
Paraspinal compartment syndrome must be considered in the post-operative setting as a cause of acute back pain and can be successfully managed non-operatively.
Dr. Gbolabo Sokunbi, Department of Spine Surgery, Hospital for Special Surgery East River Professional Building, 523 East 72nd Street, 3rd Floor, New York, NY 10021, United States. E-mail: sokunbig@HSS.edu
Abstract
Introduction: Lumbar paraspinal compartment syndrome has been infrequently reported in the literature and often overlooked in the evaluation of acute low back pain. In the post-operative setting, few cases have been described, but none after total joint arthroplasty, and appropriate management remains controversial.
Case Report: A 55-year-old male developed severe low back pain and left lower extremity radiculopathy in the immediate postoperative period following revision total knee arthroplasty. Magnetic resonance imaging demonstrated diffuse oedema throughout the left lumbosacral paraspinal musculature, and he was found to have an elevated creatine kinase level. This was consistent with acute paraspinal compartment syndrome, which was successfully managed with conservative treatment for the associated rhabdomyolysis. By the 1-year follow-up, he demonstrated resolution of his symptoms and returned to baseline activity level.
Conclusion: Paraspinal compartment syndrome must be considered in the differential diagnosis of low back pain that onsets in the immediate post-operative period. Non-operative management can result in positive outcomes.
Keywords: Paraspinal compartment syndrome, acute low back pain, radiculopathy, arthroplasty, spost-operative complication.
Lumbar paraspinal compartment syndrome is a rare but notable consideration in the differential diagnosis for low back pain. Similar to compartment syndrome of the extremities, the diagnosis is clinical, with perhaps the most important feature being pain out of proportion to exam and increasing analgesia requirements. It occurs due to increased pressure within the paravertebral myofascial compartments. Prior case reports have described acute presentations secondary to an inciting event as well as chronic exertional paraspinal compartment syndrome. The most common aetiologies for acute development include atraumatic physical exertion, direct trauma to the paraspinal musculature, and post-operative secondary to non-spine surgery [1]. Here, we describe a case of acute lumbar paraspinal compartment syndrome following total joint arthroplasty. The patient was informed that data concerning the case would be submitted for publication, and he provided consent.
A 55-year-old male with a medical history of polysubstance use, diabetes, morbid obesity (body mass index [BMI] 55 kg/m2), and obstructive sleep apnoea presented as a direct admission to our hospital with surgical site drainage and a right prosthetic knee hinge dislocation (Fig. 1a). The patient underwent primary total knee arthroplasty in 2012, which required multiple revision surgeries for infectious and mechanical complications – most recently a polyethylene liner exchange for instability 6 months prior. Notable home medications included suboxone for chronic opioid use and Bactrim for prosthetic joint infection. On admission, the patient denied musculoskeletal pain outside the right knee and was neurovascularly intact with noted baseline neuropathy. The patient subsequently underwent right knee irrigation and debridement with revision of the femoral component and modular bearings (Fig. 1b).
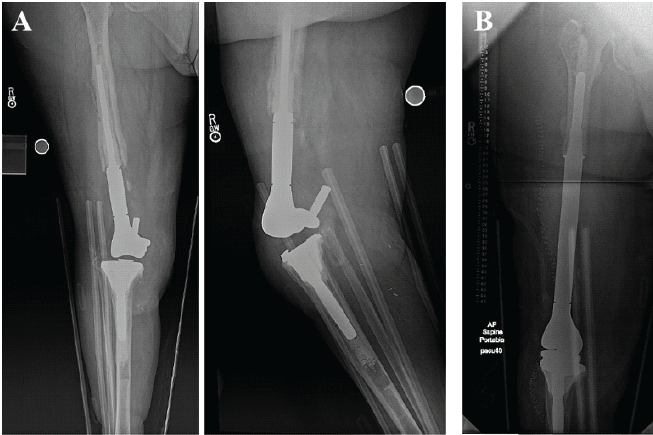
Figure 1: Radiographs depicting the patient’s right knee revision arthroplasty; (a) pre-operative with hinge dislocation on anteroposterior and lateral views; (b) post-operative.
The surgery was performed with the patient positioned supine on a standard operating room bed under combined spinal-epidural with 0.5% bupivacaine without complications. Total case duration was 3.5 h, with estimated blood loss of 1 L. Postoperatively, he was started on empiric antibiotics per the infectious disease team and maintained on a multimodal pain regimen, including epidural patient-controlled analgesia (PCA) per our chronic pain service.
On the early morning of post-operative day (POD) 1, approximately 7 h after leaving the operating room, the patient noted new-onset, severe low back pain, more on the left than the right. The epidural PCA was discontinued, and he was transitioned to a morphine intravenous PCA and started on Precedex. Four hours later, the patient reported increasing low back pain with sciatic pain radiating from the posterolateral hip to the lateral foot. The PCA was extended, and his gabapentin dose increased. Due to persistent symptoms, neurology was asked to evaluate the patient on the evening of POD1. The examination demonstrated full strength with no clear sensory level deficit, and the aetiology of his radiculopathy was undetermined. Of note, the patient had a history of bilateral sciatica earlier in the year, which resolved after 6 months with oral pain medications. However, he reported that the current symptoms were not similar.
On POD2, the patient reported persistent pain, and the spine surgery service was consulted, with the exam again demonstrating full strength and baseline numbness to the left lateral thigh and right lower extremity. Tenderness along the paraspinal musculature was also noted. Magnetic resonance imaging (MRI) of the lumbar spine from 6 months prior was reviewed, showing multilevel degenerative changes with moderate L3-5 central stenosis (Fig. 2).
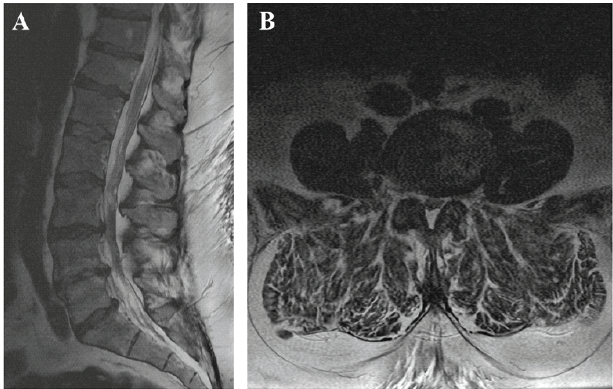
Figure 2: Lumbar T2-weighted magnetic resonance imaging obtained 6 months before current presentation, demonstrating moderate L3-5 central stenosis; (a) sagittal view; (b) axial view at L3-4.
Given a lack of new neurologic deficits on exam, a trial of Decadron was recommended before repeating advanced imaging. Unfortunately, the patient did not sustain any relief from the steroids over 72 h, and a repeat MRI was ordered on POD5. This demonstrated interval diffuse oedema throughout the left lumbosacral paraspinal musculature without a distinct fluid collection, otherwise unchanged (Fig. 3).
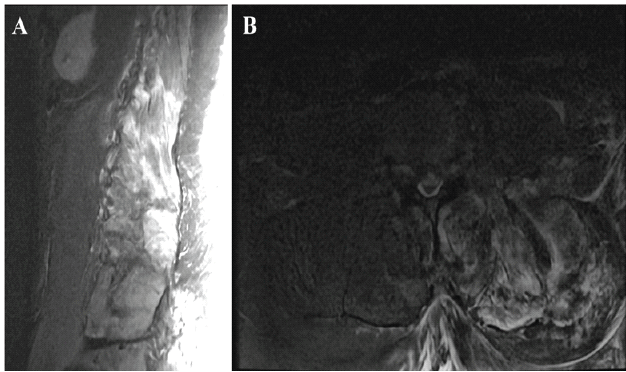
Figure 3: Lumbar inversion recovery sequence magnetic resonance imaging demonstrating left-sided paraspinal muscle edema at L1-L5; (a) sagittal view; (b) axial view at L3-4.
A creatine kinase (CK) level was obtained and elevated at 4,079. With concern for rhabdomyolysis, intravenous fluids were started. Over the next several days, the serum CK levels trended down, and as such, no further spine interventions were deemed warranted. The patient’s symptoms gradually improved with normalisation of CK over 3 weeks. The patient’s post-operative course was complicated by another dislocation of his right knee prosthesis, and he underwent second revision surgery, eventually being discharged on POD50 from the index procedure. His back pain and radiculopathy were fully resolved on discharge without residual deficits and remain as such at the 1-year follow-up.
Paraspinal compartment syndrome was first described in 1985 by Carr et al. [2]. Since then, attention to the diagnosis has increased, but fewer than 50 cases have been published. Diagnostic clinical criteria for acute paraspinal compartment syndrome are as follows: Excruciating pain with or without radiation that worsens with flexion and relieves with extension; board-like rigidity of the involved muscles; hypoactive bowel sounds with abdominal tenderness; and localised sensory loss with or without muscle atrophy. These typically present within 12 h of an insulting injury, as in our case, and 62.2% involve bilateral musculature [1]. Further supportive evidence includes elevated CK, myoglobinuria, higher intracompartmental pressure (~70–80 mmHg), and increased T2 signal intensity on MRI. To date, only 16.2% of reported cases occurred in the post-operative setting [3]. Four of the post-operative cases were reported following abdominal vascular surgery (i.e., aortic aneurysm repair) [4,5,6,7]. In this setting, diminished blood flow due to hypotension, location, and duration of aortic clamping are thought to contribute, as the lumbar compartments are supplied by dorsal branches of the segmental arteries, which branch off the abdominal aorta. Cases have also been described after gastric bypass surgery and radical cystectomy [5,8]. To the best of our knowledge, only two cases have been published following orthopaedic surgery. Sudhir et al. presented a 27-year-old female with an L1 fracture who underwent T12-L2 posterior fusion with percutaneous pedicle screws [9]. She developed acute back pain and wound drainage on POD3 with elevated CK levels, ultimately requiring an operative irrigation and debridement, which showed pale, avascular, and non-contractile paraspinal muscles with biopsy-confirmed necrosis. Saadat and Rezania further presented a 60-year-old male with 7 years of chronic low back pain and numbness; left lower extremity radiculopathy; and numbness to the left leg and lateral foot, which developed acutely after ankle surgery [10]. CK was elevated in the immediate post-operative period, and a new MRI demonstrated fatty infiltration of the paraspinal musculature. Therefore, the present case demonstrates the first example of lumbar paraspinal compartment syndrome following total joint arthroplasty. There are currently no standardised guidelines for the treatment of acute paraspinal compartment syndrome. Approximately half of reported cases have been managed operatively with fasciotomies through minimally invasive dual paramedian incisions with good functional outcomes [11,12,13,14,15]. Compared with non-operative management, surgery has been associated with a greater chance of resolution of pain and return to baseline activities without limitation [3,16]. Non-operative cases tend to have persistent discomfort, pain or sensory loss; however, symptoms often only present with physical exertion, and follow-up is typically limited to several months [2,5,10,17,18,19]. In one longer-term case report, a patient managed non-operatively was asymptomatic and had returned to collegiate-level athletics at 2-year follow-up [20]. It is also pertinent to consider that lumbar paraspinal compartment syndrome is currently a diagnosis of exclusion. As a result, there are likely patients with positive outcomes who are unintentionally managed conservatively when they seek care for low back pain. Thus, conclusions about treatment recommendations and surgical indications for this condition cannot be elucidated without comparative studies, and a trial of non-operative treatment may be reasonable. With regard to the present case, a patient developed lumbar paraspinal compartment syndrome in the immediate post-operative period after total joint arthroplasty. He demonstrated improvement of symptoms with appropriate control of his rhabdomyolysis, which previous authors have touted as the key for successful non-operative management in the long term [20]. It is also pertinent to consider that lumbar paraspinal compartment syndrome is currently a diagnosis of exclusion. As a result, there are likely patients with positive outcomes who are unintentionally managed conservatively when they seek care for low back pain. Thus, conclusions about treatment recommendations and surgical indications for this condition cannot be elucidated without comparative studies, and a trial of non-operative treatment may be reasonable.
Although paraspinal compartment syndrome has not been frequently reported, it must be considered in a patient with new-onset severe low back pain secondary to a provoking event. In the post-operative period, prolonged surgery and high BMI may be risk factors, and there should be higher suspicion in patients who received neuraxial or regional anaesthesia, which may mask symptoms. While the majority of patients will likely recover with non-surgical treatment, fasciotomies may be considered when an early diagnosis is made, the patient has worsening pain and neurologic symptoms, or CK levels remain elevated – thereby posing risk to other organs – despite appropriate supportive care.
Paraspinal compartment syndrome can present as acute low back pain in the postoperative setting after orthopaedic surgery, with long operative time and high BMI as risk factors. Non-operative management can be successful, but worsening symptoms may warrant surgical fasciotomies.
References
- 1. Nathan ST, Roberts CS, Deliberato D. Lumbar paraspinal compartment syndrome. Int Orthop 2012;36:1221-7. [Google Scholar] [PubMed]
- 2. Carr D, Gilbertson L, Frymoyer J, Krag M, Pope M. Lumbar paraspinal compartment syndrome. A case report with physiologic and anatomic studies. Spine (Phila Pa 1976) 1985;10:816-20. [Google Scholar] [PubMed]
- 3. Ilyas H, Fagan C, Roser F, Hebela NM. Lumbar paraspinal compartment syndrome: Case report and critical evaluation of the literature. Clin Spine Surg 2022;35:301-9. [Google Scholar] [PubMed]
- 4. Osamura N, Takahashi K, Endo M, Kurumaya H, Shima I. Lumbar paraspinal myonecrosis after abdominal vascular surgery: A case report. Spine (Phila Pa 1976) 2000;25:1852-4. [Google Scholar] [PubMed]
- 5. Haig AJ, Hartigan AG, Quint D. Low back pain after nonspinal surgery: The characteristics of presumed lumbar paraspinal compartment syndrome. PM R 2009;1:383-8. [Google Scholar] [PubMed]
- 6. Ferreira J, Galle C, Aminian A, Michel P, Guyot S, De Wilde JP, et al. Lumbar paraspinal rhabdomyolysis and compartment syndrome after abdominal aortic aneurysm repair. J Vasc Surg 2003;37:198-201. [Google Scholar] [PubMed]
- 7. Fitch DS, Leung D, Reish AG. Extensive lumbar paraspinal fluid/fat collections from lumbar paraspinal myonecrosis and presumed subsequent compartment syndrome: 7 years post onset. Spine J 2014;14:1077-8. [Google Scholar] [PubMed]
- 8. Sauliunaite V, Vecsernyés N, Coronado M. Acute lumbar paraspinal compartment syndrome after radical cystectomy. BMJ Case Rep 2024;17:e255983. [Google Scholar] [PubMed]
- 9. Sudhir G, Adsul NM, Acharya S, Chahal RS. Compartment syndrome of lumbar paraspinal musculature after percutaneous pedicle screw fixation. Surg Neurol Int 2018;9:190. [Google Scholar] [PubMed]
- 10. Saadat N, Rezania K. Postoperative lumbar paraspinal compartment syndrome. BMJ Case Rep 2021;14:e236040. [Google Scholar] [PubMed]
- 11. Vanbrabant P, Moke L, Meersseman W, Vanderschueren G, Knockaert D. Excruciating low back pain after strenuous exertion: Beware of lumbar paraspinal compartment syndrome. J Emerg Med 2015;49:641-3. [Google Scholar] [PubMed]
- 12. Maeckelbergh L, Moke L. An acute paraspinal compartment syndrome: Anatomic description of the compartment and surgical technique. Clin Spine Surg 2019;32:E277-81. [Google Scholar] [PubMed]
- 13. Mattiassich G, Larcher L, Leitinger M, Trinka E, Wechselberger G, Schubert H. Paravertebral compartment syndrome after training causing severe back pain in an amateur rugby player: Report of a rare case and review of the literature. BMC Musculoskelet Disord 2013;14:259. [Google Scholar] [PubMed]
- 14. Roe JC, Chen F, Cho W. Acute paravertebral compartment syndrome: Follow-up and literature review. J Am Acad Orthop Surg Glob Res Rev 2018;2:e063. [Google Scholar] [PubMed]
- 15. Khan RJ, Fick DP, Guier CA, Menolascino MJ, Neal MC. Acute paraspinal compartment syndrome. A case report. J Bone Joint Surg Am 2005;87:1126-8. [Google Scholar] [PubMed]
- 16. Alexander W, Low N, Pratt G. Acute lumbar paraspinal compartment syndrome: A systematic review. ANZ J Surg 2018;88:854-9. [Google Scholar] [PubMed]
- 17. Karam MD, Amendola A, Mendoza-Lattes S. Case report: Successful treatment of acute exertional paraspinal compartment syndrome with hyperbaric oxygen therapy. Iowa Orthop J 2010;30:188-90. [Google Scholar] [PubMed]
- 18. Wik L, Patterson JM, Oswald AE. Exertional paraspinal muscle rhabdomyolysis and compartment syndrome: A cause of back pain not to be missed. Clin Rheumatol 2010;29:803-5. [Google Scholar] [PubMed]
- 19. Ogoshi T, Yoshimiya M, Ichibakase H, Kimura T, Kameoka M, Yoshioka H, et al. Paravertebral compartment syndrome after exercise: A case report. J Med Case Rep 2020;14:208. [Google Scholar] [PubMed]
- 20. Kanaya H, Enokida M, Tanishima S, Hayashi I, Tanida A, Nagashima H. Conservative treatment for lumbar compartment syndrome shows efficacy over 2-year follow-up: A case report and literature review. Arch Orthop Trauma Surg 2017;137:1233-8. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience
August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty June 1, 2026 Determining the Accuracy of Acetabular Cup Size using Acetate Templates on Digital Radiographs in Patients Undergoing Total Hip Replacement
June 1, 2026 Determining the Accuracy of Acetabular Cup Size using Acetate Templates on Digital Radiographs in Patients Undergoing Total Hip Replacement June 1, 2026 Achieving Safe Zone Cup Positioning in Total Hip Arthroplasty using Anatomical Landmarks: A Prospective Computed Tomography-based Evaluation
June 1, 2026 Achieving Safe Zone Cup Positioning in Total Hip Arthroplasty using Anatomical Landmarks: A Prospective Computed Tomography-based Evaluation