
CT-based four-column classification of tibial plateau fractures improves detection of posterior fragments and guides column-specific fixation strategies, leading to improved functional outcomes.
Dr. Safia Sultana, Department of Orthopaedics, Nizam’s Institute of Medical Sciences, Hyderabad, Telangana, India. E-mail: sultanasafia2017@gmail.com
Abstract
Introduction: Proximal tibial plateau fractures are complex intra-articular injuries with significant implications for knee function. Conventional classification systems, such as the Schatzker classification, are limited in their ability to identify posterior column involvement. The modified Schatzker four-column concept, based on computed tomography (CT), provides a more comprehensive understanding of fracture morphology and may improve surgical planning and outcomes. This study aims to evaluate the utility of the four-column concept in guiding management and its association with functional outcomes.
Materials and Methods: This prospective observational study was conducted at a tertiary care center between January 2024 and April 2025. Thirty skeletally mature patients with closed proximal tibial plateau fractures were included. All fractures were classified using CT-based modified Schatzker (four-column) classification. Surgical management was tailored based on column involvement using appropriate approaches and fixation strategies, including single or dual plating. Functional outcomes were assessed using the Knee Society Score (KSS) and Modified Rasmussen Functional Score. Radiological union and complications were also evaluated over a minimum follow-up of 6 months.
Results: The most common fracture pattern was anterolateral (AL) with posterolateral (PL) involvement (AL + PL) which was observed in 10 patients (33.3%), followed by other two-column injuries, while four-column fractures accounted for 20%. All fractures achieved union at a mean of 14.2 weeks. Functional outcomes were predominantly good to excellent, with mean KSS ranging from 75 to 90 and Rasmussen scores from 20 to 28. Four-column fractures demonstrated higher mean Rasmussen scores (27.0) compared to two-column fractures (24.2). Functional outcomes showed a significant association with fracture morphology (KSS P = 0.021; Rasmussen P = 0.008). Dual plating yielded significantly better outcomes than single plating (P < 0.05). Complications were minimal, with 86.7% of patients having an uneventful recovery.
Conclusion: The four-column concept is a valuable tool in the management of proximal tibial plateau fractures. It facilitates accurate fracture characterization, guides surgical approach, and is associated with favorable functional outcomes, particularly when combined with column-specific fixation strategies such as dual plating.
Keywords: Tibial plateau fracture, four-column concept of proximal tibia injuries, modified Schatzker classification, functional outcome, dual plating for proximal tibia fractures.
Intra-articular proximal tibial fractures continue to represent a significant challenge in orthopedic trauma. These fractures account for approximately 1% of all fractures and up to 8% in the elderly population, with a bimodal age distribution involving high-energy trauma in younger individuals and low-energy osteoporotic fractures in older patients [1]. The knee joint, being a major weight-bearing articulation with intricate ligamentous and osseous anatomy, is particularly susceptible to functional impairment following such injuries [2]. The primary goals in the management of proximal tibial fractures include restoration of articular congruity, maintenance of mechanical alignment, preservation of joint stability, and early mobilization [3]. Failure to achieve these objectives can result in complications such as malunion, instability, stiffness, and early onset osteoarthritis. Historically, non-operative management was widely practiced; however, it was associated with poor functional outcomes due to prolonged immobilization and inadequate restoration of joint anatomy. Advances in surgical techniques and fixation methods have shifted the treatment paradigm toward operative management, emphasizing anatomical reduction and stable fixation [4]. The Schatzker classification, introduced in 1979, has been the cornerstone for categorizing tibial plateau fractures [5]. While it provides a useful framework based on fracture morphology seen on plain radiographs, it is limited by its two-dimensional perspective and inability to adequately represent posterior column involvement. With the advent of computed tomography (CT) and three-dimensional imaging, it has become evident that many fractures extend into the posterior columns, which are often missed on conventional radiographs [6]. This has led to the development of the modified Schatzker classification – a four-column concept, which divides the proximal tibia into anteromedial (AM), AL, posteromedial (PM), and posterolateral (PL) columns, allowing for a more precise understanding of fracture anatomy [4,7].
The four-column concept emphasizes the importance of rim stability and column-specific fixation in achieving optimal outcomes [4,7]. Posterior column involvement, particularly PM fragments, plays a crucial role in maintaining knee stability and must be addressed surgically [8]. Despite its growing acceptance, there remains limited data evaluating the usefulness of this classification system. This study aims to assess the functional and radiological outcomes of proximal tibial fractures that were managed by analyzing the injuries based on the four-column concept and to evaluate its utility in guiding the surgical management.
This prospective observational study was conducted in the department of Orthopedics at a Level-I tertiary center during January 2024–April 2025. The primary aim of the study was to evaluate the functional outcomes of proximal tibial plateau fractures treated surgically using the modified Schatzker (four-column) classification system. The specific objectives were to classify fractures using CT-based modified Schatzker classification, determine the distribution of column involvement, evaluate functional outcomes using standardized scoring systems, and assess complications associated with surgical management.
A total of 30 patients with proximal tibial plateau fractures were included in the study. All patients were skeletally mature individuals aged above 18 years who sustained closed fractures of the proximal tibia and were managed surgically. Only patients who were willing to participate in regular follow-up were included. Patients with open fractures, vascular injuries, pathological fractures, severe medical comorbidities contraindicating surgery, and those lost to 6-month follow-up were excluded from the study.
Institutional Ethics Committee approval was obtained before commencement of the study (No: 3664/2025), and informed written consent was obtained from all patients participating in the study.
All patients underwent a detailed pre-operative clinical and radiological evaluation. Standard radiographs of the knee, including anteroposterior and lateral views, were obtained in all cases. This was supplemented by CT scans with three-dimensional reconstruction to accurately delineate fracture morphology. Fractures were classified according to the modified Schatzker classification based on the four-column concept. This system allowed identification of involvement of the anterolateral (AL), PL, AM, and PM columns, thereby facilitating a comprehensive understanding of fracture patterns and aiding surgical planning.
Surgical management was planned based on the column involvement identified on imaging. An AL approach was utilized for fractures involving the lateral column, while PM fractures were addressed using a PM approach. In cases of bicondylar or multi-column fractures, combined surgical approaches were employed to achieve optimal visualization and fixation. Internal fixation was performed using locking compression plates, dual plating techniques, or buttress plates depending on fracture configuration and stability requirements. Care was taken to achieve anatomical reduction of the articular surface and restore mechanical alignment.
Postoperatively, all patients were managed with a standardized rehabilitation protocol. Early knee mobilization was initiated to prevent joint stiffness and promote functional recovery. Weight-bearing was gradually introduced based on fracture stability and radiological evidence of healing. Patients were monitored regularly in the outpatient setting.
Functional outcomes were assessed using validated scoring systems, including the Knee Society Score (KSS) and the Rasmussen functional score. Radiological assessment was performed to evaluate fracture union and maintenance of reduction. Patients were followed up for a minimum duration of 6 months postoperatively. Complications such as infection, knee stiffness, delayed union, and implant-related issues were documented and analyzed.
A total of 30 patients with proximal tibial plateau fractures were included in this prospective study and followed for a minimum duration of 6 months. The majority of patients were in the fourth and fifth decades of life, with the highest incidence observed in the 41–50 years age group (26.7%). There was a marked male predominance, with 26 male patients (86.7%) and 4 female patients (13.3%). Road traffic accidents were the most common mechanism of injury, accounting for 26 cases (86.7%), while falls from height accounted for 4 cases (13.3%).
Fractures were classified using the CT-based modified Schatzker (four-column) classification. The most common fracture pattern was combined AL and PL involvement (AL + PL), which was observed in 10 patients (33.3%). This was followed by combined AM and AL involvement (AM + AL) in 8 patients (26.7%), AL and PM involvement (AL + PM) in 6 patients (20.0%), and four-column fractures involving all columns in 6 patients (20.0%). When grouped according to the number of involved columns, AL + PL, AM + AL, and AL + PM each represented two-column injuries.
All fractures progressed to radiological union. The majority of fractures united between 12 and 16 weeks (mean 14.2 weeks). No case of delayed union or nonunion was encountered during the follow-up period.
Functional outcomes were assessed using the KSS and Modified Rasmussen Functional Score. Overall, the majority of patients achieved good to excellent outcomes at final follow-up. Mean KSS values ranged from 75 to 90, while Modified Rasmussen scores ranged from 20 to 28. When functional outcomes were analyzed according to fracture complexity, the mean Modified Rasmussen score was 24.2 for two-column fractures and 27.0 for four-column fractures. A statistically significant association was observed between fracture morphology and functional outcome. KSS differed significantly between fracture patterns (P = 0.021), and the Modified Rasmussen score also demonstrated a significant association with fracture morphology (P = 0.008). Functional outcome was further analyzed according to the fixation method employed. Patients managed with dual plating had superior functional outcomes compared with those managed with single plating (Fig. 1).
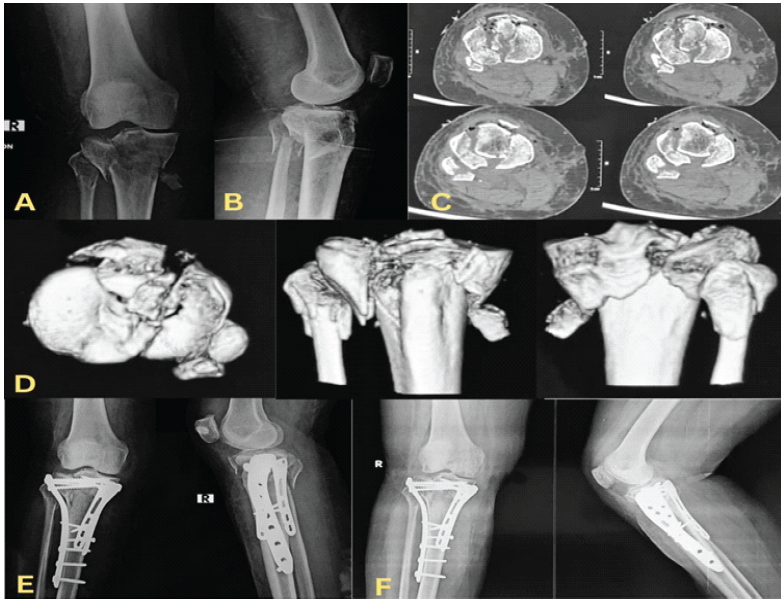
Figure 1:Representative case of a type V anterolateral (AL) + posterolateral (PL) + anteromedial (AM) + posteromedial (PM) four-column proximal tibial plateau fracture treated with column-specific fixation (triple plating). (a) Pre-operative anteroposterior radiograph, (b) lateral radiograph, (c) axial computed tomography (CT) scan demonstrating involvement of the AL, PL, AM, and PM columns, (d) three-dimensional CT reconstruction images, (e) post-operative
radiograph following triple plating fixation, (f) 6-month follow-up radiograph showing fracture union and maintenance of reduction.
The mean KSS in the dual plating group was 85.6, compared with 78.2 in the single plating group. Similarly, the mean Modified Rasmussen score was 27.3 in the dual plating group and 23.4 in the single plating group. These differences were statistically significant (KSS: P = 0.034; Modified Rasmussen score: P = 0.019).
Most patients had an uncomplicated post-operative course. Twenty-six patients (86.7%) had no recorded complication. Superficial wound infection occurred in 2 patients (6.7%) where they required serial debridement only, knee stiffness in 1 patient (3.3%) with range of motion restricted to 70° of flexion, and implant exposure in 1 patient (3.3%) that required flap cover.
The management of proximal tibial plateau fractures continues to evolve with advances in imaging, surgical techniques, and fixation strategies. With the introduction of the three-column concept for proximal tibial fractures, the biomechanical understanding of posterior column fixation evolved. However, the original three-column system did not fully characterize depression and rim injuries involving the posterior articular surface, leading to the subsequent development of the CT-based modified Schatzker four-column concept [9,10]. This system guides the management of proximal tibial injuries by aiding the selection of the surgical approach and fixation strategy appropriate for the respective fracture morphology. The present prospective observational study evaluates the role of the modified Schatzker four-column concept in guiding surgical management and its impact on functional outcomes. The findings demonstrate that CT-based column-specific fracture assessment enables more precise surgical planning and is associated with favorable functional outcomes, reliable fracture union, and a low complication rate. These results reinforce the growing consensus that three-dimensional understanding of fracture morphology is critical in optimizing outcomes in these complex injuries.
Tibial plateau fractures represent a spectrum of injuries ranging from low-energy osteoporotic fractures to high-energy trauma with significant comminution and soft tissue compromise. Traditional classification systems, particularly the Schatzker classification, have long been used for categorization and treatment planning. However, their reliance on two-dimensional radiographs limits their ability to accurately depict complex fracture patterns, especially those involving the posterior columns. Recent literature has emphasized the importance of CT-based evaluation in improving fracture characterization, with studies demonstrating that conventional radiographs frequently underestimate posterior involvement [9,10,11]. The four-column concept addresses this limitation by dividing the proximal tibia into AL, AM, PL, and PM columns, thereby offering a more comprehensive and clinically relevant framework for fracture assessment.
In the present study, the most common fracture pattern was combined AL and PL involvement, followed by other two-column injuries, while four-column fractures constituted 20% of cases. This pattern distribution is consistent with recent reports, which highlight the predominance of lateral column fractures due to valgus forces while also recognizing the increasing incidence of posterior column injuries in high-energy trauma [10,12]. Posterior column fractures, particularly those involving the PM fragment, are of significant biomechanical importance. The PM fragment acts as a key stabilizer against varus forces and contributes to the overall stability of the knee joint. Failure to adequately address this fragment has been associated with residual instability, malalignment, and inferior functional outcomes [13]. The routine use of CT scans in this study ensured accurate identification of such fragments, facilitating appropriate surgical intervention.
A notable finding of this study is the statistically significant association between fracture morphology and functional outcomes, as assessed by KSS and Modified Rasmussen Functional Score. Interestingly, patients with four-column fractures demonstrated higher Rasmussen scores compared to those with two-column injuries. While intuitively more complex fractures might be expected to yield poorer outcomes, this observation likely reflects the benefits of meticulous pre-operative planning and comprehensive fixation strategies employed in these cases. Recent studies have similarly reported that when complex fractures are managed with a structured, column-specific approach, outcomes can be comparable to or even better than less complex injuries due to improved anatomical reduction and stability [11,14].
The importance of fixation strategy is further underscored by the superior functional outcomes observed in patients treated with dual plating compared to single plating. Dual plating provides enhanced biomechanical stability by addressing both medial and lateral columns, particularly in bicondylar and multi-column fractures. Contemporary biomechanical and clinical studies have demonstrated that dual plating results in better maintenance of reduction, reduced risk of varus collapse, and improved functional outcomes compared to single lateral plating alone [15,16]. In the present study, patients managed with dual plating achieved significantly higher KSS and Rasmussen scores, supporting these findings. The ability of the four-column concept to guide the selection of appropriate fixation techniques is therefore of considerable clinical relevance.
In addition to the fixation strategy, the choice of surgical approach plays a critical role in achieving optimal outcomes. The four-column concept facilitates a tailored approach based on fracture morphology, allowing direct visualization and reduction of specific fragments. The four-column concept also helped in selecting the Frosch approach in selected cases where the fracture configuration and posterior column involvement were best addressed through this exposure (Fig. 2). PM and PL approaches, in particular, have gained popularity for addressing posterior column fractures. Studies published in recent years have demonstrated that these approaches enable more accurate reduction and stable fixation of posterior fragments compared to indirect methods, which often result in suboptimal outcomes [12,17]. In the present study, the use of combined approaches in multi-column fractures contributed to effective fracture reduction and favorable functional recovery.
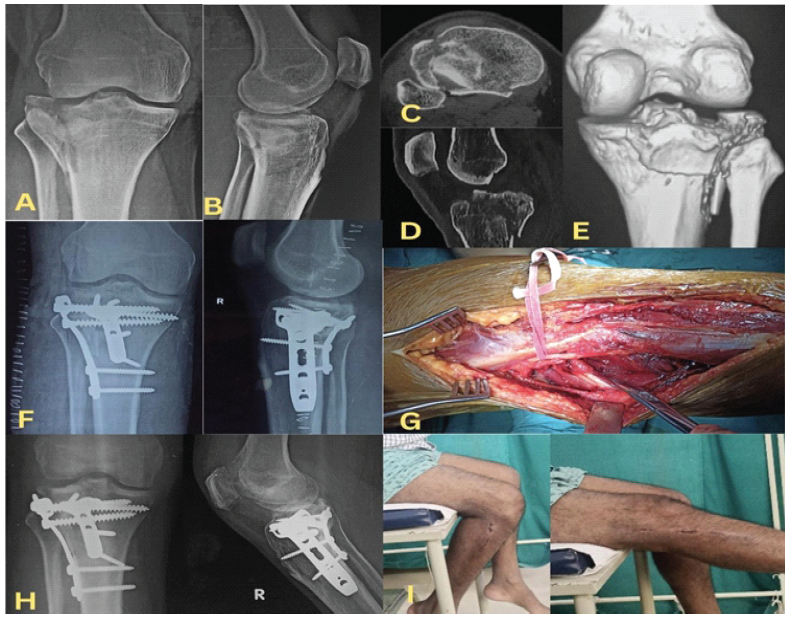
Figure 2: Case example demonstrating a Type II A+P proximal tibial plateau fracture with significant posterolateral column involvement managed using the Frosch approach. (a) Anteroposterior radiograph, (b) lateral radiograph, (c) axial computed tomography (CT) image showing the posterolateral fragment, (d) sagittal CT image, (e) coronal CT reconstruction demonstrating fracture morphology, (f) immediate post-operative radiograph demonstrating stable fixation
and restoration of articular congruity, (g) intraoperative image showing exposure through the Frosch approach, (h) Four-month follow-up radiograph, (i) Four-month follow-up clinical images showing knee range of motion.
Fracture union was achieved in all patients, with a mean union time of 14.2 weeks, which is consistent with previously reported union times in the literature [14,18]. The absence of delayed union or non-union in this cohort may be attributed to stable fixation constructs, careful surgical technique, and adherence to biological principles of fracture healing. Locking compression plates and buttress plating techniques, as utilized in this study, provide angular stability and are particularly advantageous in osteoporotic bone and comminuted fractures. Furthermore, early mobilization protocols, which were uniformly implemented in this study, play a crucial role in promoting joint function and preventing complications such as stiffness.
The complication rate observed in this study was low, with the majority of patients experiencing an uneventful post-operative course. Superficial infections, knee stiffness, and implant-related complications were minimal and manageable. This aligns with contemporary literature, which suggests that advances in surgical techniques, improved implant designs, and better perioperative care have significantly reduced complication rates in tibial plateau fracture management [16,18]. However, it is important to recognize that the risk of complications increases with fracture complexity, soft tissue injury, and the use of extensile surgical approaches. Therefore, careful patient selection, meticulous soft tissue handling, and staged management in high-energy injuries remain essential.
Another important aspect highlighted by this study is the role of early rehabilitation in achieving good functional outcomes. Early knee mobilization, as practiced in this study, helps prevent joint stiffness and promotes cartilage health. Several recent studies have emphasized the importance of early range-of-motion exercises in improving functional recovery and reducing long-term morbidity [18]. The favorable functional outcomes observed in this cohort may, in part, be attributed to the standardized rehabilitation protocol followed postoperatively.
The clinical implications of this study are significant. The four-column concept not only enhances fracture understanding but also directly influences surgical decision-making. By identifying the specific columns involved, surgeons can select appropriate approaches and fixation strategies, thereby improving the likelihood of achieving anatomical reduction and stable fixation. This tailored approach is particularly valuable in complex fractures, where conventional classification systems may be inadequate. The findings of this study add to the growing body of evidence supporting the routine use of CT-based classifications in the management of periarticular fractures [9,11].
Despite its strengths, this study has several limitations. The sample size was relatively small, which may limit the statistical power and generalizability of the findings. In addition, the study was conducted at a single tertiary care center, and the results may therefore reflect institutional expertise and may not be directly applicable to other clinical settings. Inclusion of only surgically treated closed fractures may also have introduced selection bias and does not represent the entire spectrum of proximal tibial plateau injuries. Open fractures and fractures associated with vascular injury were excluded; therefore, the findings may not be applicable to more severe and complex trauma patterns.
The follow-up period of 6 months, although sufficient to assess fracture union and short-term functional outcomes, does not permit evaluation of long-term sequelae such as post-traumatic osteoarthritis, maintenance of reduction, implant longevity, or long-term remodeling. Although fracture union was documented in all patients, detailed quantitative radiological parameters such as residual articular step-off, condylar widening, limb alignment, and restoration of joint congruity were not systematically analyzed. Furthermore, the study did not include a direct comparison group, which would have provided stronger evidence regarding the superiority of CT-based planning. The study cohort also included a heterogeneous mix of fracture patterns, ranging from two-column to four-column injuries, which may have influenced the interpretation of the functional outcomes.
The fixation strategy was not standardized across all patients, with some fractures managed using single plating and others requiring dual or triple plating through different surgical approaches. This variation may have introduced treatment-related bias. In addition, potential variability in surgeon experience, operative decision-making, and technical execution was not assessed and may have influenced the observed outcomes. Functional outcomes were assessed only using the KSS and Modified Rasmussen Functional Score. Finally, complications were not stratified according to fracture severity, fixation method, or surgical approach, and the learning curve associated with application of the four-column concept and posterior or extensile approaches, such as the Frosch approach, was not evaluated.
Future research should focus on larger, multicentric studies with longer follow-up periods to validate these findings and assess long-term outcomes. Comparative studies evaluating the four-column concept against traditional classification systems would also be valuable in establishing its clinical utility. In addition, the integration of advanced technologies such as computer-assisted surgery and patient-specific instrumentation may further enhance the precision of fracture management and improve outcomes.
The present study demonstrates that the four-column concept is a valuable tool in the management of proximal tibial plateau fractures. Its application in pre-operative planning allows for accurate fracture characterization, selection of appropriate surgical approaches, and implementation of stable fixation strategies. Incorporating this classification into routine clinical practice may enhance the management of complex tibial plateau fractures and ultimately improve patient outcomes.
The modified Schatzker four-column concept improves understanding of proximal tibial plateau fractures by identifying posterior column involvement and guiding column-specific fixation. Appropriate surgical approach selection and stable fixation can significantly improve functional outcomes.
References
- 1. Olerud F, Garland A, Hailer NP, Wolf O. Incidence of proximal tibia fractures in adults in Sweden show higher rates in women and a marked increase among young women. Sci Rep 2026;16:6364. [Google Scholar] [PubMed]
- 2. D’Lima DD, Fregly BJ, Patil S, Steklov N, Colwell CW Jr. Knee joint forces: Prediction, measurement, and significance. Proc Inst Mech Eng H 2012;226:95-102. [Google Scholar] [PubMed]
- 3. Kasha S, Yalamanchili RK, Rohit G, Koneru S, Gurram A, Ravi Weera Athili V. Intra-articular and extra-articular malunion of proximal tibia: Assessment and management. J Clin Orthop Trauma 2025;72:103279. [Google Scholar] [PubMed]
- 4. Schatzker J, Kfuri M. Revisiting the management of tibial plateau fractures. Injury 2022;53:2207-18. [Google Scholar] [PubMed]
- 5. Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The toronto experience 1968-1975. Clin Orthop Relat Res 1979;138:94-104. [Google Scholar] [PubMed]
- 6. Charalambous CP, Tryfonidis M, Alvi F, Moran M, Fang C, Samarji R, et al. Inter- and intra-observer variation of the Schatzker and AO/OTA classifications of tibial plateau fractures and a proposal of a new classification system. Ann R Coll Surg Engl 2007;89:400-4. [Google Scholar] [PubMed]
- 7. Mansur H, Corrêa VL, Abdo B, Ramos LS, Castiglia MT. Evaluation of the Reproducibility of the Schatzker classification reviewed by Kfuri for tibial plateau fractures. Rev Bras Ortop (Sao Paulo) 2021;57:502-10. [Google Scholar] [PubMed]
- 8. Yao X, Zhou K, Lv B, Wang L, Xie J, Fu X, et al. 3D mapping and classification of tibial plateau fractures. Bone Joint Res 2020;9:258-67. [Google Scholar] [PubMed]
- 9. Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 2010;24:683-92. [Google Scholar] [PubMed]
- 10. Kfuri M, Schatzker J. Revisiting the Schatzker classification of tibial plateau fractures. Injury 2018;49:2252-63. [Google Scholar] [PubMed]
- 11. Wang Y, Luo C, Zhu Y, Zhai Q, Zhan Y, Qiu W, et al. Updated three-column concept in surgical treatment for tibial plateau fractures – a prospective cohort study of 287 patients. Injury 2016;47:1488-96. [Google Scholar] [PubMed]
- 12. Chang SM, Hu SJ, Zhang YQ, Yao MW, Ma Z, Wang X, et al. A surgical protocol for bicondylar four-quadrant tibial plateau fractures. Int Orthop 2014;38:2559-64. [Google Scholar] [PubMed]
- 13. Sun H, Luo CF, Yang G, Shi HP, Zeng BF. Anatomical evaluation of the modified posterolateral approach for posterolateral tibial plateau fracture. Eur J Orthop Surg Traumatol 2013;23:809-18. [Google Scholar] [PubMed]
- 14. Higgins TF, Klatt J, Bachus KN. Biomechanical analysis of bicondylar tibial plateau fixation: How does lateral locking plate fixation compare to dual plate fixation? J Orthop Trauma 2007;21:301-6. [Google Scholar] [PubMed]
- 15. Raj M, Gill S, Rajput A, Singh KS, Verma KS. Outcome analysis of dual plating in management of unstable bicondylar tibial plateau fracture – a prospective study. Malays Orthop J 2021;15:29-35. [Google Scholar] [PubMed]
- 16. Biggi F, Di Fabio S, D’Antimo C, Trevisani S. Tibial plateau fractures: Internal fixation with locking plates and the MIPO technique. Injury 2010;41:1178-82. [Google Scholar] [PubMed]
- 17. Elsoe R, Larsen P, Nielsen NP, Swenne J, Rasmussen S, Ostgaard SE. Population-based epidemiology of tibial plateau fractures. Orthopedics 2015;38:e780-6. [Google Scholar] [PubMed]
- 18. Krause M, Müller G, Frosch KH. Chirurgische Zugänge bei Tibiakopffrakturen [Surgical approaches to tibial plateau fractures]. Unfallchirurg 2018;121:569-82. [Google Scholar] [PubMed]
- 19. Papagelopoulos PJ, Partsinevelos AA, Themistocleous GS, Mavrogenis AF, Korres DS, Soucacos PN. Complications after tibia plateau fracture surgery. Injury 2006;37:475-84. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study
June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study October 1, 2025 Radiological and Functional Assessment of Tibial Plateau Fractures Managed with Locking Compression Plates: A Prospective Study
October 1, 2025 Radiological and Functional Assessment of Tibial Plateau Fractures Managed with Locking Compression Plates: A Prospective Study August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series
August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures
August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures