfragmentary compression after reduction of articular fragments using a pointed reduction clamp. After satisfactory reduction, plate of adequate length was applied and screws inserted taking into consideration of screw density.
RN
Patients were settled supine with access to fluoroscopy. The affected side was placed in 60° flexion at knee. A 3 cm longitudinal infra-patellar skin incision was centered over the patellar tendon, and the tendon split longitudinally in its middle. The insertion point was confirmed radiologically with both AP and lateral views in the intercondylar notch anterior to Blumensaat’s line and in projection of the femoral shaft axis. Fracture was reduced, and guide wire inserted followed by serial reaming until the cortical chatter was appreciated. A nail of size 1 mm less than the last reamer employed was inserted and advanced with the final position of the distal end well below the subchondral bone established under fluoroscopy. The distal locking screws were inserted using the aiming device and trocar. Proximally, either jig-enabled or free-hand locking of two interlocking bolts was implemented.
Rehabilitation protocol
Knee physiotherapy and non-weight bearing walk was started immediately from post-op day one. Progressive Quadriceps Strengthening and Straight leg raise were emphasized. Between 6 and 10 weeks, the patient was shifted to partial weight-bearing walk depending upon radiological evidence of callus formation. Full weight-bearing walk started depending on the clinico-radiological features of bone healing. X-rays were done at each follow-up to assess radiological union and implant failure. knee flexion, anterior knee pain, flexion deformity, extensor lag, signs of infection and non-union were observed in follow-up. Clinical outcome assessment was done according to Hospital for special surgery knee rating scale (HSS).
Statistical analysis
Categorical variables were presented in number and percentage (%), and continuous variables were presented as mean ± standard deviation. Quantitative variables were compared using student’s t-test, whereas qualitative variables were assessed using Chi-square test and fisher exact t-test. A P < 0.05 was considered statistically significant.
In the LCP group, 1 patient died in follow-up and 1 lost to follow-up due to change of location, whereas two patients died in RN group. All mortalities were not related to injuries rather due to pre-existing co-morbidities. Mean age in the LCP and RN group were 35.91 ± 17.76 and 42.48 ± 16.90 years, respectively. Most common age group in LCP group was 15–30 years, while in RN group, it was 46–60 years. Overall, there were 63% males and 37% females. Road traffic accident (RTA) was found to be the most common mode of injury, constituting 67.4% cases. RTA was common among young males, whereas trivial trauma was more common among old females likely due to Osteoporosis. Due to high velocity trauma, these fractures were associated with other injuries. In our study, the most common associated injuries were ipsilateral lower limb fractures followed by head injury. Hypertension was seen in 13% population in the study. Other comorbidities such as diabetes and coronary artery disease were also present, which were needed to be optimized. These comorbidities also predispose to post-operative morbidity and mortality. Demographics and fracture pattern in both groups are given in Table 1.
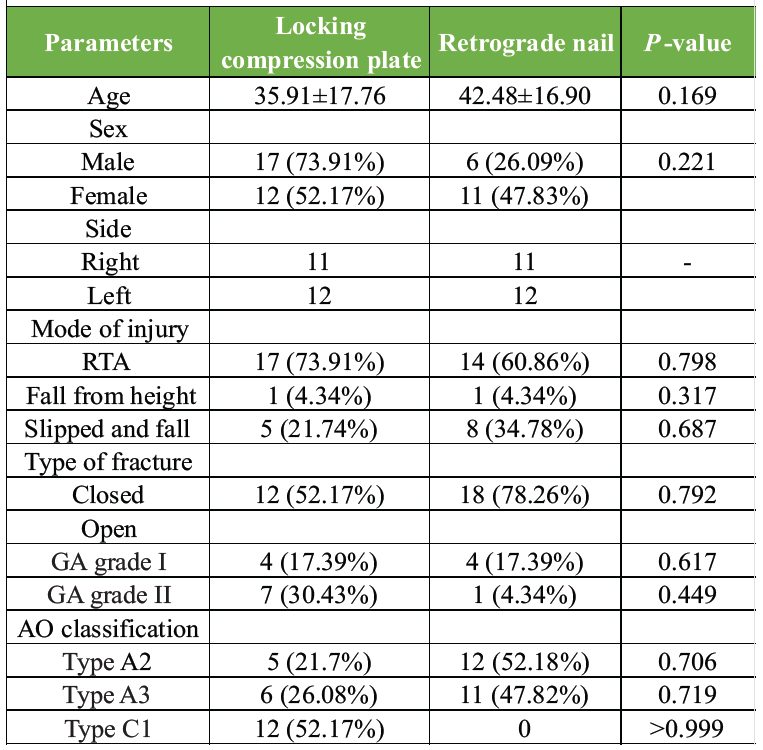
Table 1: Demographics and fracture pattern in two groups
In the RN group, 74% cases were operated with CRIF and 26% cases operated with mini-open technique (Figs. 1, 2).

Figure 1: Showing (a) radiographs of a patient with spiral fracture of left distal femur; (b) immediate post-operative radiographs of the same patient, managed operative by closed reduction and internal fixation with supracondylar nail; (c) follow-up radiographs after 1 year; (d-f) complete range of motion of patient at 1-year follow-up.

Figure 2: (a) Radiographs of a patient with comminuted fracture of right distal femur; (b) immediate post-operative radiographs of the same patient, managed operative by closed reduction and internal fixation with supracondylar nail; (c) follow-up radiographs after 1 year; (d-f) complete range of motion of patient at 1-year follow-up.
In LCP group, 43.5% patients were operated using MIPO, whereas in 56.5%, ORIF was used (Figs. 3, 4).
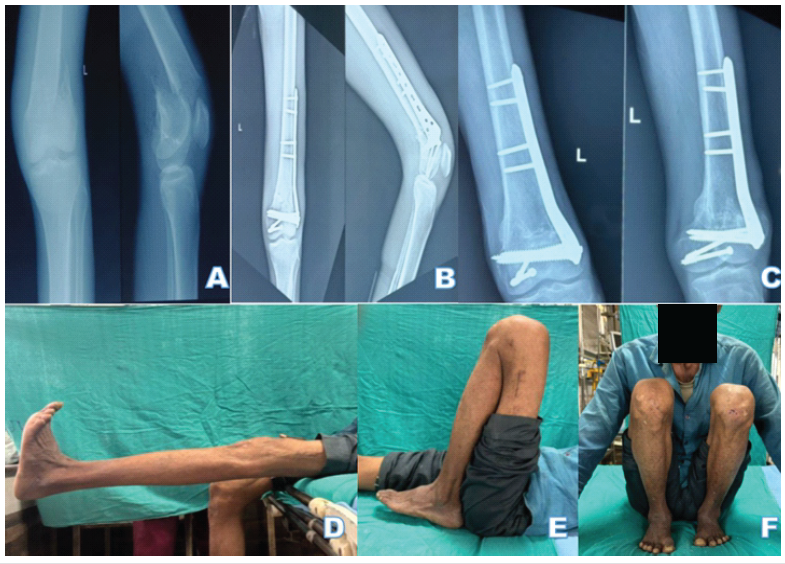
Figure 3: (a) Radiographs of a patient with fracture of the left distal femur; (b) immediate post-operative radiographs of the same patient, managed operative by open reduction and internal fixation with distal femur locking plate; (c) follow-up radiographs after 1 year; (d-f) complete range of motion of the patient at 1-year follow-up.

Figure 4: (a) Radiographs of a patient with fracture of right distal femur; (b) immediate post-operative radiographs of the same patient, managed operative by open reduction and internal fixation with distal femur locking plate; (c) follow-up radiographs after 1 year; (d) flexion deformity of 10° and (e) extensor lag of 60° at 1-year follow-up, which may be contributed by the advanced tricompartmental knee osteoarthritis of the patient.
Mean blood loss was 310 mL and 181 mL in LCP and RN group, respectively, with a statistically significant difference. Order of mean blood loss seen in the LCP group was ORIF (lateral parapatellar)>ORIF (Lateral approach)>MIPO. Mean operative time was 119.2 min and 123.5 min in LCP and RN group with an insignificant difference. Radiation exposure was measured in terms of no. of C-arm shots taken during surgery. Mean no. of C-arm shots taken in LCP and RN group were 24 and 33 with a statistically significant difference (Table 2).
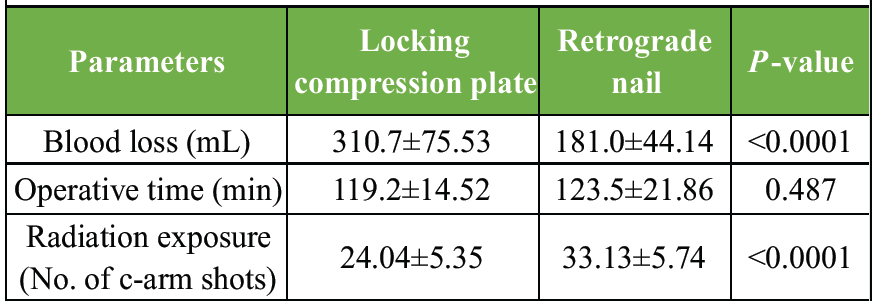
Table 2: Intraoperative parameters in two groups
Both groups of patients were followed up for a duration of 18 months. Mean union time in LCP and RN groups was 26 and 22 weeks, respectively, with no significant difference. Union rate was 100% in LCP, whereas in RN group, it was 95%. Mean knee flexion in the LCP and RN groups was 100.5° and 123.7°, respectively, with a statistically significant difference. Three patients in the plating group were having knee flexion ≤60°, among which two patients had intra-articular fractures and one patient was having severe osteoarthritis of knee. All three patients were non-compliant to post-operative rehabilitation exercises (Table 3).
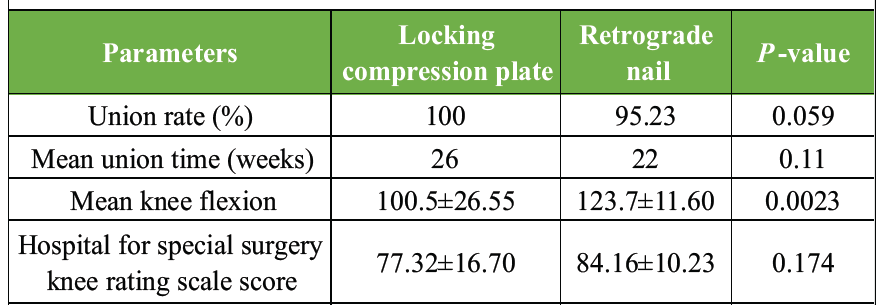
Table 3: Functional Outcome in two groups
Functional outcome assessment was done using HSS at the last follow-up. Mean HSS score in LCP and RN groups was 77.32 and 84.16, respectively. However, there was no statistically significant difference. HSS score ≥70 was seen in 95.2% and 71.4% patients in plating and nailing group, respectively. Fall in HSS score was observed with increasing age (Table 3 and 4).
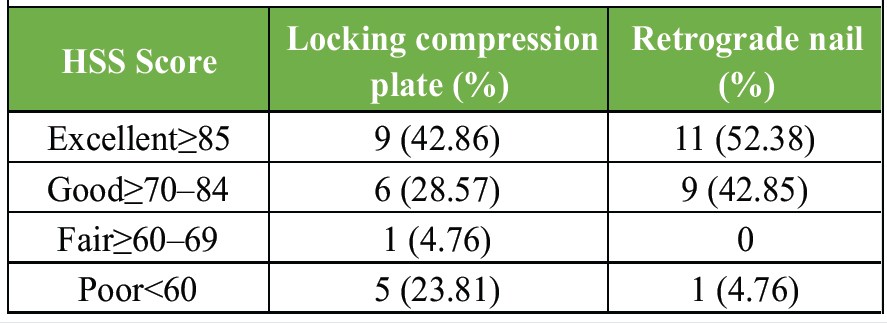
Table 4: Functional outcome in terms of hospital for special surgery knee rating scale score in both groups
The return to work and recreational activities was satisfactory in both groups, except five patients in the LCP group and one patient in the RN group, who had poor outcomes as well as HSS scores at the end of the follow-up period.
Extensor lag was also observed in some patients due to quadriceps weakness. Extensor lag (≥10°) was seen in 47.6% and 42.8% patients in LCP and RN groups, respectively. Mean extensor lag measured in LCP and RN group was 11.9° and 8.9° in LCP and RN groups, respectively. Lag was seen mostly in older patients. Flexion deformity was seen in 38.1% and 14.3% cases in the LCP and RN group, respectively, with no statistically significant difference (Fig. 4). Non-union was seen only in one case of the nailing group, while no case observed in plating group. This case was managed with freshening of fracture margins with exchange nailing with iliac crest bone grafting. Knee pain was observed in 14.3% and 19% patients in LCP and RN group, respectively. Deep infection was observed in one patient of the nailing group after fracture union, which was treated by implant removal (Fig. 5).

Figure 5: Pus discharging sinus over antero-medial aspect of left knee operated with retrograde nailing in the distal femur fracture.
No case of implant failure was seen in any group in the study. Shortening (>2 cm) was seen in 9.5% and 14.3% cases in the LCP and RN group, respectively (Table 5).
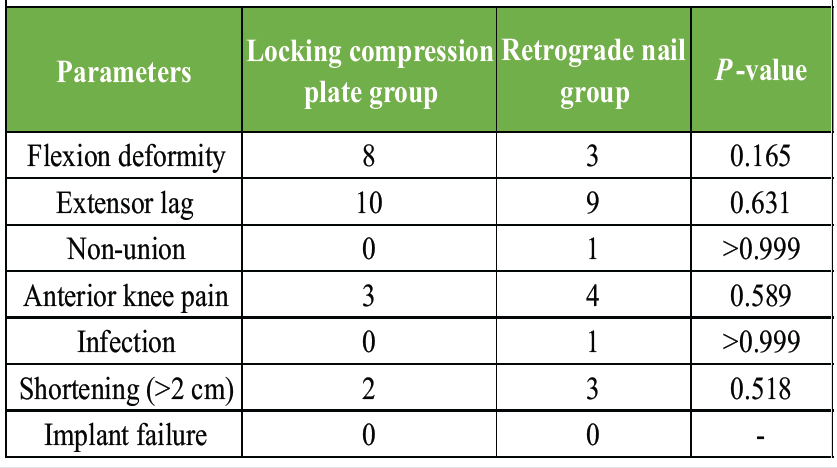
Table 5: Post-operative Complications in two groups
Distal femur fractures have always remained a controversial subject to treat for orthopedic surgeons. Despite modern fixation techniques, distal femur fractures often result in continued disability and worse outcomes [6]. These are usually complex injuries associated with soft-tissue loss and severe comminution. Treatment requires skill and meticulous technique for a good outcome. However, newer biological methods of fixation have reduced the union and infection problems; their treatment still remains an enigma to the treating surgeon [2]. Despite numerous advances in operative techniques and implant designs, the incidence of non-union and need for secondary procedures has been well documented with the surgical treatment of these injuries [7].
Treatment for the fractures of the distal femur has evolved from the use of condylar screw and angled blade plate to the use of LCP and retrograde intramedullary nailing [8]. These days, habitually applied methods are retrograde nailing and locked plating [3,9]. Both allow fixation with minimal soft-tissue dissection and can adhere to the principle of biological osteosynthesis [8]. The locking plate relies on the principles of absolute stability and interfragmentary compression to achieve union. The technique of retrograde nailing uses indirect reduction of the metaphyseal fracture component and offering relative stability [10].
The present study shows significantly more blood loss and radiation exposure in LCP group as compared to RN group. More bleeding in LCP was due to more cases of open reduction, unlike closed reduction in all cases of RN. Gill et al. also suggested significant blood loss in the LCP group [2]. Contrary to this, Gao et al. found more blood loss in nailing compared to plating, but insignificant [11]. However, both these studies employed minimal invasive plating, unlike our study. Radiation exposure was more in nailing mainly due to the indirect reduction technique. Apart from reduction, entry making and freehand proximal locking are challenging tasks and require multiple exposures. Operative time was similar in both groups. Other studies have also shown different results. Operative time varies with operating surgeon experience and team, implants and instruments at disposal and operation theatre standards [12].
Non-union was seen in only one case of nailing, which can be attributed to the thinner nail leading to excessive motion at the fracture site. Most studies suggest more union rate in nailing. Study of Gao et al. suggests more non-union in the plating group. It was argued that the callus formation in locking plates is asymmetric and less compared to nails, which is a centric load-sharing device. The stiffness of a fixation construct is a principal determinant of the motion of a fracture site and therefore affects the mechanism and progression by which a fracture is healed [11]. Study of Gill et al. showed 90% union rate in both techniques. They also suggested early union in RN due to intramedullary contents released at fracture site during reaming. An intramedullary stabilization along with a long working length, also appears to be an adjuvant factor for early union in nails [2]. Our study and most other studies show early union in nailing, but not significant (P > 0.05). However, Gupta et al. observed longer union time in nailing, which is unlikely to other studies [13].
Mean degrees of flexion were found to be significantly higher in nailing compared to plating. Flexion deformity and extensor lag were also more in the LCP group, but not statistically significant. In RN group, knee joint was not involved as no intra-articular fractures were included in this group. In addition, less soft-tissue stripping required, which produces less fibrosis in RN and more patients with osteoarthritis knee were included in the LCP group who had prior reduced ROM in the injured knee. However, literature shows that ROM is a variable parameter which is not related to the implant. Adequate reduction and a strong fixation construct, which is followed by early rehabilitation exercises, is the key. Delayed operation due to comorbidities and associated injuries, non-compliance to knee physiotherapy and extensive soft-tissue stripping led to quadriceps weakness.
Knee pain was seen in 17% cases of RN and 13% of LCP in our study. This can be attributed to damage to the patellar and femoral cartilage while reaming and nail insertion, despite taking precautions. However, knee pain in plating can be due to impingement of soft tissues by plate and screws, which is less likely. Primary Osteoarthritis in old-aged patients and the development of early osteoarthritis in intra-articular fractures who are operated with LCP is most likely reason of knee pain. Discrimination of knee pain due to multiple reasons is difficult. Gao et al., Shroff et al. and Solanki et al. suggested more cases of knee pain in LCP with insignificant difference [11,14,15]. However, Gill et al. showed 18% cases of knee pain in LCP, contrast to only 5% cases in RN [2].
Numerous scales have been used for the assessment of the functional outcome of patients in distal femur fractures. Time-to-time evolution of scoring systems has emerged for functional outcome evaluation and comparison between different surgical techniques. Hence, many studies have been done to compare the functional outcome of distal femur fractures and the most common scoring systems used are knee society score and Neer score. Other scoring systems used in various studies were Lysholm Gillquist scoring system (LGSS), Sanders’ scoring, the knee and osteoarthritis outcome score (KOOS), Schatzker and Lambert criteria, lower extremity functional scale (LEFS).
In our study, mean HSS score was compared, which was not significantly different. Yadav et al., Gupta et al., and Gao et al. had also compared the functional outcome on the basis of HSS score, but all have showed no significant difference between both the groups. HSS score is mainly based on functional abilities of knee joint and post-operative complications such as knee pain, flexion deformity, malalignment and extensor lag. As knee pain was seen more in RN, whereas extensor lag and flexion deformity were more in LCP. These parameters compensate each other while calculation of HSS score, giving an insignificant difference in results. In our study, 43% and 28.5% cases have excellent and good outcome in LCP, and 52% and 43% have excellent and good outcome in RN. Approx. 24% and 5% cases have poor outcome in LCP and RN group. Haider et al. graded 52% and 25% as excellent outcome in LCP and RN groups, respectively, in terms of HSS score, whereas 5.4% and 21.4% cases had poor outcome in LCP and RN groups [16]. Compared to our study, Haider et al., Gao et al. and Yadav et al. showed better results in LCP because they have taken only extra-articular fractures in their study, as compared 12 intra-articular fractures taken in LCP group in our study [11,16,17]. Mean HHS score of RN group of our study is similar to the study of Gao et al. and Gupta et al. [11,13] (Table 6).
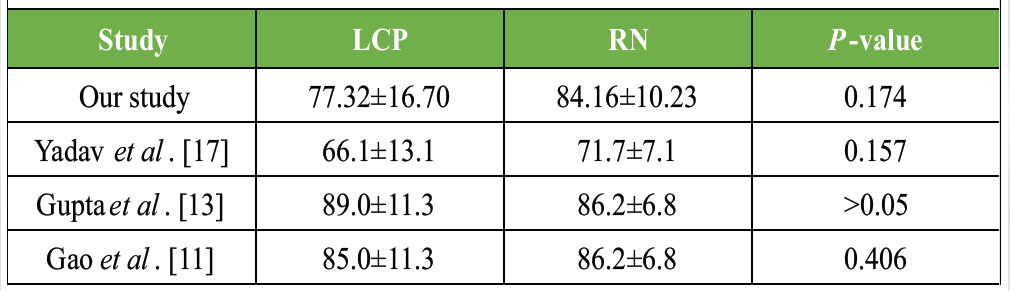
Table 6: Comparison of locking compression plate (LCP) and retrograde nail (RN) according to hospital for special surgery knee rating scale Score in various studies
Limitation
Although studies have been performed on this topic by an even smaller cohort, a larger number of patients would further strengthen the study and even enable stratification of fracture types. Inclusion of more scoring systems like the SF-36, KOOS, or EQ-5D would have provided a more comprehensive comparison. Surgeries in both groups were performed by different surgeons, which may have some bearing on the results, although the standard techniques for operative methods remained the same. All intra- articular fractures were managed by LCP in the study, which may cause discrepancy in results.
LCP can be used in any fracture morphology where RN works well in extra-articular fractures. In the open reduction technique, there is loss of fracture hematoma and soft-tissue stripping. However, MIPO technique has overcome these complications. Early union, better knee ROM, and less post-operative complications were associated in patients managed with RN. Satisfactory reduction, adequate fixation and early rehabilitation are the key for better outcome.
Compared to LCP, RN is associated with less intraoperative blood loss, earlier union, greater knee flexion, and fewer complications, despite more radiation exposure and anterior knee pain.
References
- 1. Singh S, Baghel PK, Rastogi D, Shantanu K, Sharma V. Distal femoral locked plating versus retrograde nailing for extra articular distal femur fractures: A comparative study. Int J Orthop Sci 2018;4:702-5. [Google Scholar] [PubMed]
- 2. Gill S, Mittal A, Raj M, Singh P, Singh J, Kumar S. Extra articular supracondylar femur fractures managed with locked distal femoral plate or supracondylar nailing: A comparative outcome study. J Clin Diagn Res 2017;11:RC19-23. [Google Scholar] [PubMed]
- 3. Hierholzer C, Von Rüden C, Pötzel T, Woltmann A, Bühren V. Outcome analysis of retrograde nailing and less invasive stabilization system in distal femoral fractures: A retrospective analysis. Indian J Orthop 2011;45:243-50. [Google Scholar] [PubMed]
- 4. Chandra Vemulapalli K, Pechero GR, Warner SJ, Achor TS, Gary JL, Munz JW, et al. Is retrograde nailing superior to lateral locked plating for complete articular distal femur fractures? Injury 2022;53:640-4. [Google Scholar] [PubMed]
- 5. Yoon BH, Park IK, Kim Y, Oh HK, Choo SK, Sung YB. Incidence of nonunion after surgery of distal femoral fractures using contemporary fixation device: A meta-analysis. Arch Orthop Trauma Surg 2021;141:225-33. [Google Scholar] [PubMed]
- 6. Hoffmann MF, Jones CB, Sietsema DL, Tornetta P 3rd, Koenig SJ. Clinical outcomes of locked plating of distal femoral fractures in a retrospective cohort. J Orthop Surg Res 2013;8:43. [Google Scholar] [PubMed]
- 7. Rodriguez EK, Zurakowski D, Herder L, Hall A, Walley KC, Weaver MJ, et al. Mechanical construct characteristics predisposing to non-union after locked lateral plating of distal femur fractures. J Orthop Trauma 2016;30:403-8. [Google Scholar] [PubMed]
- 8. Neradi D, Sodavarapu P, Jindal K, Kumar D, Kumar V, Goni V. Locked plating versus retrograde intramedullary nailing for distal femur fractures: A systematic review and meta-analysis. Arch Bone Jt Surg 2022;10:141-52. [Google Scholar] [PubMed]
- 9. Markmiller M, Konrad G, Südkamp N. Femur-LISS and distal femoral nail for fixation of distal femoral fractures: Are there differences in outcome and complications? Clin Orthop Relat Res 2004;426:252-7. [Google Scholar] [PubMed]
- 10. Krishna C, Shankar RV. Current concept of management of supracondylar femur fracture: Retrograde femoral nail or distal femoral locking plate. Int Surg J 2016;3:1356-9. [Google Scholar] [PubMed]
- 11. Gao K, Gao W, Huang J, Li H, Li F, Tao J, et al. Retrograde nailing versus locked plating of extra-articular distal femoral fractures: Comparison of 36 cases. Med Princ Pract 2013;22:161-6. [Google Scholar] [PubMed]
- 12. Agarwal S, Udapudi S, Gupta S. To assess functional outcome for intra-articular and extra-articular distal femur fracture in patients using retrograde nailing or locked compression plating. J Clin Diag Res 2018;12:RC21-4. [Google Scholar] [PubMed]
- 13. Gupta SK, Govindappa CV, Yalamanchili RK. Outcome of retrograde intramedullary nailing and locking compression plating of distal femoral fractures in adults. OA Orthop 2013;1:23. [Google Scholar] [PubMed]
- 14. Shroff AS, Bhamare DS, Herode P, Sadaria MH, Patel JM. Comparison of outcomes of supracondylar femur fractures treated with locking compression plate vs supracondylar nail. Surg Update Int J Surg Orthop 2017;3:120-6. [Google Scholar] [PubMed]
- 15. Solanki M, Kelkar RY, Chhutani D. Comparative study between results of retrograde intramedullary nailing (RN) vs locked plating (LP) in treatment of extra articular distal femur fracture: A prospective analysis. Int J Orthop Sci 2019;5:574-8. [Google Scholar] [PubMed]
- 16. Haider MI, Siddiq K, Jamal A, Razzaque MA, Nazir A, Anjum MI. Comparison of functional outcome of closed retrograde nailing and mippo (minimally invasive percutaneous plate osteshnthesis) distal femoral locking plate fixation for distal femoral fractures. Pak J Med Health Sci 2022;16:488. [Google Scholar] [PubMed]
- 17. Yadav CB, Limbu A, Rajak A, Rijal R, Shrestha BP, Maharjan R, et al. Functional outcome of retrograde nailing versus locked plating of extra-articular distal femoral fractures in adults: A randomized controlled trial. J Kathmandu Med Coll 2021;9:122-9. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Distal Femoral Replacement in Young Adults with Traumatic Comminuted Distal Femur Fractures: A Report of Two Cases
April 1, 2026 Distal Femoral Replacement in Young Adults with Traumatic Comminuted Distal Femur Fractures: A Report of Two Cases February 1, 2026 Anterior Minimally Invasive Plate Osteosynthesis Versus Open Reduction Plate Osteosynthesis in Humeral Diaphyseal Fractures: A Functional and Clinical Analysis
February 1, 2026 Anterior Minimally Invasive Plate Osteosynthesis Versus Open Reduction Plate Osteosynthesis in Humeral Diaphyseal Fractures: A Functional and Clinical Analysis October 1, 2025 Bilateral Traumatic Scaphoid Fracture Managed Surgically with Headless Compression Screw: A Case Report with Review Literature
October 1, 2025 Bilateral Traumatic Scaphoid Fracture Managed Surgically with Headless Compression Screw: A Case Report with Review Literature October 1, 2025 Radiological and Functional Assessment of Tibial Plateau Fractures Managed with Locking Compression Plates: A Prospective Study
October 1, 2025 Radiological and Functional Assessment of Tibial Plateau Fractures Managed with Locking Compression Plates: A Prospective Study