
An uncommon mechanical failure of the proximal femur nail and the subsequent management of the same.
Dr. Nirvin Paul, Department of Trauma Surgery, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India. E-mail: drnirvinpaul@gmail.com
Abstract
Introduction: Intertrochanteric fractures are increasingly common in the elderly, and intramedullary fixation with a proximal femoral nail antirotation (PFNA) is widely preferred due to its biomechanical advantages. The helical blade improves cancellous bone purchase, yet complications such as cut-out, cut-in, and excessive sliding remain concerns. Mechanical uncoupling of the helical blade from the nail is extremely rare. We report an unusual case of spontaneous helical blade disengagement following PFNA fixation of a stable fracture.
Case Report: An 85-year-old male sustained a stable intertrochanteric femur fracture following a road traffic accident and underwent closed reduction with a long PFNA fixation, achieving good reduction and implant placement. Early recovery was uneventful. At 8 weeks, he developed proximal thigh pain and a firm mass. Imaging showed subcutaneous migration of the uncoupled distal helical blade without additional trauma. The component was removed under local anesthesia, and weight-bearing was deferred. Alignment remained stable, and at 12 months, a painless fibrous non-union allowed continued conservative management.
Conclusion: Helical blade uncoupling is an exceptionally rare PFNA failure mode. In elderly, low-demand patients with stable alignment and minimal symptoms, conservative treatment after such mechanical failure can provide satisfactory outcomes without revision surgery.
Keywords: Proximal femur nail, uncoupling of helical blade, mechanical failure.
Rising life expectancy worldwide has led to an increase in the geriatric population, which in turn has caused a higher incidence of trochanteric fractures. It is estimated that by 2050, approximately 4.5 million people annually worldwide will be affected by hip fractures [1]. The mortality rate within the 1st year after hip fracture surgery ranges from 15% to 30% [2]. It is crucial that these elderly individuals regain their previous function and ambulate as soon as possible because over 50% lose their independence due to prolonged hospital stays, infections, or delayed mobilization [3]. Therefore, early surgical intervention with stable fixation is vital for mobility and a better quality of life. The ideal implant of choice for the management of intertrochanteric fractures is debatable. Traditionally, extramedullary devices such as the dynamic hip screw, dynamic condylar screw, and locking condylar blade plate were used for fixation. Intramedullary fixation devices for intertrochanteric fractures were introduced in the 1990s and have undergone significant design upgrades over time. Currently, intramedullary devices are the preferred modality of fixation, due to biological and biomechanical advantages over extramedullary devices [4]. The proximal femoral nail (PFN) with screw (second generation) was introduced by AO/ASIF in 1996. The helical blade PFN (third generation) was developed by AO/ASIF in 2003, which improved on the femoral head purchase employing lesser bone loss and better fixation as a result of radial compaction of the cancellous bone around the helical blade [5,6]. The commonly reported complications with the trochanteric fixation systems include excessive helical blade sliding, varus collapse, screw pull-out, superolateral cut-out, and medial cut-through [7,8]. Herein, we report an unusual complication of uncoupling of the helical blade following treatment of a stable intertrochanteric fracture with PFN antirotation (PFNA).
An 85-year-old man reported to the emergency room (ER) with pain, swelling, external rotation deformity of the right lower limb, and inability to walk as a result of a traffic collision (2-wheeler vs. pedestrian). In the ER, the ATLS protocol was followed. The patient was clinically and hemodynamically stable, and there were no systemic injuries on the primary survey. He was sent for a radiograph after stabilization, and it revealed a stable intertrochanteric fracture of the right femur (AO/OTA classification A 1.2), with a Singh’s Index of grade 3 (Fig. 1).
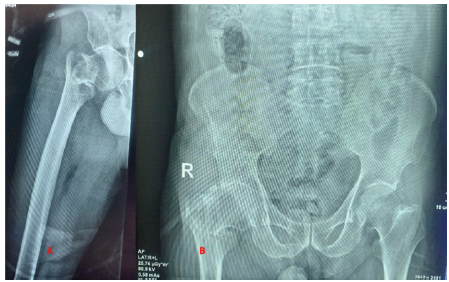
Figure 1: Pre-operative X-ray (AO/OTA A1.2).
He underwent closed reduction and an intramedullary nail fixation under spinal anesthesia. An anatomical reduction was achieved, and a long PFNA was inserted without any difficulty (size – 10 × 400 mm with a 95 mm helical blade and 2 distal interlocks of size 46 and 52 mm).
Post-operative radiographs were obtained, and they showed a neutral reduction, a Baumgaertner’s Tip Apex Distance (TAD) of 19.73 mm, the neck shaft angle was 138°, and Parker’s ratio was 38.9% (Figs. 2 and 3).
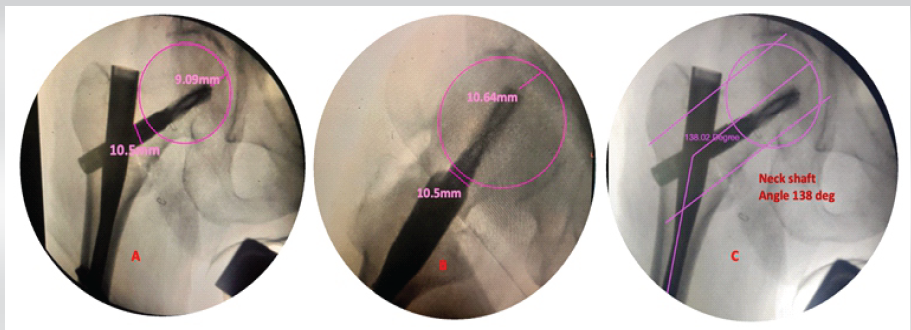
Figure 2: Intraoperative assessment of tip apex distance (TAD) (a) in anterior posterior 9.09 mm, 10.64 mm in lateral view (b), and total TAD = 19.73 mm (c) neck shaft angle 138°s.
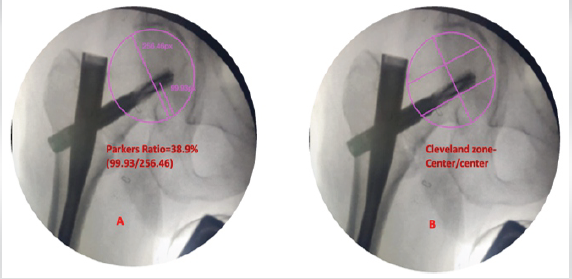
Figure 3: (a) Parker’s ratio 38.9%, (b) Cleveland zone-center/center
The post-operative fracture gap was <1 mm, and Garden alignment index was good, and the center of the helical blade was placed in the Cleveland zone center–center. The reduction quality was good according to the Baumgaertner reduction quality criteria, and excellent according to the Chang reduction quality criteria, respectively.
The perioperative period was uneventful, and the patient was started on partial weight-bearing walking with the aid of a walker after assessment of the reduction on the post-operative radiograph. He underwent suture removal on day 14 post-operative, and he had an uneventful recovery at the 6-week follow-up. However, he presented 2 weeks later with pain in the proximal thigh and a palpable hard mass. The patient did not report any history of accidental falls, was afebrile, and the local site was unremarkable. The inflammatory indicators were within the normal range (erythrocyte sedimentation rate 18 mm/h, C-reactive protein 2 mg/dL). Our clinical diagnosis was screw pull-out, varus collapse, and implant failure; however, imaging revealed that the distal half of the helical blade had uncoupled from the blade and was impinging on the skin (Fig. 4 and 5).
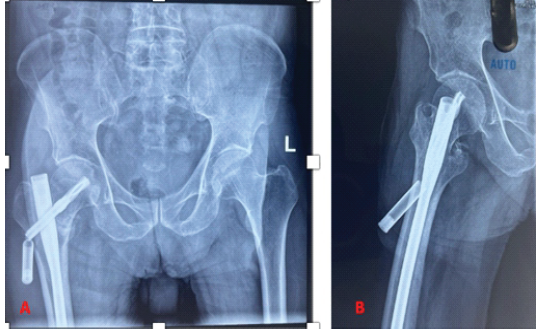
Figure 4: Anterior posterior (a) and lateral radiograph (b) showing uncoupling of helical blade.
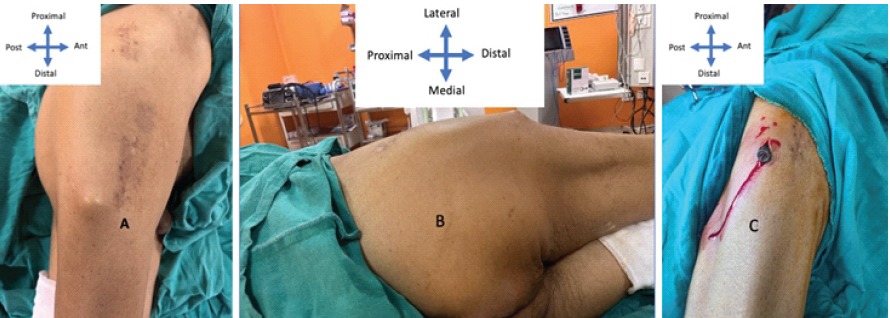
Figure 5: Clinical picture at 2 months presentation (a), bony hard swelling at the lateral proximal thigh (b), Uncoupled component (c).
Following the diagnosis, we planned to remove the uncoupled component and wait for union. The uncoupled component was removed in the minor theatre on an outpatient basis (Fig. 6).
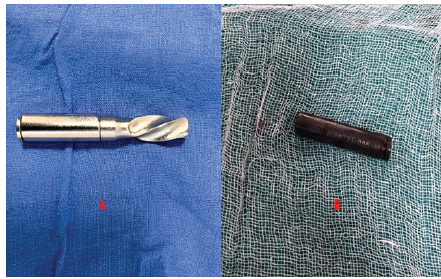
Figure 6: (a) Intact helical blade, (b) uncoupled component.
The patient was advised to continue physiotherapy, but weight bearing was deferred. The risk factors for collapse and the need for a possible revision surgery were explained to the patient. He was urged to follow up every 4 weeks till bony union. At the 16-week follow-up, he was clinically pain-free, and there was no further collapse or loss in reduction; hence, progressive weight-bearing mobilization was started.
The patient remained asymptomatic till the 12-month follow-up, and a computed tomography was obtained, which revealed a fibrous non-union. However, the patient was asymptomatic and did not have any limp or abductor lurch, and the Harris Hip Score was 84. The head was viable, and options were explained to the patient, who opted for conservative management (Fig. 7).
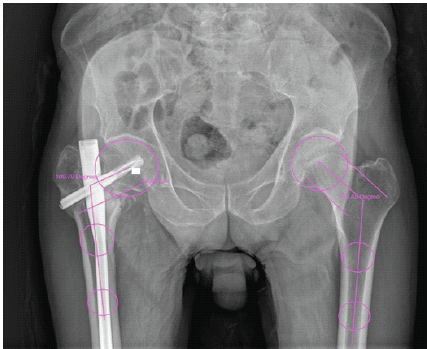
Figure 7: X-ray at follow-up of 18 months.
With increased life expectancy, the number of per-trochanteric fractures is projected to double by 2050 [9]. Fracture-related mortality and morbidity are considerably decreased by early surgical stabilization of the fracture, allowing for early mobility and return to pre-fracture activity levels, which remains the primary goal of surgery [10]. Elderly individuals are more vulnerable to complications after surgery, such as wound infections, pneumonia, urinary tract infections, and cardiovascular events. Above that, due to insufficient bone quality or osteoporosis, fixing fractures and union becomes challenging. Due to implant failure, one out of every five trochanteric fracture fixations fails, increasing hospital stays, treatment costs, morbidity, and mortality [11]. Despite advances in implant design and technique, fixation failure remains a notable complication in osteoporotic bone due to poor bone quality and altered biomechanics. To overcome the problems with previous intramedullary devices, such as the Gamma nail, including rotational instability and femoral shaft fractures at the nail tip, Simmermacher et al. created the AO/ASIF PFN [12]. The subsequent modification, called PFNA, improved rotational stability and load distribution in osteoporotic femoral heads by replacing the dual screw structure with a single helical blade intended to crush cancellous bone. The helical blade has several special challenges, even though it should increase purchase and decrease cut-out rates. Mechanical failures, including varus collapse, excessive blade sliding, cut-out, cut-through, and medial migration (cut-in), have been documented [13,14]. In a prospective randomized study comparing screw-type PFN and helical PFN in older patients with unstable trochanteric fractures, Kumar and Srivastava [14] found no significant differences in union rates, complications, or functional outcomes; however, the helical PFN group experienced less blood loss and operative time. These findings confirm that surgical technique, reduction quality, and implant positioning are the major determinants of success, rather than implant type alone. In approximately 2.2% of PFNA patients, Yam et al. [15] identified a unique mechanical failure pattern called “cut-in,” characterized by superomedial migration of the helical blade through the femoral head into the hip joint. The main risk factors were severe osteoporosis (bone mineral density <−2.5), poor blade alignment, and insufficient reduction. The possible risk associated with PFNA’s lack of a mechanical anti-slide locking function was also highlighted by Chen et al. [16], who reported a catastrophic case of pelvic perforation in a severely osteoporotic patient as a result of excessive medial sliding of the PFNA blade. These findings highlight the importance of achieving optimal blade positioning (center–center or inferior–center) and maintaining a TAD between 20 and 25 mm to prevent both cut-out and cut-in failures. In contrast to cut-in and cut-out mechanisms, the current case demonstrates an even rarer phenomenon: The helical blade’s uncoupling from its nail interface. Such mechanical separation is quite rare to our knowledge and most likely indicates a manufacturing or fatigue-related breakdown at the blade–nail coupling junction. This atypical failure pattern can be explained by several interrelated mechanisms:
- (i). Mechanical disengagement at the coupling interface: The press-fit locking mechanism in the PFNA design does not have a separate anti-rotation screw. In osteoporotic bone, repetitive axial micro-motion may gradually loosen the coupling, predisposing to disengagement [17]
- Cyclic axial loading and interface fatigue: Transmitted stresses concentrate at the coupling junction in fractures with limited impaction or when telescoping ceases prematurely, causing micro-fretting and eventual separation [13]
- Insertional or manufacturing factors: Under repeated physiological loads, incomplete mechanical engagement or slight variation in design tolerance could predispose to early fatigue.
In the present case, the disengaged helical blade was removed under local anesthesia as part of conservative management because the fracture was still well reduced and there was no infection or loss of alignment. The patient subsequently achieved stable fibrous union and pain-free mobility. Angelini et al. [17] emphasized that in low-demand elderly patients with stable alignment and minimal pain, non-operative management can yield satisfactory outcomes. Revision surgery or arthroplasty should be reserved for symptomatic non-union, progressive varus collapse, or acetabular perforation.
Technical and Preventive Aspects to minimize PFNA mechanical failures, the following technical recommendations are reinforced by literature evidence:
- (i). Achieve near-anatomical or slight valgus reduction to provide a cortical buttress and prevent uncontrolled blade sliding [13]
- To minimize both cut-out and cut-in risks, optimal blade placement in center–center or inferior–center positions with TAD ≈ 20–25 mm is critical [16]
- Confirm mechanical locking intraoperatively through tactile and fluoroscopic verification of the blade–nail engagement
- Reduce cyclic load transmission to the coupling interface by delaying full weight-bearing in cases of severe osteoporosis until a radiographic sign of callus formation appears [17].
This report adds to the limited literature on rare mechanical failures of PFNA, highlighting that uncoupling of the helical blade – though exceedingly rare – can occur even with proper reduction and placement. It highlights that, even in the presence of such mechanical failure, if fracture alignment and function are maintained, conservative treatment can have satisfactory outcomes in selected elderly patients. It emphasizes the need for careful intraoperative assembly verification, post-operative monitoring, and individualized rehabilitation. Conservative management after such failure can produce satisfactory results with stable alignment without the need for revision arthroplasty.
Although PFN is an excellent system for the management of fractures around the hip, it is not bereft of mechanical failures. Careful consideration of the patient’s clinical status and expectations must guide treatment principles.
References
- 1. Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. Osteoporos Int 1997;7:407-13. [Google Scholar] [PubMed]
- 2. Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int 2004;15:897-902. [Google Scholar] [PubMed]
- 3. Geiger F, Zimmermann-Stenzel M, Heisel C, Lehner B, Daecke W. Trochanteric fractures in the elderly: The influence of primary hip arthroplasty on 1-year mortality. Arch OrthopTrauma Surg 2007;127:959-66. [Google Scholar] [PubMed]
- 4. Niu E, Yang A, Harris AH, Bishop J. Which fixation device is preferred for surgical treatment of intertrochanteric hip fractures in the United States? A survey of orthopaedic surgeons. Clin Orthop Relat Res 2015;473:3647-55. [Google Scholar] [PubMed]
- 5. Al-Yassari G, Langstaff RJ, Jones JW, Al-Lami M. The AO/ASIF proximal femoral nail (PFN) for the treatment of unstable trochanteric femoral fracture. Injury 2002;33:395-9. [Google Scholar] [PubMed]
- 6. Strauss E, Frank J, Lee J, Kummer FJ, Tejwani N. Helical blade versus sliding hip screw for treatment of unstable intertrochanteric hip fractures: A biomechanical evaluation. Injury 2006;37:984-9. [Google Scholar] [PubMed]
- 7. Lobo-Escolar A, Joven E, Iglesias D, Herrera A. Predictive factors for cutting-out in femoral intramedullary nailing. Injury 2010;41:1312-6. [Google Scholar] [PubMed]
- 8. Seyhan M, Turkmen I, Unay K, Ozkut AT. Do PFNA devices and Intertan nails both have the same effects in the treatment of trochanteric fractures? A prospective clinical study. J Orthop Sci 2015;20:1053-61. [Google Scholar] [PubMed]
- 9. Siu AL, Penrod JD, Boockvar KS, Koval K, Strauss E, Morrison RS. Early ambulation after hip fracture: Effects on function and mortality. Arch Intern Med 2006;166:766-71. [Google Scholar] [PubMed]
- 10. Cohn MR, Cong GT, Nwachukwu BU, Patt ML, Desai P, Zambrana L, et al. Factors associated with early functional outcome after hip fracture surgery. Geriatr Orthop Surg Rehabil 2016;7:3-8. [Google Scholar] [PubMed]
- 11. Liu W, Zhou D, Liu F, Weaver MJ, Vrahas MS. Mechanical complications of intertrochanteric hip fractures treated with trochanteric femoral nails. J Trauma Acute Care Surg 2013;75:304-10. [Google Scholar] [PubMed]
- 12. Simmermacher RK, Bosch AM, Van Der Werken C. The AO/ASIF-proximal femoral nail (PFN): A new device for the treatment of unstable proximal femoral fractures. Injury 1999;30:327-32. [Google Scholar] [PubMed]
- 13. Bojan AJ, Beimel C, Taglang G, Collin D, Ekholm C, Jönsson A. Critical factors in cut-out complication after Gamma nail treatment of proximal femoral fractures. BMC Musculoskelet Disord 2013;14:1. [Google Scholar] [PubMed]
- 14. Kumar N, Srivastava MP. Screw versus helical proximal femoral nail in the treatment of unstable trochanteric fractures in the elderly. J Clin Orthop Trauma 2019;10:779-84. [Google Scholar] [PubMed]
- 15. Yam M, Kang BJ, Chawla A, Zhang W, Way LG, Xavier RP, et al. Cephalomedullary blade cut-ins: A poorly understood phenomenon. Arch Orthop Trauma Surg 2020;140:1939-45. [Google Scholar] [PubMed]
- 16. Chen XK, Xiong J, Liu YJ, Han Q, Wang TB, Zhang DY, et al. A rare complication of pelvic perforation by an excessive medial slide of the helical blade after treatment of an intertrochanteric fracture with proximal femoral nail anti-rotation: A case report and literature review. Chin J Traumatol 2022;25:118-21. [Google Scholar] [PubMed]
- 17. Angelini M, McKee MD, Waddell JP, Haidukewych G, Schemitsch EH. Salvage of failed hip fracture fixation. J Orthop Trauma 2009;23:471-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 6, 2024 Mechanical Failure of SIGMA Total Condylar-III Revision Total Knee System Modular Femoral Component Due to Bolt Screw Breakage – Our Experience in Overcoming Broken Component Incarceration
August 6, 2024 Mechanical Failure of SIGMA Total Condylar-III Revision Total Knee System Modular Femoral Component Due to Bolt Screw Breakage – Our Experience in Overcoming Broken Component Incarceration October 10, 2023 Proximal Femur Endoprosthesis Augmentation with Polymethylmethacrylate and Condylar Plate: A Case Series
October 10, 2023 Proximal Femur Endoprosthesis Augmentation with Polymethylmethacrylate and Condylar Plate: A Case Series August 10, 2022 Buttress Plate Assisted Fixation for Bicondylar Hoffa Fracture: A Missed Fracture-case Report with Review of Literature
August 10, 2022 Buttress Plate Assisted Fixation for Bicondylar Hoffa Fracture: A Missed Fracture-case Report with Review of Literature June 1, 2026 Influence of Menopause Onset on the Progression of Lumbar Degenerative Disease: A Clinical Correlation Study
June 1, 2026 Influence of Menopause Onset on the Progression of Lumbar Degenerative Disease: A Clinical Correlation Study