
Acetate templating on magnified digital radiographs is a reliable and cost-effective method for accurately predicting acetabular cup size in total hip replacement, especially in resource-limited settings.
Dr. Mohammed Shahid, Department of Orthopaedics, Vydehi Institute of Medical Sciences and Research Centre, Whitefield, Bengaluru - 560 066, Karnataka, India. E-mail: bonedrshahid@gmail.com
Abstract
Introduction: Accurate pre-operative templating is essential for successful total hip replacement (THR) to optimize component sizing and minimize complications. With the transition to digital radiography, traditional acetate templating faces compatibility challenges. This study evaluates the accuracy of acetate templates on magnified digital radiographs as a cost-effective alternative to digital templating software.
Materials and Methods: A prospective observational study was conducted over 18 months on 25 patients undergoing uncemented total hip arthroplasty (THA) at a tertiary care center. Standardized anteroposterior pelvic radiographs with a 3 cm metal marker were obtained. Digital images were magnified to match the acetate template scale. Pre-operative predictions were compared with actual intraoperative acetabular cup sizes.
Results: The mean patient age was 66.60 ± 5.74 years with male predominance (68%). Osteoarthritis was the most common indication (48%). Pre-operative templating predicted acetabular cup size with 88% exact match and 100% accuracy within ±2 mm. Most radiographs were rated good quality (64%). The most common cup sizes used were 50 mm and 54 mm.
Conclusion: Acetate templating on digital radiographs provides highly accurate, reliable, and cost-effective prediction of acetabular cup size in THA. This method demonstrates excellent predictive power with 88% exact match and 100% accuracy within ±2 mm, making it a valuable tool, especially in resource-limited settings where advanced templating software may be unavailable.
Keywords: Total hip replacement, acetabular cup, acetate templates, digital radiography, pre-operative templating, arthroplasty.
Total hip arthroplasty (THA) represents one of the most successful and commonly performed orthopaedic procedures worldwide, providing substantial pain relief and functional improvement for patients with debilitating hip pathology [1]. The success of THA depends critically on multiple factors, including proper patient selection, surgical technique, implant positioning, and accurate component sizing [2]. Among these factors, pre-operative planning and templating have emerged as essential components that significantly influence surgical outcomes, operative efficiency, and long-term implant survival [3]. Pre-operative templating serves multiple crucial purposes in total hip replacement (THR) surgery. First and foremost, it enables surgeons to predict the appropriate size of both the acetabular cup and femoral stem components before entering the operating room, thereby ensuring that necessary implants and instruments are available during surgery [4]. This advance preparation minimises operative time, reduces the need for intraoperative trial-and-error sizing, and decreases the likelihood of requiring unusual or unavailable component sizes. In addition, accurate templating facilitates restoration of proper hip biomechanics, including hip offset and leg length, which are critical determinants of post-operative function, patient satisfaction, and implant longevity [5]. Historically, pre-operative templating was performed using transparent acetate overlay templates provided by implant manufacturers, which were positioned over conventional analogue radiographic films [6]. These acetate templates were manufactured with a predetermined magnification factor, typically 115–120%, to match the inherent magnification present in standard radiographic imaging. Surgeons would physically overlay these templates on radiographic films to determine optimal implant sizes and positions. This method, while relatively simple and cost-effective, proved reasonably accurate and became the standard approach for several decades [7]. However, the landscape of medical imaging has undergone a dramatic transformation with the widespread adoption of digital radiography and picture archiving and communication systems (PACS). Digital radiography offers numerous advantages over traditional film-based imaging, including superior image quality, immediate availability, ease of storage and retrieval, reduced radiation exposure, and elimination of film processing costs [8]. Consequently, most modern orthopaedic practices and hospitals have transitioned completely to digital imaging systems, rendering traditional analogue radiographic films increasingly obsolete or entirely unavailable. This technological evolution has created a significant practical challenge for pre-operative templating in THR. Digital radiographs lack the standardised magnification inherent to analogue films, and their displayed size can be easily manipulated through computer software. Consequently, traditional acetate templates designed for analogue films cannot be directly applied to digital images displayed on computer monitors [9]. This incompatibility has necessitated the development of alternative templating approaches for the digital era. Several solutions have emerged to address this challenge. Digital templating software packages have been developed that contain digital libraries of implant templates from various manufacturers. These software programs allow surgeons to import digital radiographic images, calibrate magnification using reference markers, and overlay digital templates to plan the procedure [10]. While these digital templating systems have demonstrated good accuracy and reliability, they present several limitations. First, they require significant financial investment for software licensing and regular updates. Second, they necessitate specialised training for proper use. Third, they may not include templates for all implant systems used by a particular surgeon or institution. Finally, they require integration with existing PACS infrastructure, which can pose technical challenges [11]. Given these limitations of commercial digital templating software, there remains substantial interest in developing simpler, more accessible, and cost-effective templating methods that can utilise traditional acetate templates with digital radiography. Several researchers have explored various techniques to achieve this goal, including the use of calibration markers of known size placed near the patient during radiography; direct magnification of digital images to match the acetate template scale; and mathematical calculation of appropriate implant sizes based on anatomical measurements [12,13]. The acetabulum represents a critical focus of pre-operative planning in THR. Accurate prediction of acetabular cup size is essential for several reasons. During surgery, the acetabulum is progressively reamed in 2 mm increments until an optimal fit is achieved, with reaming continued until subchondral bone is exposed. An uncemented cup of the same diameter or 1–2 mm larger is then press-fitted into the prepared acetabulum [14]. If the surgeon’s pre-operative size estimate is inaccurate, valuable operative time may be wasted on excessive trial sizing, or worse, inappropriate cup sizing may lead to inadequate fixation, malposition, or other complications. Furthermore, having accurate pre-operative size predictions ensures that the necessary implant sizes are available in the operating room, avoiding delays or the need to use suboptimal alternative components. Research on pre-operative templating accuracy has yielded variable results depending on the methods employed. Studies using traditional acetate templates on analogue radiographs reported accuracy rates ranging from 70% to 90% for predicting acetabular cup size within one size increment [15]. With the advent of digital templating software, some studies have reported similar or slightly improved accuracy, though results have been inconsistent. Factors affecting templating accuracy include radiographic quality, patient positioning during imaging, proper calibration of magnification, surgeon experience, and the specific templating method employed. Despite the availability of sophisticated digital templating software, many orthopaedic practices, particularly in resource-limited settings, continue to seek simpler and more cost-effective alternatives. The ability to accurately template using traditional acetate overlays on digital radiographs would offer significant advantages, including minimal cost, no requirement for specialised software or training, compatibility with existing acetate template libraries, and straightforward implementation in any practice with access to digital radiography. This study was undertaken to evaluate the accuracy and reliability of a standardised method for using traditional acetate templates on magnified digital radiographs to predict acetabular cup size in patients undergoing uncemented THR. By utilising a metal calibration marker of known size and magnifying digital radiographs to match the acetate template scale, we sought to determine whether this simple, cost-effective approach could provide accuracy comparable to more expensive digital templating systems. Understanding the precision of this technique has important implications for surgical planning, resource allocation, and clinical practice, particularly in settings where advanced digital templating software may not be readily available or economically feasible.
Aims and objectives:
Primary aim:
This study aims to determine whether acetate templating on magnified digital radiographs accurately predicts the acetabular cup size required during THR surgery.
Specific objectives:
- To evaluate the exact match accuracy rate between preoperatively predicted acetabular cup size using acetate templates and the actual intraoperative cup size utilized
- To assess the accuracy of predictions within a clinically acceptable range (±2 mm or one size increment)
- To determine the reliability and reproducibility of the acetate templating technique on digital radiographs
- To identify factors that may influence templating accuracy, including patient demographics, radiograph quality, and pre-operative diagnosis
- To analyse the cost-effectiveness of this technique compared to commercial digital templating software.
Study design and setting:
This prospective observational study was conducted at the Department of Orthopaedics, Vydehi Institute of Medical Sciences and Research Centre, Whitefield, Bengaluru, over 18 months from March 2023 to June 2024. The study protocol received approval from the Institutional Ethics Committee (VIEC/2023/APP/PG/033, EC Reg No: ECR/747/Inst/KA/2015/RR21, dated March 31, 2023). All patients provided written informed consent before enrolment after being fully informed about the study objectives, procedures, and their rights to withdraw at any time without affecting their clinical care.
Sample size calculation:
Sample size was calculated using the formula for diagnostic accuracy studies with the following parameters: alpha (α) = 0.05, estimated proportion (P) = 0.83 based on similar published studies, and estimated error (d) = 0.15. Based on this calculation and considering the institutional surgical volume, a sample size of 25 patients was deemed adequate for this pilot study. The sampling method employed was consecutive sampling, wherein all eligible patients presenting during the study period were enrolled until the target sample size was achieved.
Study population:
Inclusion criteria:
Patients meeting all of the following criteria were included in this study:
- Age 18 years or older
- Scheduled to undergo primary unilateral THR with an uncemented acetabular component
- Ability to provide informed consent
- An adequate-quality pre-operative anteroposterior (AP) pelvic radiograph available
- No contraindications to standard positioning for pelvic radiography.
Exclusion criteria:
Patients meeting any of the following criteria were excluded from the study:
- Presence of active local or systemic infection
- Previous hip surgery on the affected side (revision cases)
- Severe acetabular bone loss or developmental dysplasia requiring specialized implants
- Significant skeletal deformities preventing standardized radiographic positioning
- Neurological disorders affecting the hip region
- Inability to cooperate for proper radiographic positioning
- Pregnancy.
Pre-operative assessment and radiographic protocol:
All enrolled patients underwent a comprehensive pre-operative evaluation, including a detailed history, physical examination, and routine laboratory investigations required for surgical fitness assessment. Standard AP radiographs of the pelvis, including both hips, were obtained using a standardised technique. Patients were positioned supine on the radiographic table with both lower limbs in 15–20° of internal rotation. The X-ray beam was centred on the midpoint between the symphysis pubis and the line connecting both anterior superior iliac spines. The source-to-film distance was maintained at 1 m for all patients to ensure consistency. A critical component of our methodology involved the use of a calibration marker. A spherical metal ball measuring exactly 30 mm in diameter was secured to the patient’s skin at the level of the greater trochanter on the affected side using adhesive tape. This marker served as a reference object of known size to facilitate subsequent magnification calibration of the digital images.
Radiographic equipment:
All radiographs were acquired using a Philips Digital Diagnostic radiography system. Images were captured in digital format, stored in the hospital’s PACS, and exported as high-resolution JPEG files for templating purposes. Images were reviewed for adequate quality, proper patient positioning, and clear visualisation of relevant anatomical landmarks, including both femoral heads, the entire pelvis, bilateral acetabula, and proximal femurs extending to a level below the lesser trochanters.
Templating procedure:
The templating procedure followed a standardised protocol developed specifically for this study, based on established principles but adapted for use with digital radiography.
Step 1: Image preparation:
Digital radiographic images were transferred from PACS to a dedicated computer workstation with a high-resolution LCD monitor. Images were opened using standard image viewing software that allowed for magnification adjustment while maintaining aspect ratio.
Step 2: Magnification calibration:
The calibration process utilised the 30 mm metal ball marker visible in the radiograph. Using the image viewing software’s measurement tool, a digital line was drawn to measure the diameter of the metal ball as it appeared in the radiograph. The image was then magnified or reduced until the measured diameter of the metal ball matched its actual physical size of 30 mm when measured against a standard ruler placed directly on the computer monitor screen. This process effectively calibrated the displayed image to a 1:1 scale or 100% magnification, eliminating the magnification inherent in the radiographic process.
Step 3: Acetate template application:
Manufacturer-provided acetate templates (Stryker Corporation) were utilised for templating. These templates are designed with a built-in magnification factor of 1.20 (120%) to match typical radiographic magnification. Since our digital images had been calibrated to a 1:1 scale, the templates were applied directly to the computer monitor screen over the displayed image. The acetabular templating followed established anatomical principles. Three key radiographic landmarks were identified: (1) The base of the radiographic teardrop, (2) The ilioischial line (Kohler’s line) and (3) The superolateral margin of the acetabulum. The acetabular template was positioned such that its inferior edge aligned with the inter-teardrop line, its medial border matched the ilioischial line, and its superolateral margin approximated the anatomical acetabular rim. The template was orientated at an abduction angle of 40–45° to simulate ideal cup positioning. Multiple template sizes were evaluated, and the size providing the best fit according to these anatomical criteria was recorded as the predicted acetabular cup size. The templating was performed by the primary investigator, who was blinded to intraoperative findings at the time of templating. For a subset of cases, independent templating was also performed by a second observer to assess interobserver reliability.
Surgical procedure:
All surgical procedures were performed by a single experienced arthroplasty surgeon using a standardised posterior approach to the hip. The surgeon was blinded to the pre-operative templating results to eliminate bias in intra-operative decision-making. After exposure of the hip joint and femoral head resection, the acetabulum was prepared using sequential hemispherical reamers, beginning with a small size and progressively increasing in 2 mm increments until adequate coverage of the subchondral bone was achieved and a stable rim was established.
Trial acetabular components were inserted to assess fit and stability. The final acetabular cup size selected was based on achieving optimal press-fit fixation, adequate bone coverage, and appropriate positioning. All surgeries utilised uncemented porous-coated hemispherical acetabular cups (Stryker Trident System) with polyethylene liners. The actual size of the acetabular cup implanted was recorded as the definitive intraoperative measurement against which pre-operative predictions were compared.
Data collection and variables:
A standardised data collection form was utilised to record all relevant variables for each patient. Demographic data included age, gender, body mass index (BMI), and contact information. Clinical data encompassed the primary pre-operative diagnosis (osteoarthritis, avascular necrosis, rheumatoid arthritis, fracture, or other); relevant comorbidities, including diabetes mellitus and hypertension; and surgical parameters, including duration of surgery, intraoperative blood loss, and any complications encountered. The primary outcome variable was the accuracy of acetabular cup size prediction, defined in two ways: (1) Exact match accuracy – the percentage of cases where the predicted size exactly matched the implanted size; and (2) Acceptable accuracy – the percentage of cases where the predicted size was within one size increment (±2 mm) of the implanted size. Secondary variables included radiographic quality (rated as good, fair, or poor based on image clarity and proper positioning), predictive accuracy categories (accurate prediction, overestimated size, or underestimated size), and potential confounding factors.
Statistical analysis:
All data were entered into Microsoft Excel spreadsheets and subsequently analysed using the IBM Statistical Package for the Social Sciences Statistics version 25.0. Descriptive statistics were calculated for all variables. Continuous variables were expressed as mean ± standard deviation and tested for normality using the Shapiro-Wilk test. Categorical variables were presented as frequencies and percentages. The accuracy rates were calculated along with 95% confidence intervals. Chi-square tests or Fisher’s exact test was used to examine associations between categorical variables. Correlation analyses were performed using Pearson’s or Spearman’s rank correlation tests as appropriate based on data distribution. P < 0.05 was considered statistically significant.
Patient demographics:
A total of 25 patients meeting the inclusion and exclusion criteria were enrolled in this prospective study. The age distribution revealed that the majority of participants (56%, n = 14) were in the 61–70 years age group, followed by 28% (n = 7) in the 71–80 years category and 16% (n = 4) in the 51–60 years group. The mean age of the study population was 66.60 ± 5.74 years (range: 52–75 years). Gender analysis showed a male predominance, with 17 males (68%) and 8 females (32%). The mean BMI was 29.14 ± 3.49 kg/m2, indicating that, on average, the study participants were classified as overweight according to World Health Organization criteria (Table 1).
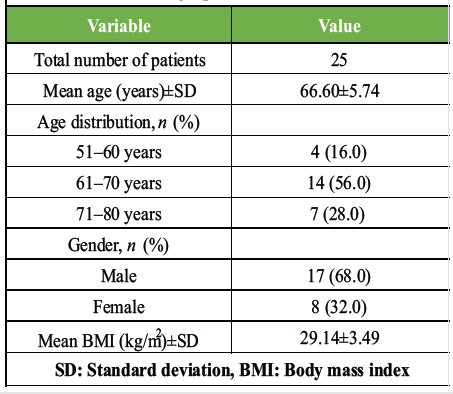
Table1: Patient demographics and clinical characteristics
Preoperative diagnosis:
Analysis of the primary pathology necessitating THR revealed that osteoarthritis was the most common indication, affecting 12 patients (48%). Avascular necrosis and rheumatoid arthritis each accounted for 6 patients (24% each), whereas fracture was the indication in only 1 patient (4%). This distribution is consistent with epidemiological data showing osteoarthritis as the leading cause requiring THA in the general population (Table 2).
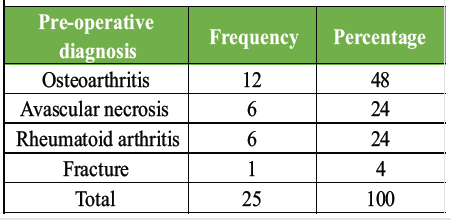
Table 2: Distribution of pre-operative diagnoses
Acetabular cup size distribution:
The pre-operative templating predicted acetabular cup sizes ranging from 48 mm to 56 mm. The most frequently predicted sizes were 50 mm and 54 mm, each predicted in 6 cases (24%); followed by 52 mm in 5 cases (20%); and 48 mm and 56 mm, each predicted in 4 cases (16%). The actual intraoperative acetabular cup sizes utilised ranged from 48 mm to 58 mm. The most commonly used size was 50 mm in 7 cases (28%), followed by 52 mm and 54 mm, each used in 5 cases (20%); 56 mm in 4 cases (16%); 48 mm in 3 cases (12%); and 58 mm in 1 case (4%) (Table 3).
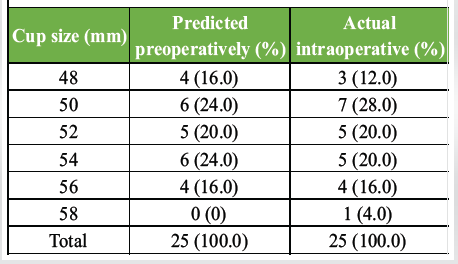
Table 3: Distribution of predicted and actual acetabular cup sizes
Radiographic quality assessment:
Evaluation of radiographic image quality showed that the majority of radiographs (64%, n = 16) were rated as good quality, meaning they demonstrated excellent visualisation of anatomical landmarks, proper patient positioning, and adequate image resolution. Seven radiographs (28%) were rated as fair quality, with minor limitations but still adequate for templating purposes. Only 2 radiographs (8%) were classified as poor quality, typically due to suboptimal positioning or image clarity issues (Table 4).
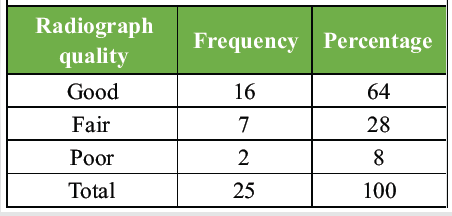
Table 4: Radiographic quality distribution
Predictive accuracy analysis:
The primary outcome measure of this study was the accuracy of preoperative templating in predicting the actual acetabular cup size used during surgery. Results demonstrated that in 22 cases (88%), the preoperatively predicted cup size exactly matched the actual cup size implanted during surgery. In 2 cases (8%), the templating overestimated the required size, meaning the predicted size was larger than what was actually used. In 1 case (4%), the templating underestimated the size, with the actual cup being larger than predicted. When evaluating accuracy within a clinically acceptable range of ±2 mm (one size increment), the accuracy rate reached 100%, with all 25 cases (100%) falling within this acceptable margin (Table 5).
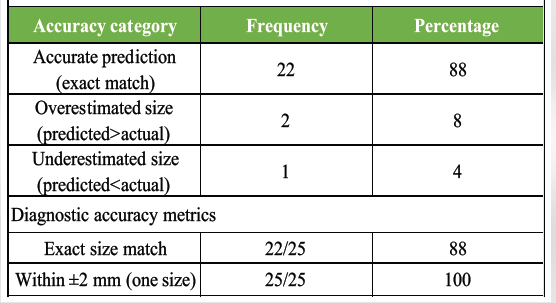
Table 5: Predictive accuracy of acetate templating
Relationship between variables:
Analysis of the relationship between radiographic quality and predictive accuracy revealed that all cases with good quality radiographs (16/16, 100%) achieved accurate predictions within one size increment. Among fair-quality radiographs, 7/7 (100%) were also accurate within one size. Interestingly, even the two cases with poor quality radiographs achieved accuracy within one size, though one of these represented an exact size mismatch. This suggests that while image quality influences optimal templating, the method demonstrates robustness even with suboptimal radiographs, though exact match accuracy may be compromised. Evaluation of predictive accuracy across different diagnostic categories showed that osteoarthritis cases had an 83.3% (10/12) exact match rate, avascular necrosis cases showed a 100% (6/6) exact match, rheumatoid arthritis cases demonstrated an 83.3% (5/6) exact match, and the single fracture case showed an exact match. These differences were not statistically significant (P > 0.05), suggesting that the underlying pathology does not substantially impact templating accuracy with this method. BMI showed no significant correlation with templating accuracy (r = 0.12, P = 0.56), indicating that patient body habitus did not substantially affect the precision of acetate templating in this study population. Similarly, age and gender showed no significant association with predictive accuracy (P = 0.43 and P = 0.67, respectively), suggesting that the method is equally reliable across different demographic groups.
Summary of key findings:
In summary, this prospective study of 25 patients undergoing uncemented THA demonstrated that acetate templating on magnified digital radiographs is highly accurate for predicting acetabular cup size. The technique achieved an 88% exact match rate and 100% accuracy within a clinically acceptable range of ±2 mm. The method proved reliable across different patient demographics, preoperative diagnoses, and varying radiographic quality levels, supporting its potential utility as a cost-effective alternative to expensive digital templating software.
This prospective study evaluated the accuracy of using traditional acetate templates on magnified digital radiographs for predicting acetabular cup size in THR surgery. Our findings demonstrate that this simple, cost-effective method achieves excellent predictive accuracy, with 88% exact size match and 100% accuracy within a clinically acceptable range of ±2 mm. These results have important implications for surgical planning, particularly in resource-limited settings where expensive digital templating software may not be available or economically justified. The 88% exact match accuracy observed in our study compares favorably with published literature on various templating methods. Goyal et al. reported an exact size accuracy of 36.7% for acetabular cups and 89.9% within ±1 size using a similar technique of acetate templating on LCD monitors after calibration with a digital radiography equipment scale. Krishnamoorthy et al. achieved 70% exact accuracy and 90% within one size using acetate templates with a metal ball calibration marker on digital radiographs, which is somewhat lower than our findings. The superior accuracy in our study may be attributed to meticulous attention to standardized radiographic technique, consistent use of the 30 mm calibration marker, and careful magnification calibration. Several studies have compared acetate templating with digital templating software. Petretta et al. found that acetate templating on digitally calibrated images was more accurate than computer-based templating for THA, with better interobserver and intraobserver reliability. Similarly, Pullen and Whiddon reported 96% accuracy for acetabular components with acetate methods versus 93% with digital methods, suggesting no significant advantage for digital software. These findings support our conclusion that traditional acetate templates remain a viable and accurate option when properly adapted for use with digital radiography. Our study population demographics were representative of typical THR patients, with a mean age of 66.60 ± 5.74 years and male predominance (68%). This age distribution aligns with epidemiological data showing that the majority of THRs are performed in patients between 60 and 75 years of age. The male preponderance in our series is consistent with some studies, though overall epidemiological data suggest relatively equal gender distribution in osteoarthritis-related hip replacements. The higher proportion of males in our study may reflect referral patterns or population-specific factors. Osteoarthritis was the predominant indication for surgery in 48% of patients, followed by avascular necrosis (24%) and rheumatoid arthritis (24%). This distribution is consistent with global epidemiological data identifying osteoarthritis as the leading cause requiring THA. Avascular necrosis represented a substantial proportion in our series, which may reflect regional patterns or specific patient demographics. Importantly, our analysis found no significant differences in templating accuracy across different diagnostic categories (P > 0.05), suggesting that the method is equally reliable regardless of the underlying pathology. The mean BMI of 29.14 ± 3.49 kg/m2 in our study population indicates that most patients were overweight or at the threshold of obesity. While obesity is recognized as a risk factor for complications in THR, we found no significant correlation between BMI and templating accuracy (r = 0.12, P = 0.56). This finding is reassuring and suggests that the calibration method using an external marker effectively compensates for potential magnification variations related to patient body habitus. Previous studies have reported conflicting results regarding BMI’s impact on templating accuracy, with some showing decreased accuracy in obese patients when using software-based methods. Radiographic quality assessment revealed that 64% of images were rated as good quality, 28% fair, and only 8% poor. Notably, the method achieved 100% accuracy within one size, even for the two cases with poor quality radiographs, though exact match accuracy was compromised in one of these cases. This finding underscores the robustness of the technique but also highlights the importance of obtaining high-quality radiographs for optimal results. Wasim et al. emphasized the importance of standardized radiographic protocols for pre-operative templating, demonstrating that implementation of standard protocols significantly improved radiograph adequacy from 58% to 89%. The distribution of acetabular cup sizes used in our study ranged from 48 mm to 58 mm, with 50 mm and 54 mm being the most common. This distribution is consistent with anatomical studies of acetabular dimensions in adult populations. The presence of one 58 mm cup, which was not predicted preoperatively, represents one of the cases where templating underestimated the required size. Intraoperative factors such as greater bone loss than anticipated on radiographs or technical considerations during reaming may account for such discrepancies. Several factors may influence templating accuracy regardless of the method employed. Patient positioning during radiography is critical, as improper positioning can distort anatomical relationships and affect magnification. We attempted to minimize this source of error using a standardized radiographic protocol with the patient supine and lower limbs in 15–20° internal rotation. The use of the 30 mm calibration marker placed at the level of the greater trochanter provided a reliable reference for magnification calibration, though its effectiveness depends on proper placement at approximately the same depth as the hip center. Lecerf et al. highlighted the importance of three-dimensional considerations in pre-operative planning, noting that two-dimensional radiographs may underestimate measurements such as femoral offset. While our study focused specifically on acetabular cup sizing in the coronal plane, these observations underscore the inherent limitations of any two-dimensional templating method. Future studies incorporating computed tomography-based three-dimensional planning could provide interesting comparative data, though cost considerations may limit widespread implementation of such approaches. The cost-effectiveness of acetate templating compared to digital software is substantial. Commercial digital templating software packages typically require initial licensing fees of several thousand dollars, plus ongoing annual maintenance and update fees. In contrast, acetate templates are provided by implant manufacturers at minimal or no cost, and the only requirement is access to a computer with basic image viewing software and a calibration protocol. For practices performing moderate volumes of THRs, particularly in resource-limited settings, this cost difference is highly significant. However, digital templating software does offer certain advantages over acetate methods. Software programs typically include templates for multiple implant systems, facilitate documentation and storage of templating results, allow for quantitative assessment of parameters such as leg length and offset, and may incorporate automated measurements and calculations. For high-volume centers or practices using multiple implant systems, these features may justify the additional cost. Nevertheless, our study demonstrates that for surgeons seeking a simple, accurate, and cost-effective method for basic cup size prediction, acetate templating on digital radiographs represents a viable alternative. Interobserver and intraobserver reliability are important considerations for any templating method. While our study was primarily performed by a single investigator, previous studies using similar acetate templating methods have reported excellent reliability. Krishnamoorthy et al. demonstrated strong interobserver and intraobserver reliability with intraclass correlation coefficients above 0.8. Shin et al. reported significant inter- and intraobserver reliability for both implant size (kappa > 0.70) and measurements such as leg length discrepancy (intraclass correlation coefficients 0.89–0.97) using on-screen templating of digital radiographs. Several limitations of our study warrant consideration. First, the sample size of 25 patients was relatively small, though adequately powered for the primary outcome based on our sample size calculation. Larger multicenter studies would provide more robust evidence and allow for subgroup analyses. Second, all surgeries were performed by a single experienced surgeon, which may limit generalizability to surgeons with different experience levels or surgical techniques. Third, we focused exclusively on acetabular cup sizing and did not evaluate femoral stem sizing or other parameters such as offset and leg length restoration. Fourth, the study was conducted at a single tertiary care center, which may not represent all practice settings. Additional limitations include the lack of long-term follow-up data to assess whether accurate templating translates into improved clinical outcomes. While logical to assume that accurate sizing contributes to optimal implant positioning and long-term survival, this relationship would require extended follow-up to confirm. Furthermore, we did not directly compare acetate templating with digital software in the same patient population, which would provide the strongest evidence regarding relative accuracy. Finally, challenging cases such as severe dysplasia, significant protrusion, or revision surgery were excluded, so our results may not apply to these complex scenarios. Despite these limitations, our study provides valuable evidence supporting the continued use of acetate templates in the era of digital radiography. The excellent accuracy achieved with proper calibration methodology demonstrates that sophisticated software is not necessary for accurate pre-operative planning in routine THR. This finding is particularly relevant for orthopedic surgeons in developing countries or resource-limited settings where access to expensive templating software may be restricted. Future research directions could include: (1) Larger multicenter studies to validate these findings across diverse populations and practice settings, (2) direct head-to-head comparison of acetate templating versus digital software in the same patients, (3) evaluation of acetate templating for femoral stem sizing and other parameters beyond cup size, (4) assessment of the technique in challenging cases such as dysplasia or revision surgery, (5) investigation of whether accurate templating correlates with improved long-term clinical outcomes and implant survival, (6) development of standardized protocols and training programs to optimize implementation of acetate templating in digital workflows. In conclusion, this study demonstrates that acetate templating on magnified digital radiographs is a highly accurate method for predicting acetabular cup size in THR, achieving 88% exact match and 100% accuracy within ±2 mm. The technique is simple, cost-effective, and reliable across different patient demographics and clinical scenarios. These findings support the continued use of traditional acetate templates when properly adapted for digital imaging, providing an accessible alternative to expensive digital templating software without compromising accuracy.
This prospective study of 25 patients undergoing uncemented THA demonstrates that acetate templating on magnified digital radiographs is a highly accurate, reliable, and cost-effective method for pre-operative prediction of acetabular cup size. The technique achieved an 88% exact match rate between predicted and actual implant sizes, with 100% accuracy within a clinically acceptable margin of ±2 mm (one size increment). These results compare favorably with published data on both traditional acetate methods and modern digital templating software. The standardized methodology utilizing a 30 mm calibration marker and systematic image magnification to match the acetate template scale proved robust across diverse patient demographics, varying radiographic quality, and different underlying pathologies. No significant differences in accuracy were observed based on age, gender, BMI, or pre-operative diagnosis, supporting the broad applicability of this technique in routine clinical practice. The findings have important practical implications, particularly for orthopedic practices in resource-limited settings where expensive digital templating software may not be available or economically justified. The minimal cost of acetate templates, combined with their ease of use and proven accuracy, makes this approach an attractive alternative to software-based methods. Even in well-resourced settings, this technique provides a valuable backup option when digital systems are unavailable or for surgeons who prefer traditional templating approaches. While digital templating software offers certain advantages, such as comprehensive implant libraries and automated measurements, our study confirms that these sophisticated tools are not essential for accurate basic pre-operative planning in straightforward primary THR. The acetate templating method described here preserves the simplicity and familiarity of traditional templating while successfully adapting to the realities of modern digital radiography. Future research with larger sample sizes, multicenter validation, and long-term outcome assessment would further strengthen the evidence base for this technique. Nevertheless, the current findings provide compelling support for acetate templating as a reliable, accessible, and cost-effective approach to pre-operative planning in THA that maintains high accuracy standards in the digital imaging era.
Accurate pre-operative planning for total hip arthroplasty can be effectively achieved using acetate templating on calibrated digital radiographs, providing a reliable and affordable alternative to digital software without compromising surgical precision or outcomes.
References
- 1. Sloan M, Premkumar A, Sheth NP. Projected volume of primary total joint arthroplasty in the U.S., 2014 to 2030. J Bone Joint Surg Am 2018;100:1455-60. [Google Scholar] [PubMed]
- 2. Bourne RB, Rorabeck CH. Soft tissue balancing: The hip. J Arthroplasty 2002;17 4 Suppl 1:17-22. [Google Scholar] [PubMed]
- 3. Barrack RL. Preoperative planning for revision total hip arthroplasty. Clin Orthop Relat Res 2004;420:32-8. [Google Scholar] [PubMed]
- 4. Bono JV. Digital templating in total hip arthroplasty. J Bone Joint Surg Am 2004;86-A Suppl 2:118-22. [Google Scholar] [PubMed]
- 5. Lecerf G, Fessy MH, Philippot R, Massin P, Giraud F, Flecher X, et al. Femoral offset: Anatomical concept, definition, assessment, implications for preoperative templating and hip arthroplasty. Orthop Traumatol Surg Res 2009;95:210-9. [Google Scholar] [PubMed]
- 6. Unnanuntana A, Wagner D, Goodman SB. The accuracy of preoperative templating in cementless total hip arthroplasty. J Arthroplasty 2009;24:180-6. [Google Scholar] [PubMed]
- 7. Suh KT, Cheon SJ, Kim DW. Comparison of preoperative templating with postoperative assessment in cementless total hip arthroplasty. Acta Orthop Scand 2004;75:40-4. [Google Scholar] [PubMed]
- 8. Crooijmans HJ, Laumen AM, Van Pul C, Van Mourik JB. A new digital preoperative planning method for total hip arthroplasties. Clin Orthop Relat Res 2009;467:909-16. [Google Scholar] [PubMed]
- 9. Sinclair VF, Wilson J, Jain NP, Knowles D. Assessment of accuracy of marker ball placement in pre-operative templating for total hip arthroplasty. J Arthroplasty 2014;29:1658-60. [Google Scholar] [PubMed]
- 10. Gamble P, De Beer J, Petruccelli D, Winemaker M. The accuracy of digital templating in uncemented total hip arthroplasty. J Arthroplasty 2010;25:529-32. [Google Scholar] [PubMed]
- 11. Bertz A, Indrekvam K, Ahmed M, Englund E, Sayed-Noor AS. Validity and reliability of preoperative templating in total hip arthroplasty using a digital templating system. Skeletal Radiol 2012;41:1245-9. [Google Scholar] [PubMed]
- 12. Goyal T, Sethy SS, Ansari S, Das L, Paul S. Use of acetate templates over digital radiographs for templating in total hip arthroplasty: Technique and its validation. Indian J Orthop 2020;55 Suppl 1:81-7. [Google Scholar] [PubMed]
- 13. Krishnamoorthy VP, Perumal R, Daniel AJ, Poonnoose PM. Accuracy of templating the acetabular cup size in total hip replacement using conventional acetate templates on digital radiographs. J Clin Orthop Trauma 2015;6:215-9. [Google Scholar] [PubMed]
- 14. O’Sullivan M, Tai CC, Richards S, Skyrme AD, Walter WL, Walter WK. Iliopsoas tendonitis a complication after total hip arthroplasty. J Arthroplasty 2007;22:166-70. [Google Scholar] [PubMed]
- 15. Shin JK, Son SM, Kim TW, Shin WC, Lee JS, Suh KT. Accuracy and reliability of preoperative on-screen templating using digital radiographs for total hip arthroplasty. Hip Pelvis 2016;28:201-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes
December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes July 1, 2025 Metal Mesh Saved The Joint In Primary Hip Arthroplasty In Low Low-Resource Setting
July 1, 2025 Metal Mesh Saved The Joint In Primary Hip Arthroplasty In Low Low-Resource Setting August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience
August 1, 2026 The Forgotten Joint and Forgotten Spine: Recalibrating Success around the Patient’s Experience August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty