
Recurrent knee swelling or hemarthrosis, even in the presence of established diagnoses, should prompt consideration of vascular causes, such as genicular artery pseudoaneurysm and early vascular imaging to avoid diagnostic delay.
Dr. Nizaj Nasimudeen, Department of Orthopaedics, Apollo Adlux Hospital, Kochi, Kerala, India. E-mail: drnizaj239@gmail.com
Abstract
Introduction: Recurrent knee swelling in elderly or anticoagulated patients is commonly attributed to conditions, such as deep vein thrombosis (DVT), Baker’s cyst rupture, septic arthritis, or anticoagulation-related hemarthrosis. However, vascular causes, such as genicular artery pseudoaneurysm, are rare and may be overlooked, especially when symptoms persist despite appropriate treatment.
Case Report: We describe a 60-year-old male with multiple comorbidities who presented with recurrent painful swelling of the right knee. Initial evaluations identified sequential pathologies, including popliteal DVT, ruptured Baker’s cyst, and septic arthritis, all treated appropriately. Despite resolution of infection and withdrawal of anticoagulation, hemarthrosis recurred. Further evaluation with Doppler ultrasonography and magnetic resonance angiography revealed a pseudoaneurysm of the superior medial genicular artery. The lesion was successfully treated using ultrasound-guided compression, resulting in complete thrombosis and resolution of symptoms without complications.
Conclusion: Superior medial genicular artery pseudoaneurysm is a rare but important cause of recurrent hemarthrosis. Persistent or unexplained knee swelling should prompt early vascular imaging to avoid diagnostic delay and enable timely, minimally invasive management.
Keywords: Pseudoaneurysm, genicular artery, recurrent knee swelling, hemarthrosis, ultrasound-guided compression.
Knee swelling is a common presentation in elderly patients and may arise from degenerative, inflammatory, cystic, infectious, or vascular causes. Ruptured Baker’s cysts frequently mimic deep vein thrombosis (DVT), while septic arthritis remains a critical diagnosis because of its potential for rapid joint destruction. In anticoagulated patients, spontaneous hemarthrosis is another well-recognized cause, often complicating the clinical picture [1]. However, vascular etiologies, such as pseudoaneurysms, are extremely rare and can be easily overlooked. They may follow trauma, iatrogenic injury from arthroscopy or arthrocentesis, or occur in the setting of infection and anticoagulation [2]. Because their features are often non-specific and overlap with more common conditions, diagnosis is frequently delayed unless vascular imaging is pursued. We present a diagnostically complex case of recurrent knee swelling in a patient with multiple comorbidities who sequentially developed DVT, ruptured Baker’s cyst, and septic arthritis, with the ultimate diagnosis being a pseudoaneurysm of the superior medial genicular artery. This case highlights the importance of maintaining a broad differential and considering vascular causes when hemarthrosis recurs despite appropriate treatment.
A 60-year-old male with a history of diabetes, hypertension, hypothyroidism, and coronary artery disease presented with acute painful swelling of the right knee. Clinical examination revealed diffuse swelling, tenderness over the knee joint and leg, and fullness in the popliteal fossa. Initial Doppler ultrasonography demonstrated a DVT of the right popliteal vein, and anticoagulation was initiated, leading to partial resolution of limb edema, although the knee swelling persisted. Subsequent magnetic resonance imaging (MRI) of the knee revealed a ruptured Baker’s cyst with a large joint effusion. Arthrocentesis yielded yellow, turbid synovial fluid, which cultured Staphylococcus aureus. The patient underwent arthroscopic lavage, Baker’s cyst decompression, and synovial biopsy. Histopathology and culture confirmed septic arthritis, and he was treated with intravenous culture-sensitive cephalosporin, resulting in symptomatic improvement and normalization of inflammatory markers. Three weeks later, the patient again presented with painful knee swelling. Aspiration at this stage revealed hemarthrosis, but cultures were sterile. The swelling decreased when anticoagulation was withheld, suggesting a possible anticoagulation-related bleed. However, a third episode of acute hemarthrosis occurred despite cessation of anticoagulation, raising suspicion of a vascular cause. Initial MRI of the knee demonstrated a periarticular lesion (Fig. 1), and Doppler ultrasonography suggested a vascular etiology (Fig. 2).
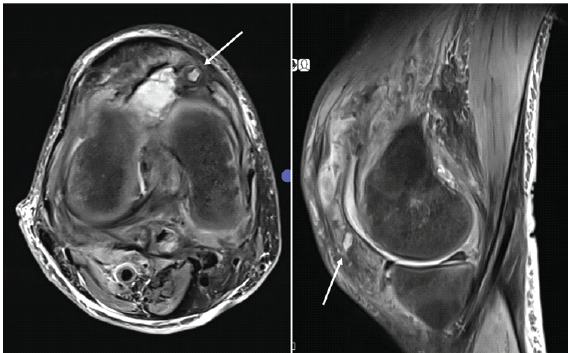
Figure 1: Axial and sagittal T2-weighted magnetic resonance images of the right knee showing a periarticular lesion adjacent to the joint capsule (white arrow).
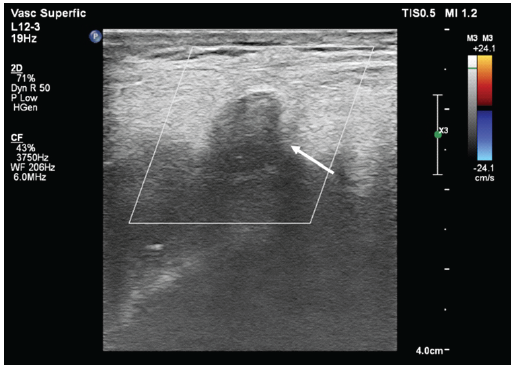
Figure 2: Doppler ultrasonography of the right knee demonstrating a well-defined periarticular vascular lesion with internal turbulent flow, consistent with a pseudoaneurysm (white arrow).
In this case, the pseudoaneurysm measured 10 × 8 mm with a narrow 2.7 mm neck, and Doppler demonstrated the classical “Yin-Yang” sign, confirming turbulent bidirectional flow and suitability for compression therapy. Magnetic resonance angiography subsequently confirmed a pseudoaneurysm arising from the superior medial genicular artery adjacent to the joint capsule (Fig. 3).
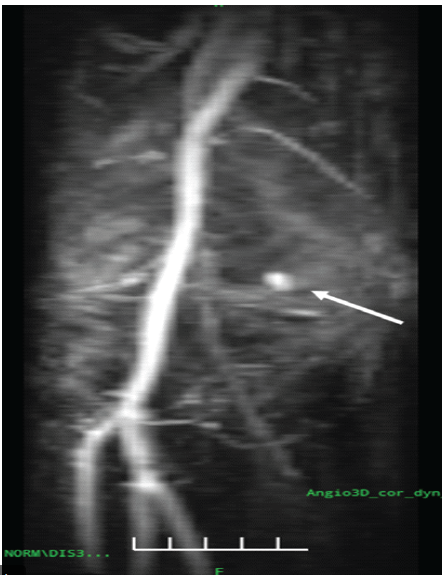
Figure 3: Magnetic resonance angiography of the right knee demonstrating a saccular pseudoaneurysm arising from the superior medial genicular artery adjacent to the joint capsule, with preserved popliteal artery flow (white arrow).
The patient was referred to the interventional radiology team and managed with ultrasound-guided compression. A high-frequency 7–12 MHz linear transducer was used, and sustained probe compression was applied directly over the pseudoaneurysm neck in approximately 30-min cycles under real-time Doppler guidance, with intermittent assessment of intralesional flow. After two sessions, complete disappearance of color flow within the sac was observed, confirming successful thrombosis of the pseudoaneurysm, which was subsequently replaced by an echogenic hematoma (Fig. 4).
Follow-up computed tomography (CT) angiography at 24 h showed complete obliteration of the lesion with preservation of distal arterial flow (Fig. 5).
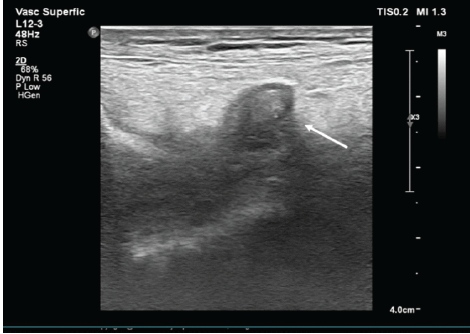
Figure 4: Post–ultrasound-guided compression grayscale ultrasonography of the right knee demonstrating an echogenic thrombus within the pseudoaneurysm sac, indicating successful thrombosis and obliteration of the lesion (white arrow).
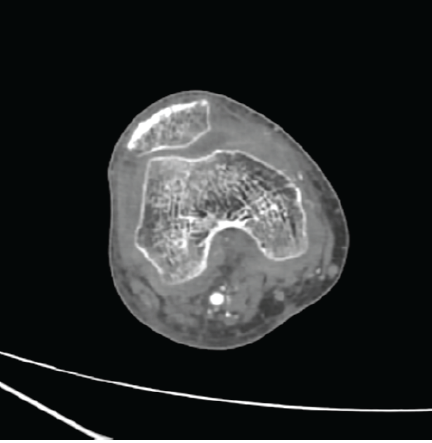
Figure 5: Computed tomography angiography of the right knee performed 24 h after ultrasound-guided compression demonstrating complete obliteration of the superior medial genicular artery pseudoaneurysm, with no residual contrast filling and preserved distal arterial flow.
The procedure was well tolerated with no complications, such as thrombosis, ischemia, or infection. At 6 months of follow-up, the patient remained asymptomatic, demonstrated no recurrence on imaging, and had regained full functional mobility.
This case underscores the diagnostic complexity of recurrent knee swelling in an elderly patient with multiple comorbidities and ongoing anticoagulation. Each of the initial conditions – DVT, ruptured Baker’s cyst, and septic arthritis – was a genuine and well-supported diagnosis. However, the persistence of hemarthrosis despite appropriate treatment highlighted that more than one pathology could sequentially contribute to the clinical picture. A key learning point is the risk of anchoring bias, where clinicians may pre-maturely attribute new or ongoing symptoms to an already established diagnosis. In this patient, recurrent hemarthrosis was initially attributed to anticoagulation, but persistence despite cessation of therapy mandated further evaluation. The eventual discovery of a superior medial genicular artery pseudoaneurysm emphasizes the importance of maintaining diagnostic vigilance when the clinical course deviates from expectations. Pseudoaneurysms develop after partial disruption of the arterial wall, with blood dissecting into surrounding tissues and forming a cavity that is walled off by fibrous tissue rather than true vessel layers [3]. Turbulent flow is often demonstrable within the sac on Doppler ultrasonography. Over time, these lesions may enlarge, with risks of rupture, infection, skin necrosis, erosion into adjacent structures, distal limb ischemia, or compression neuropathy [4]. While idiopathic cases exist, iatrogenic causes are particularly important in the knee. Minor arterial injury may occur during arthroscopy or arthrocentesis, especially near the anteromedial and anterolateral access portals that are close to the superior genicular arteries. Although rare, such vascular complications should be suspected when recurrent hemarthrosis occurs after instrumentation [2]. The classical findings include a painful, enlarging, pulsatile mass with associated bruit or palpable thrill, though deep pseudoaneurysms may present only with recurrent hemarthrosis [5,6]. Doppler ultrasonography can identify turbulent flow, while CT angiography remains the gold standard for diagnosis and pre-procedural planning [7]. Management depends on size, accessibility, and patient tolerance. Ultrasound-guided compression repair (UGCR) involves applying probe pressure until flow within the pseudoaneurysm ceases, inducing thrombosis and hematoma organization. This approach is simple and non-invasive, though limitations include severe tenderness, overlying infection, large or calcified hematomas, and critical limb ischemia [8]. Success rates are higher in lesions under 3–4 cm; Coley et al. reported technical success in 87% of pseudoaneurysms ≤4 cm, compared to 62% when larger [9], with similar findings from Eisenberg et al. [10]. In cases unsuitable for compression, adjunctive thrombin injection or endovascular embolization provides effective alternatives, while surgical repair is reserved for complex or refractory lesions [11]. In our patient, ultrasound-guided compression successfully achieved obliteration of the superior medial genicular artery pseudoaneurysm, with complete resolution of symptoms and preservation of distal perfusion. This case highlights the diagnostic complexity of recurrent knee swelling in an elderly patient with multiple comorbidities and ongoing anticoagulation. Each of the initial diagnoses – DVT, ruptured Baker’s cyst, and septic arthritis – was genuine and well supported. However, the persistence of hemarthrosis despite appropriate management indicated that multiple sequential pathologies could coexist and contribute to the clinical presentation. A major diagnostic pitfall in such scenarios is anchoring bias, where ongoing or new symptoms are attributed to an already established diagnosis. In this patient, recurrent hemarthrosis was initially considered secondary to anticoagulation; however, persistence despite cessation of therapy prompted further evaluation. The identification of a superior medial genicular artery pseudoaneurysm underscored the importance of maintaining diagnostic vigilance when the clinical course deviates from expectations. Pseudoaneurysms result from partial disruption of the arterial wall, allowing blood to extravasate into surrounding tissues and form a cavity bounded by fibrous tissue rather than true vessel layers [3]. Turbulent flow within the sac is commonly demonstrable on Doppler ultrasonography. Over time, these lesions may enlarge and lead to complications, such as rupture, infection, skin necrosis, erosion into adjacent structures, distal limb ischemia, or compression neuropathy [4]. Although idiopathic pseudoaneurysms are reported, iatrogenic causes are particularly relevant around the knee. Minor arterial injury may occur during arthroscopy or arthrocentesis, especially near the anteromedial and anterolateral portals that lie close to the superior genicular arteries. In this patient, the exact etiology could not be definitively established; possibilities include occult arterial trauma during arthrocentesis or arthroscopy, vessel-wall weakening from septic arthritis, or propagation of an arterial defect facilitated by anticoagulation, suggesting a multifactorial origin. The classical findings may include a painful, enlarging, pulsatile mass with an associated bruit or thrill; however, deeply situated pseudoaneurysms may present solely with recurrent hemarthrosis [5,6]. A structured differential diagnosis for recurrent hemarthrosis includes infection, crystal arthropathy, anticoagulation-related bleeding, meniscal or ligament injury, synovial neoplasms, such as pigmented villonodular synovitis, vascular tumors, and arterial injuries, including pseudoaneurysm or arteriovenous fistula. Doppler ultrasonography serves as a useful screening tool by demonstrating turbulent flow, while CT angiography remains the gold standard for definitive diagnosis and procedural planning [7]. Management depends on lesion size, accessibility, and patient tolerance. UGCR is a simple, non-invasive technique that induces thrombosis by occluding flow at the pseudoaneurysm neck. Limitations include severe tenderness, overlying infection, large or calcified hematomas, and critical limb ischemia [8]. Reported success rates are higher in lesions smaller than 3–4 cm, with reduced success in larger pseudoaneurysms [9,10]. Alternative modalities include ultrasound-guided thrombin injection, which enables rapid thrombosis; endovascular embolization using coils or particles, which offers durable exclusion with high technical success; and open surgical repair, reserved for infected, wide-neck, or refractory lesions [11]. In this case, ultrasound-guided compression successfully achieved obliteration of the superior medial genicular artery pseudoaneurysm, resulting in complete symptom resolution and preservation of distal arterial perfusion. While this favorable outcome is notable, single-case reports have limited generalizability. Even so, the case supports the notion that early incorporation of vascular imaging in selected presentations can be cost-effective by reducing repeat evaluations, minimizing delays in diagnosis, and avoiding the higher procedural costs associated with embolization or operative management. This case also reinforces the importance of multidisciplinary collaboration among orthopaedics, radiology, and interventional specialists when evaluating complex and recurrent knee swelling.
Multiple sequential causes may coexist in recurrent knee swelling, particularly in high-risk patients. Pseudoaneurysm should be suspected when hemarthrosis recurs despite appropriate infection control and anticoagulation adjustment. Early vascular imaging and multidisciplinary collaboration are essential to prevent complications and enable timely diagnosis and management. By recognizing these principles, clinicians can avoid diagnostic delay and ensure that rare but treatable vascular complications are promptly identified and managed.
Recurrent hemarthrosis should prompt evaluation for vascular causes, such as genicular artery pseudoaneurysm, especially in anticoagulated patients or after knee procedures, as early diagnosis allows effective minimally invasive treatment and prevents diagnostic delay.
References
- 1. Filho ES, Isolani GR, Baracho FR, De Oliveira Franco AP, Ridder Bauer LA, Namba M. Pseudoaneurysm after arthroscopic procedure in the knee. Rev Brasil Ortopedia 2015;50:131-5. [Google Scholar] [PubMed]
- 2. Ho CW, Lee SH, Wu SH, Lin CY, Lee CH, Wu JL. Pseudoaneurysm following hamstring tendon harvest in arthroscopic anterior cruciate ligament reconstruction: A case report. BMC Musculoskelet Disord 2020;21:697. [Google Scholar] [PubMed]
- 3. Gliatis JD, Papagiannis SL, Sinos GV, Argyropoulou ED, Kotsia CV. Pseudoaneurysm of the superior lateral genicular artery of the knee following arthroscopic irrigation and debridement and review of literature. Indian J Orthop 2022;57:159-62. [Google Scholar] [PubMed]
- 4. Glanz L. Pseudaneurysm of the superolateral genicular artery following an anterior cruciate ligament reconstruction. Int J Surg Case Rep 2020;72:628-31. [Google Scholar] [PubMed]
- 5. Oversier LM, Corten BJ, Barten DG, Elshof JW. Pseudoaneurysm of the superior lateral genicular artery following anterior cruciate ligament repair. Acta Chir Belg 2018;118:258-63. [Google Scholar] [PubMed]
- 6. Alammari N, Ananthan B, Alotaibi S, Asiri Y, Mohammed M, Almulla A. A rare presentation of pseudoaneurysm of the popliteal artery after total knee replacement: A case report and review of the literature. Cureus 2024;16:e65772. [Google Scholar] [PubMed]
- 7. Daniels SP, Sneag DB, Berkowitz JL, Trost D, Endo Y. Pseudoaneurysm after total knee arthroplasty: Imaging findings in 7 patients. Skeletal Radiol 2019;48:699-706. [Google Scholar] [PubMed]
- 8. Huang TL, Liang HL, Huang JS, Yang TL, Chen YJ, Huang PY, et al. Ultrasound-guided compression repair of peripheral artery pseudoaneurysm: 8 years’ experience of a single institute. J Chin Med Assoc 2012;75:468-73. [Google Scholar] [PubMed]
- 9. Coley BD, Roberts AC, Fellmeth BD, Valji K, Bookstein JJ, Hye RJ. Postangiographic femoral artery pseudoaneurysms: Further experience with US-guided compression repair. Radiology 1995;194:307-11. [Google Scholar] [PubMed]
- 10. Eisenberg L, Paulson EK, Kliewer MA, Hudson MP, DeLong DM, Carroll BA. Sonographically guided compression repair of pseudoaneurysms: Further experience from a single institution. AJR Am J Roentgenol 1999;173:1567-73. [Google Scholar] [PubMed]
- 11. Rashaideh MA, Janho KE, Shawaqfeh JS, Ajarmeh E, As’ad M. Ultrasound-guided thrombin injection versus ultrasound-guided compression therapy of iatrogenic femoral false aneurysms: Single center experience. Med J Armed Forces India 2020;76:293-7. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 10, 2022 Pseudoaneurysm of the Lateral Genicular Artery Following Unicompartmental knee Arthroplasty: A Rare Case Report
August 10, 2022 Pseudoaneurysm of the Lateral Genicular Artery Following Unicompartmental knee Arthroplasty: A Rare Case Report June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report
June 1, 2026 Pseudoaneurysm of the Medial Femoral Circumflex Artery following Surgical Fixation of Trochanteric Femur Fracture: A Case Report June 1, 2026 Delayed Pseudoaneurysm of the Subclavian Artery Following Clavicle Fracture Fixation: A Case Report
June 1, 2026 Delayed Pseudoaneurysm of the Subclavian Artery Following Clavicle Fracture Fixation: A Case Report November 1, 2025 Anterior Tibial Artery Pseudoaneurysm Following Arthroscopic Ankle Arthrodesis: A Case Report
November 1, 2025 Anterior Tibial Artery Pseudoaneurysm Following Arthroscopic Ankle Arthrodesis: A Case Report